
記住我
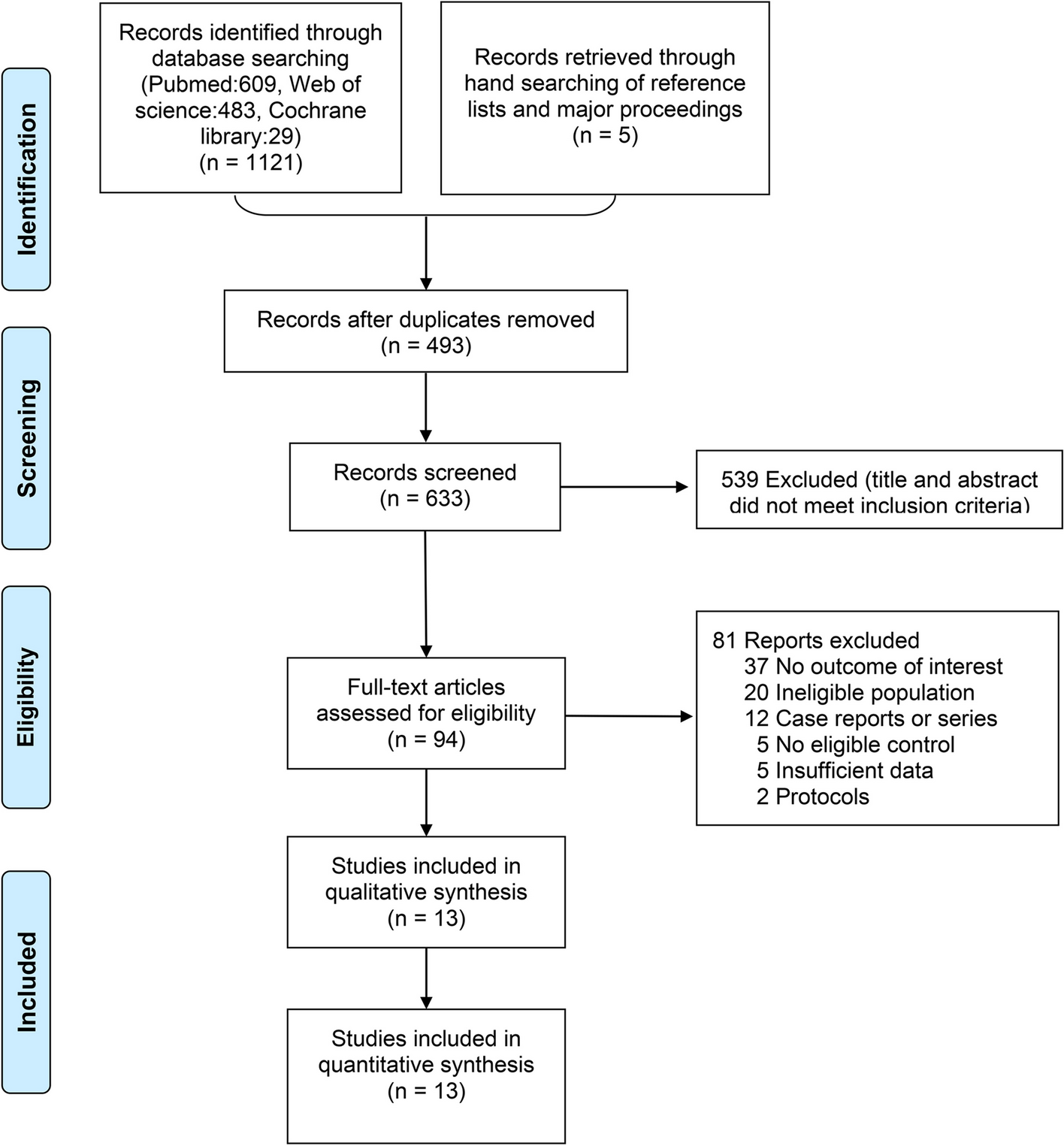



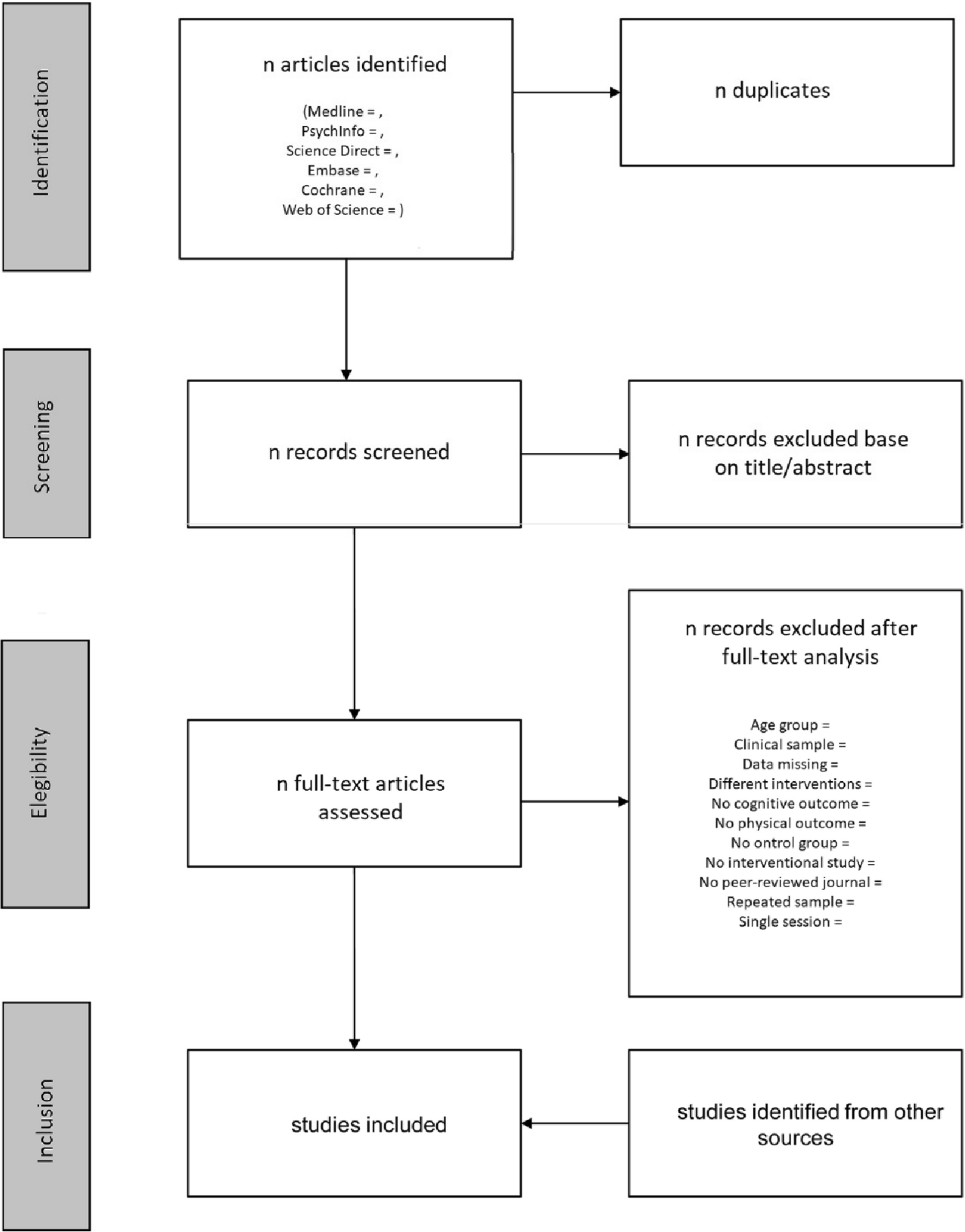


The database search identified 7552 studies after removal of 2401 duplicates. Following the first stage of screening (title and abstract), 88 full texts were screened to identify eligible studies for final inclusion. A further 75 studies were excluded at the second stage of screening (full text), mainly because the studies were not assessing any causation or relationship, not both the interested conditions were explored, or because of non-peer-reviewed publications such as conference proceedings, commentaries, and research notes. Thirteen studies [6,7,8,9, 12, 16,17,18,19,20,21,22,23] were therefore included into the final analysis of the current review (Table 1) (Fig. 1).
Table 1 Description of eligible studiesFig. 1
The included studies were conducted in eight countries (Korea, Taiwan, Japan, Canada, Australia, Netherland, Kansas, and China) involving in 4976 participants. Outcome measures assessed were related to the knee were pain, disability, knee range of motion (ROM), and KOA severity grades. There were seven studies assessing biomechanical associations [9, 16, 18,19,20, 22, 23] and 10 of studies assessing clinical outcomes [6,7,8, 12, 16,17,18, 21,22,23]. There were six studies evaluating the outcomes related to knee pain and disability [7, 8, 17, 18, 20, 23] (Table 2), six studies evaluating the outcomes related to back pain and disability [6, 8, 17, 18, 21, 22], one study measuring the knee flexion angle [20], the spinal ROM [18], and one study evaluating the knee OA severity [22] (Table 2).
Table 2 Biomechanical causations/relationships between LBP and knee OA Association between LBP and KOABiomechanical associations Spinopelvic alignmentThere were seven studies that have investigated biomechanical measures such as specific angles and alignment of the bones in relation to LBP and KOA in the literature. Development and progression of KOA in degenerative spondylolisthesis (DS) patients may be induced by significantly greater mismatches of lumbo-pelvic sagittal alignment [19]. Rate of double adjacent level of spondylolisthesis (condition in which a vertebral body shifts forward with an intact neural arch, compared to the vertebral body beneath it [24] in KOA group and non-KOA group) was 33.3% and 18.1%, respectively [19]. As a result of significantly greater PI (mean ± SD, 58.0° ± 10.4) and pelvic tilt (PT) (27.2° ± 9.8), double adjacent level spondylolisthesis with greater pelvic incidence-lumbar lordosis (PI-LL) (30.6 ± 10.0) is dominant in KOA patients with DS than patients without KOA. This shows that these factors are responsible in complicating KOA in patients with DS [19]. Elderly patients with degenerative lumbar spondylolisthesis (DLS) and severe KOA reported a different pelvic morphology than in patients with no to mild and moderate KOA [20]. They also presented with an increased sagittal malalignment and a lack of lumbar lordosis due to the double-level listhesis and greater knee flexion (mean ± SD, 10.1° ± 5.3) contracture. Parameters in lumbo-pelvic sagittal alignment is as follows: PT, LL, PI-LL, and SS of KOA group and non-KOA group were mean ± SD, 27.2° ± 9.8 and 22.2° ± 8.6, 40.4° ± 15.8 and 42.6° ± 14.3, 17.9° ± 15.1 and 10.3° ± 12.9, and 30.6° ± 10.0 and 30.6° ± 8.9, respectively. A greater pelvic retroversion (mean ± SD, 34.1° ± 10.8) may have activated in these patients as a compensatory mechanism [20]. Severe OA exhibited a significantly greater (mean ± SD, 56.7° ± 8.7) (p = 0.05) pelvic incidence (the angle between the line perpendicular to the sacral end plate at its midpoint and a line connecting this point to the axis of the femoral head), pelvic tilt, and knee flexion angle (KFA), along with a smaller degree (mean ± SD, 34.9° ± 14.6) of lumbar lordosis than in the mild-OA group (p = 0.26) [20].
Rate of radiographic adjacent-segment disease (ASD) (which is a condition with encompassing many complications of spinal fusion, including listhesis, instability, herniated nucleus pulposus, stenosis, hypertrophic facet arthritis, scoliosis, and vertebral compression fracture [25]) was observed to be higher in the severe OA group than in the mild OA group (38%) (p = 0.02) [20]. Patients with ASD in severe OA exhibited significantly greater PT (mean ± SD, 26.2° ± 7.0), along with less LL (38.7° ± 12.2), than the patients without ASD (p < 0.05). High PI (58.3°) is a risk factor for development of spondylolisthesis and KOA [16]. The incidence of knee OA was higher in individuals with a high PI (58.3°) compared to low PI (49.5°) (p = 0.03).
A significantly greater pelvic anterior tilt (44.68°) angle was found in the patients with KOA of both the LBP and non-LBP groups compared to healthy people without KOA or LBP [18]. There was no significant difference in anterior trunk inclination angle or sagittal alignment between KOA patients with and without LBP [9]. The sagittal alignment of spine-pelvis-lower extremity axis was significantly influenced by severe KOA [9]. The lumbar spine is served as the primary source of compensation, while hip flexion and pelvic anteversion increased for further compensation [9]. Changes in sagittal alignment may not be involved in the pathogenesis of LBP in this patient population [9]. Patients with severe KOA showed significant backward femoral inclination (FI), hip flexion, and forward spinal inclination (p < 0.001) compared with controls (without KOA) [9]. In addition, patients with FI of 10° showed reduced lumbar lordosis and significant forward spinal inclination compared with controls, whereas those with FI > 10° presented with significant pelvic anteversion and hip flexion [9]. Individuals over 50 years of age with severe KOA reported to have a poor lumbo-pelvic sagittal alignment [22]. Severity of KOA found to be related to lumbo-pelvic sagittal alignment; however, it does not relate to the global spinal balance [22]. KOA was found to be strongly related with the pelvic retroversion [22]. This pelvic retroversion may lead the progression of KOA [22]. Vice versa, knee joint degeneration may affect the pelvic retroversion [22]. According to kinematic chain reaction, pelvic retroversion is related to hip external rotation and varus knee deformity in standing position [22]. Varus knee alignment increases the medial tibiofemoral load and is associated with knee osteoarthritis [22]. Thus, sagittal lumbo-pelvic malalignment, especially pelvic retroversion, could lead to the progression of KOA. Furthermore, lumbar kyphosis in women was found to be associated with a lower Knee Society Knee Scoring System (KSS) symptom score [23].
Range of motion (ROM)Both knee and spinal ROM were measured in relation to LBP and KOA. The knee flexion angle on the ipsilateral side bent to pick up was significantly smaller in both KOA groups (median with LBP — 9.11° and without LBP — 8.99°) than in the controls (median without KOA and LBP 15.45°) in the downward reach and pickup movements [18].
The patients with KOA in the LBP and non-LBP groups showed significantly smaller (median: with LBP = −27.65°; non-LBP = −27.44°) trunk flexion angles than that of the controls (without KOA or LBP, median = −40.43°), and the rotation angle of the non-LBP group was smaller (median = 6.01°) than that of the controls (9.15°) [18].
Clinical characteristicsAlmost every clinical measure was worse among those who report back pain, including Health Assessment Questionnaire disability, pain, global severity, fatigue, and psychological status in people with KOA [6]. Pain and functional disability were commonly investigated in relation to LBP and KOA in the previous literature Table 3.
Table 3 Clinical causations/relationships between LBP and knee OAPain in concurrent LBP and KOABack pain is strongly associated with knee pain [6]. Compared to the primary KOA patients with mild LBP, patients with severe LBP had significantly poorer Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score [17]. Roland-Morris Disability Questionnaire (RDQ) and Oswestry Disability Index (ODI) pain scores were higher (median = 9, non-LBP = 3.5) in the LBP group with KOA [18]. LBP was significantly associated with increased WOMAC knee pain score (p < 0.01) [7]. Although mild LBP was not associated with WOMAC knee pain score, moderate and severe LBP were each associated with substantially higher (95% CI = −11.6) WOMAC knee pain scores [17]. Knee pain intensity with LBP was higher (β: 0.62; 95% CI: 0.51 to 0.73) than in those without LBP (β: 0.40; 95% CI: 0.32 to 0.49) in individuals with LBP compared to no LBP in KOA [8]. There was another study to support no association between LBP and pain in KOA [12].
Functional disability in concurrent LBP and KOALBP interacts with knee pain intensity and contributes to the disability level in individuals with KOA [8]. Coexisting LBP and knee pain had a stronger impact on disability level than in individuals with LBP than in those without LBP [8]. The presence of LBP was associated with increased disability level (with LBP (β: 0.62; 95% CI: 0.51 to 0.73) than in those without LBP (β: 0.40; 95% CI: 0.32 to 0.48)), and relationship between knee pain intensity and disability level was higher in individuals with LBP than in those without LBP [8]. More severe lumbar spine symptoms (visual analogue scale (VAS score ≥ 7)) were likely to adversely affect the WOMAC physical component summary and mental component summary scores of the SF-36 among patients with advanced KO [17]. In addition, a moderate lumbar spine symptom grade was associated with a poorer WOMAC function score [8].
ODQ and ODI scores were higher (11 and 9, respectively) in people with concurrent LBP and KOA [2, 8]. Moreover, the progression severity of KOA had more impact on stronger relationship with disability-related LBP in women than in men [22]. In women, the ODI score in people with severe OA was worse compared to that in mild OA [22].
Both LBP and lumbar kyphosis are useful clinical signals and indicate functional disability and knee symptoms in patients with knee OA [23]. LBP and lumbar kyphosis were independently associated with a lower KSS function score [23]. The coexistence of LBP and lumbar kyphosis in women was associated with a lower KSS symptom score [23].
There is evidence to support for having no clinical relationship between these two conditions. LBP was not associated with disability in individuals with KOA (p = 0.998) [12]. There was no statistically significant difference in the Lequesne’s index scores between the LBP and non-LBP groups with KOA [18]. ODI score and corresponding back pain disability among KOA patients indicated none or minimal disability in another study [21]. Patients with end-stage KOA were more likely to experience none or very mild LBP, with minimal disability due to back pain based on ODI score.
Quality of the included studiesFigure 2 reveals the overall assessment of the quality of the included studies. Out of 14 items of the quality assessment, 6 criteria were adequately addressed by all the included studies. They have clearly described the objectives and study population and had a rate of ≥ 50% eligible persons, reliable and valid exposure measures and outcome measures, sufficient timeframe, and sufficient follow-up rate. However, sample size justification, power description, or variance and effect estimates should be clearly indicated in the methods (Fig. 2).
Fig. 2
Quality assessment of the included studies
留言 (0)