Bayesian network meta-analysis will be carried out. This protocol is reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) [27], and the checklist is presented in online Supplementary Appendix 1. This network meta-analysis will be reported in accordance with PRISMA extension version (PRISMA-NMA) [28]. This study protocol has been registered on the international prospective register of systematic review (INPLASY2020110067).
Search strategy
We will perform electronic search until December 2022 in the following databases: PubMed, Embase, Cochrane Library, and Web of Science. We will also search ClinicalTrials.gov, WHO International Clinical Trials Registry Platform (ICTRP), and International Standard Randomized Controlled Trial Number Registry for all registered clinical trials and randomized controlled trials. Furthermore, we will search the gray literature in Google Scholar, OpenGrey, and ProQuest Dissertation. The reference lists of articles and relevant systematic reviews will be tracked to identify other relevant studies. No restrictions on language will be set. If we find more relevant key words during our primary search, we will modify the search syntax. All searches will be updated before submitting the review.
The PubMed search strategies are as follows:
#1 “Ductus Arteriosus, Patent” [MeSH Terms]
#2 “patent ductus arteriosus” [Title/Abstract]
#3 #1 OR #2
#4 "Thoracic Surgery, Video-Assisted "[MeSH Terms] OR "video-assisted thoracoscopic
surgery"[Title/Abstract] OR "Minimally Invasive Surgical Procedures"[MeSH Terms] OR "minimally invasive"[Title/Abstract] OR "Minimal Access Surgical Procedures"[Title/Abstract] OR "mini-invasive"[Title/Abstract] OR "minimal surgical procedure*"[Title/Abstract] OR "Surgical ligation"[Title/Abstract] OR "surgical closure"[Title/Abstract] OR "Transthoracic"[Title/Abstract] OR "transcatheter"[Title/Abstract] OR "percutaneous closure"[Title/Abstract] OR "pharmacological"[Title/Abstract] OR "Cyclooxygenase Inhibitors"[MeSH Terms] OR "acetaminophen"[MeSH Terms] OR "COXI"[Title/Abstract] OR "Indomethacin"[Title/Abstract] OR "indometacin"[Title/Abstract] OR "indocid"[Title/Abstract] OR "ibuprofen"[Title/Abstract] OR "brufen"[Title/Abstract] OR "motrin"[Title/Abstract] OR "paracetamol"[Title/Abstract]. #5 #3 AND #4
Eligibility and exclusion criteriaEligibility criteria
1) Types of study: We will include randomized controlled trials. The number of cases included in each group must be greater than ten. Retrospective cohort studies, prospective cohort studies, case–control studies, and case series will not be included.
2) Types of participants: PDA children were confirmed clinically and by transthoracic echocardiography and scheduled for pharmacological treatment, surgical closure of PDA, or interventional closure. There were no restrictions in children weight and age. PDA diameter ranged from 2 to 5.5 mm.
3) Types of interventions: Pharmacological treatment (acetaminophen, indomethacin, or ibuprofen), mini-thoracotomy, VATS, fluoroscopy-guided transfemoral venin and artery of percutaneous closure, fluoroscopy combined with TTE-guided transfemoral venin and artery of percutaneous closure, TTE-guided transfemoral artery of percutaneous closure, and TTE-guided transfemoral vein of percutaneous closure.
4) Types of comparison groups: Surgical ligation for surgical interventions and placebo for pharmacological treatment. If there are head-to-head studies, these studies which compare surgical ligation with other mini-invasive treatments, treatment between different medicines, or pharmacological with surgical treatments will be included.
5) Types of outcomes.
The primary outcomes include the following: primary PDA closure (defined as echocardiography-confirmed closure of PDA after the first course of the treatment), overall PDA closure (defined as echocardiography-confirmed closure of PDA after one or more courses of the treatment), and technical success (defined as patient leaving the procedure room (catheterization laboratory or appropriate alternative) with a device or coil in the PDA. Cases were also considered successful in the event of coil/device embolization that was retrieved during the same procedure, and the PDA was closed with a different size of device/coil.)
The secondary outcomes include the following: mean days/hours needed for closure of PDA, surgical success rate, mortality during hospital stay, operation time, intraoperative radiation dose, radiation exposure time, total postoperative complication rate, postoperative major complication rate, intensive care unit stay, total hospital stays, postoperative hospital stays, and total cost.
Exclusion criteria
1)
Children were diagnosed with other congenital heart diseases (such as ventricular septal defect or atrial septal defect).
2)
Those studies which assessed the change of cardiac function and cardiac physiology changes after PDA treatment
3)
No treatment (conservative management)
Selection of studies
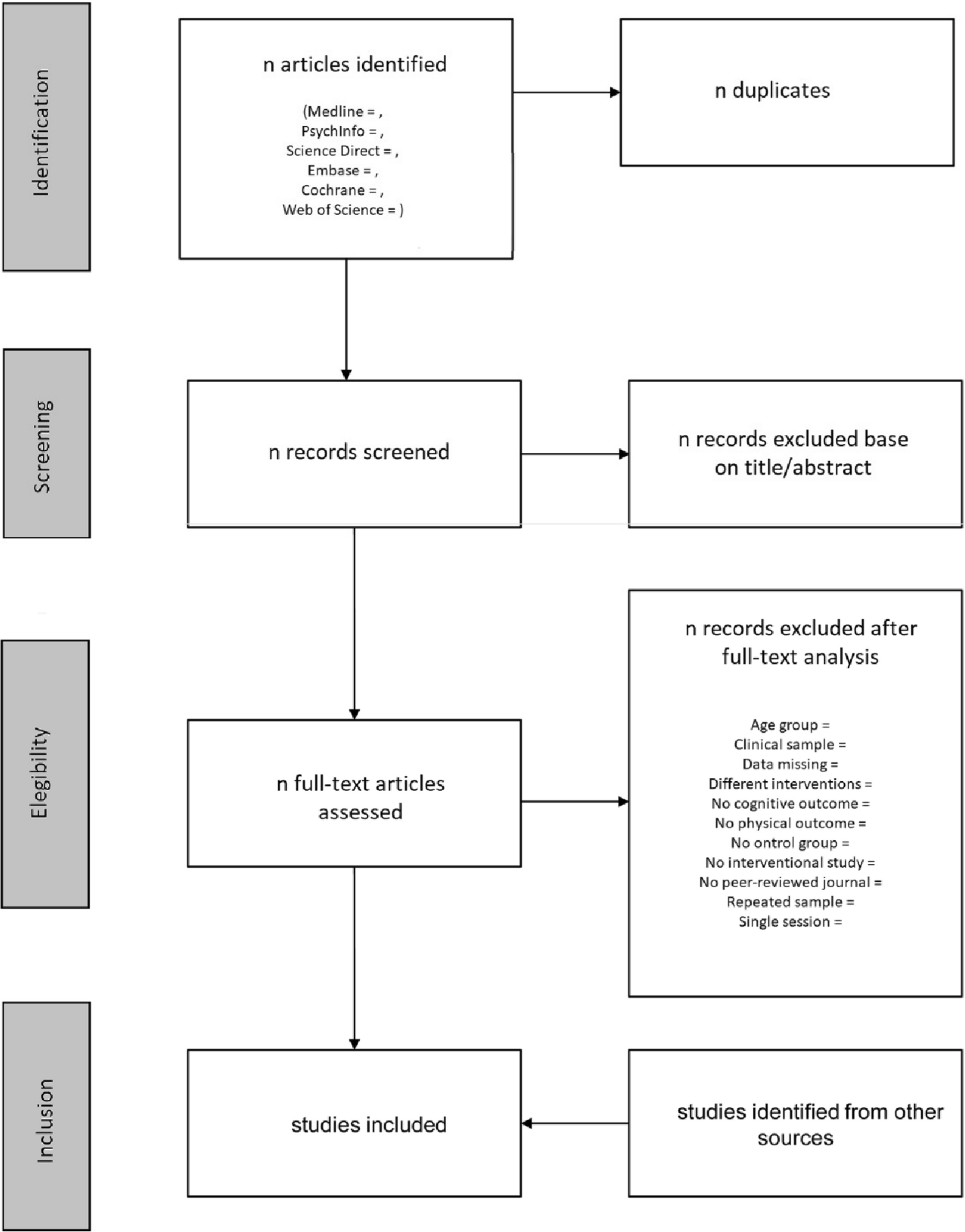
Literature search records will be imported into EndNote X8.1 (Thomson Reuters (Scientific) LLC Philadelphia, PA, USA) software. First, the EndNote X8.1 will be used to exclude duplicate articles, and then, two reviewers will independently screen the titles and abstracts and exclude the articles that do not fulfill the inclusion criteria. If it is hard to judge, full texts will be retrieved. After then, two reviewers will cross-check whether the final selected research is consistent. If there are any disagreements between two reviewers during the selection of eligible studies, a third reviewer will involve resolving the disagreements.
Data extraction
A standard data abstraction form will be created using Microsoft Excel 2019 (Microsoft, Redmond, WA, USA, www.microsoft.com). Then, two independent reviewers will extract the basic characteristics and the data of outcomes. The extracted data will include the following: authors, gender, age, birthweight, year of publication, study design, inclusion criteria, medicine dosing protocol, sample size, primary closure rate, reopening rate, mortality, intraventricular hemorrhage (IVH all grades), necrotizing enterocolitis (NEC all grades), pulmonary hemorrhage (blood-stained liquid flowing from the trachea of the infant), bronchopulmonary dysplasia, retinopathy of prematurity, renal dysfunction, hepatic dysfunction, gastrointestinal bleeding, treatment methods, device used, median follow-up, PDA diameter, etc. If there is a discrepancy between the two reviewers, a third researcher will be consulted. We will randomly select five to ten studies to check the completeness of the data abstraction form. The data abstraction form will be complemented by the pilot trial. We will contact the corresponding author to query information when the essential data are insufficient or missing in the original study through sending an email. Studies will be excluded if we are unable to get access to the data, and the reasons for exclusion will be reported in detail.
Risk-of-bias assessment
Randomized controlled trials will be assessed using the Cochrane Handbook’s Risk of Bias (ROB) assessment tool [29]. Studies will be reviewed and scored as “high risk,” “low risk,” or “unclear” in each of the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. Inter-rater reliability of the ROB tool has been demonstrated to range from fair to substantial depending on the assessment domain [24]. The risk of bias will be assessed by two independent reviewers, and conflicts will be resolved by a third reviewer.
Geometry of the network
A network plot will be created to describe and present the geometry of the treatment network of comparisons across trials using STATA (16.0; Stata Corporation, College Station, TX, USA). If the trial is not linked by treatments, we will exclude it from network meta-analysis and just describe the findings of the study.
In the network plot, nodes represent different interventions, and edges represent a head-to-head comparison between interventions. The size of the nodes and the thickness of the edges are associated with the sample size of the intervention and the number of trials included, respectively.
For pharmacological treatment, a network will be created. The pharmacological treatment includes acetaminophen, indomethacin, and ibuprofen. For surgical treatment, the network includes surgical ligation, mini-thoracotomy, VATS, and interventional therapy. Finally, a network of pharmacological and surgical treatment will be created if possible.
Statistical analysis and data synthesisPairwise meta-analysis
We will use Review Manager 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) statistical analysis software for pairwise meta‐analysis. For dichotomous outcomes, the combined results will be calculated as odds ratios (ORs) and 95% confidence intervals (CIs). For continuous outcomes, we will calculate and meta-analyze mean differences (MD) or standardized mean differences (SMD) and their 95% CIs. We will use the Cochran’s Q-test and I2 statistics to assess and report heterogeneity. When I2 ≤ 40%, the heterogeneity is considered acceptable, and the fixed-effects model is used for the combined analysis. If I2 > 40%, the heterogeneity is considered to be large, and the source of heterogeneity will be explored. Sensitivity analysis, subgroup analysis, and meta-regression will be used to find the source of heterogeneity. Meanwhile, the clinical and methodological heterogeneity across studies will be reassessed. If no proper reasons will be found for high heterogeneity, the random effects model will be used to incorporate the heterogeneity. P < 0.05 was considered as statistically significant.
Network meta-analysis
Network meta-analysis will be conducted using a Bayesian Markov chain Monte Carlo (MCMC) framework. We will use the generalized linear modelling framework for network meta-analysis of randomized controlled trials. The convergence will be assessed using the Brooks-Gelman-Rubin (BGR) plots method. Both random and fixed models will be used. And the best model will be chosen based on the deviance information criterion (DIC) values. The model with lowest DIC value is usually selected because it is considered in most cases to be the most reliable. Transitivity is a key assumption of NMA and refers to the belief that an indirect comparison is a valid estimate of the unobserved direct comparison [30, 31]. The node splitting method will be used to examine the transitivity between direct and indirect comparisons if a loop connecting three or more arms exist [32]. If node-splitting analysis determined P < 0.05, the inconsistency model will be used for pooled analysis. Meanwhile, the consistency model will be used [33, 34]. The network meta-analysis results using inconsistency and consistency model will be compared. If the results using inconsistence and consistence model are not compared or there are any inconsistences between direct and indirect results, subgroup analysis, sensitivity analysis, or meta-regression will be used to find the source of inconsistence will be also used. Besides, we will rank all included interventions in terms of probability. The rank and probabilities of each intervention will be shown using surface under the cumulative ranking curve (SUCRA) and ranking plots (rank probability — rank curve). SUCRA is a numeric presentation of the overall ranking and presents a single number, ranging from 0 to 1, associated with each treatment [35]. If the SUCRA value of a certain intervention is close to 1, it is always ranked first, and if it is close to 0, it is always ranked last [36]. The MCMC simulation will be implemented using the R software (gemtc and pcnetmeta packages) (V.4.1.0) (http://cran.r-project.org/) with interfacing to OpenBUGS (V.3.2.3, MRC Biostatistics Unit, Cambridge, UK) (http://www.openbugs.net/w/Downloads) [37,38,39].
Subgroup analysis
According to the instrument to assess the Credibility of Effect Modification Analyses (ICEMAN) tool [40], subgroup analyses will be performed according to the following factors:
1.
Participant characteristics (e.g., sex, age)
2.
Study-specific factors are as follows:
(a) Sample size
(b) Overall study quality
(c) Risk of bias (e.g., all studies versus low bias studies only)
Assessment of publication bias
The funnel plot and Egger test will be conducted to detect publication bias if the number of studies was more than ten.
Quality of evidence
We will assess the quality of the evidence by following the steps to assess the quality of treatment effect estimates for network meta-analysis as per the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) [41] approach. The GRADE approach will assess five domains including study limitations, consistency of effect, imprecision, indirectness, and publication bias to assess the quality of the body of evidence for each outcome. We will use the following four steps to assess the quality of treatment effect estimates from NMA. Firstly, present direct and indirect treatment estimates for each comparison of the evidence network. Secondly, rate the quality of each direct and indirect effect estimate. In addition, present the NMA estimate for each comparison of the evidence network. Meanwhile, conceptual advances will be applied ((1) consideration of imprecision is not necessary when rating the direct and indirect estimates to inform the rating of NMA estimates, (2) there is no need to rate the indirect evidence when the certainty of the direct evidence is high and the contribution of the direct evidence to the network estimate is at least as great as that of the indirect evidence, (3) not trust a statistical test of global incoherence of the network to assess incoherence at the pairwise comparison level) [42]. Finally, rate the quality of each NMA effect estimate. It is classified into four levels: high level, moderate level, low level, and very low level.
Sensitivity analysis
We will perform a sensitivity analysis to verify the robustness of the study results. This will be achieved by assessing the impact of the sample size, high risk of bias, missing data, and selected models. Following the analyses, if the quality of a study is judged to be low, it will be removed to ensure the robustness of the results.
Ethics and dissemination
Ethical approvals and patient consent are not required because this is a network meta-analysis based on published trials. The findings of this project will provide a general review and evidence of the efficacy and safety of pharmacological treatment, surgical ligation, mini-thoracotomy, VATS, fluoroscopy-guided transfemoral venin and artery of percutaneous closure, fluoroscopy combined with TTE-guided transfemoral venin and artery of percutaneous closure, TTE-guided transfemoral artery of percutaneous closure, and TTE-guided transfemoral vein of percutaneous closure for PDA in children. The results will be submitted to a peer-reviewed journal for publication. We hope that these findings will help clinicians and patients choose a more appropriate repair method for PDA.






留言 (0)