
記住我
KEY POINTS
Question: Is socioeconomic status associated with outcomes in critical care?
Findings: Lower socioeconomic status is associated with higher mortality in critical care and may impact length of stay and discharge destination.
Meanings: Care providers should be aware that socioeconomic status influences outcomes in critical care, and health policy should consider how critical care provision may help to mitigate these health inequalities.
Socioeconomic status is a well-established determinant of inequality in health outcomes. This is mediated by both patient and healthcare factors including comorbidities, health beliefs, stage of disease presentation, likelihood of referral, and threshold for intervention (1,2). Since critical care units deliver urgent care based on severity of disease, some of these factors, particularly those related to chronic disease, may be less relevant in this environment.
Existing literature examining the impact of socioeconomic status on outcomes in critical care has produced inconsistent findings. Some studies identified that socioeconomically deprived groups present to critical care with a different spectrum of disease compared with less deprived groups (3) or that outcomes for these groups differ by source of admission (4). A mixed picture exists on how socioeconomic status influences critical care mortality. Current literature varyingly reports either no difference in outcomes or worse outcomes in the most deprived patients (5–7). Therefore, a systematic review and meta-analysis were undertaken to collate the available evidence, appraise its quality and, for the first time, derive a pooled estimate of the association between socioeconomic status and short-term mortality and length of stay in critical care.
MATERIALS AND METHODSThe review was conducted in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews and meta-analyses (8).
Search Strategy and Study SelectionThe CINAHL, MEDLINE, and EMBASE databases were searched for eligible studies, published in English, using search terms (including synonyms) for intensive care and socioeconomic factors. The final search was conducted on September 13, 2022.
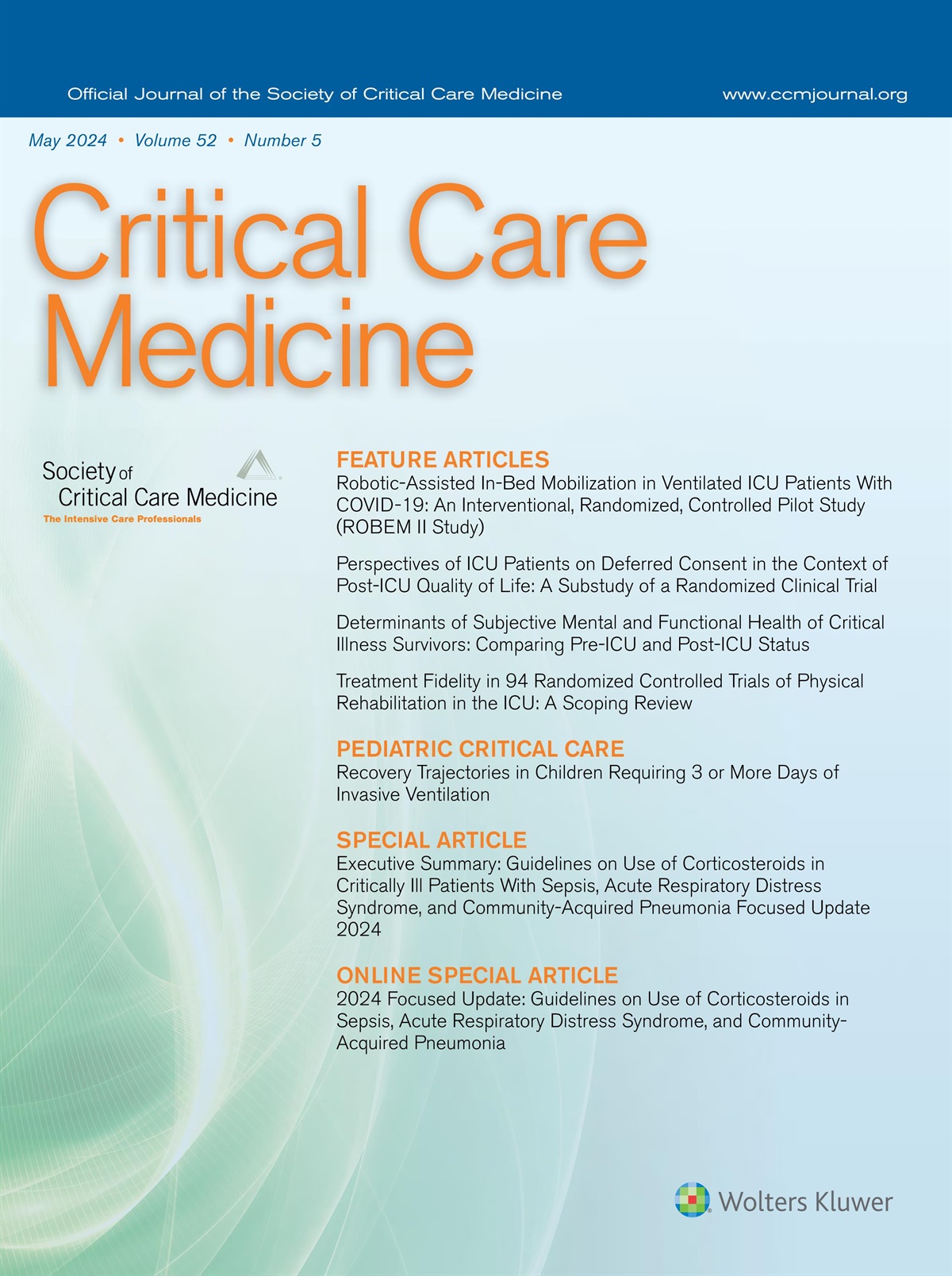
Studies were eligible if they included an adult patient population admitted to a critical or ICU, used education, income, occupation, housing or an index including one of these as a measurement of socioeconomic status as an exposure variable, and reported association between this exposure and any patient outcome (Table 1). The full search strategy is reported in the Supplementary Appendix (https://links.lww.com/CCM/H267). Studies were included even if they only reported a subset of the critical care population—for example, studies with disease-specific inclusion criteria. Studies using hospital type, race, and/or health insurance status as a marker of socioeconomic status without other indicators were excluded due to concern that they may limit generalizability across healthcare systems or locations. No restrictions were placed on geographical location, study design, or year of publication. Where multiple eligible studies considered different groups or outcomes within the same cohort, all were considered in the systematic review.
TABLE 1. - Inclusion and Exclusion Criteria for Systematic Review Search Strategy and Article Selection Category Inclusion Exclusion Population Adult patients admitted to critical, or intensive, care units Studies reporting mixed admissions to both critical care and general hospital settings Exposure One or more marker of socioeconomic status as income, education, employment, housing or a composite index including one or more of these variables Only hospital type, race, and/or insurance status as markers of socioeconomic status Outcome Any patient outcomes including mortality, disease severity, quality of life, risk of admission or disease, or access to services No patient outcomes reported No association between socioeconomic status and outcome(s) reported Reporting English language Worldwide No restriction by publication yearTitles and abstracts were assessed independently by two authors (R.D.M., C.E.J.M.) according to the inclusion and exclusion criteria, with potentially eligible full-text articles retrieved and reviewed. Citation tracking, by manual checking of the reference lists of included studies and previous systematic reviews, was used to identify potentially eligible articles not identified in this search. Where full-text articles for potentially eligible citations were unavailable, authors were contacted.
Data ExtractionData on the study design, sample size, study population characteristics, years of recruitment, country/countries in which the study was conducted, exposure and outcome measures used, length of follow-up, adjustment for confounding, and effect size estimates were extracted from eligible manuscripts. Where required, ratios were recalculated to ensure consistent comparison of most to least deprived group. Where a single article reported multiple comparisons for multiple levels of deprivation, the comparison of the most and least deprived groups was used. If effect sizes were presented in smaller increments, for example, in percentage point increments of area-level postsecondary education, representative groups were chosen from the median of quintiles one and five, or the limits of the interquartile range. Where effect sizes were not reported, unadjusted odds ratios (ORs) were calculated from the available data (9). Adjusted estimates were reported in preference to crude. Where analyses used different levels of adjustment, the model adjusted for the highest number of confounders was used. The Newcastle-Ottawa Scale was used to assess the quality of eligible studies (10).
Meta-AnalysisMeta-analysis was undertaken of studies that reported mortality up to 30 days following ICU admission and those that reported median length of stay and interquartile ranges across socioeconomic groups. These included the most commonly reported outcomes and reflected mortality related to the index critical illness. Where studies reported mortality at several time points, the longest follow-up, up to 30 days was used. Where studies reported ICU or in-hospital mortality alongside 30-day mortality, the latter was used for meta-analysis. Studies reporting insufficient data (e.g., absence of precision measures) were excluded from meta-analysis. Due to low event rates and short-term time-defined reporting of outcomes for mortality, ORs and hazard ratios (HRs) were pooled for meta-analysis as ORs. Studies solely reporting a subset of another study were excluded from the meta-analysis. Where studies reported the effect of more than one individual-level measure of socioeconomic status, only one was included—with education prioritized above a descending hierarchy through income, occupation and housing, in keeping with previous studies (11).
Statistical AnalysisMeta-analysis of eligible studies was conducted using an inverse-variance random-effects model with Paule-Mandel estimator. Between-study statistical heterogeneity was assessed using I2. For mortality, pooled ORs were calculated, and for ICU length of stay, the pooled difference of medians were estimated, each with 95% CIs. Post hoc subgroup meta-analysis for mortality, including only studies that adjusted for confounders, was conducted using the same methodology. Funnel plots were constructed to visualize small-study effects and Egger test used to describe asymmetry. Meta-regression was used to explore possible causes of heterogeneity between studies reporting mortality, with year of publication, and population size as continuous variables, and continent of study, type of socioeconomic indicator (area- or individual-level), adjustment for confounders, and measure of effect size (HR or OR) as categorical variables, defined a priori and incorporated into a single model. Influence analysis using leave-one-out methodology was used to evaluate the impact of individual studies and assess robustness of the pooled effect estimate (12). All analyses were conducted using the meta, metafor, and metamedian packages in R (13–16).
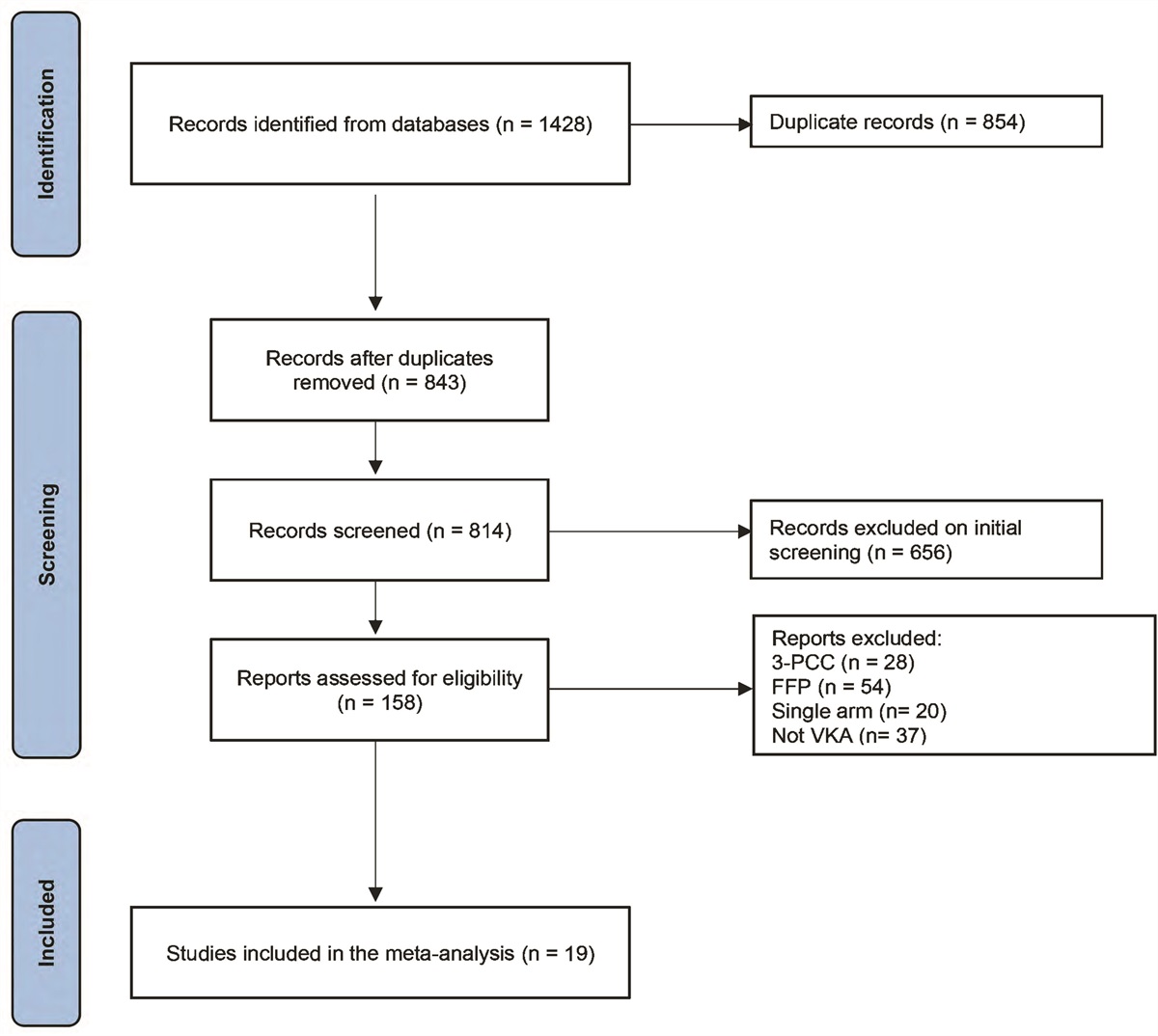
RESULTSCINAHL identified 738 potentially eligible publications, Medline 1,187 and EMBASE 2,136 (Supplementary Fig. 1, https://links.lww.com/CCM/H267). Following exclusion of 1,107 duplicate publications, 2,932 were reviewed for eligibility. Of these, 30 articles met all the inclusion criteria. An additional 11 potentially eligible articles were identified by citation tracking, eight of which met the inclusion criteria, resulting in 38 eligible studies.
Four studies reported a patient group or varying analysis of the same cohort included in other articles (17–24). The additional outcomes these reported were considered for systematic review. One article screened, but excluded, was a previous systematic review of 10 studies, which focused on longer-term outcomes and quality of life following intensive care (5).
Study CharacteristicsOf the 38 eligible studies, 32 were retrospective cohort studies, four prospective cohort studies (25–28), one a mixed case-control and retrospective cohort study (29), and one a case-control study (30). The majority (n = 33) were published after 2010, of which four reported the impact of the COVID-19 pandemic (17,18,27,29). Most included all admissions to the relevant critical care units, however, some reported outcomes of a specific disease subgroup (21,31–35). There was diversity in the approach to measuring socioeconomic status—most notably its basis on individual-level measures such as educational attainment, income or housing (3,29–31,33,35–41), or area-based measures (4,6,7,17–28,32,34,42–50). The latter included studies using a single measure such as poverty rate in the patient’s census tract (21,22), to studies using indices of multiple deprivation: composite scores derived from up to 39 indicators across several domains (42). Most studies (n = 35) were assessed as good quality; with those rated as fair or poor tending to lack adjustment in their reporting of outcomes relative to socioeconomic exposure (19,38,50). Supplementary Tables 1 and 2 (https://links.lww.com/CCM/H267) give a summary of study characteristics.
Outcomes MortalityThe 33 studies that reported ICU or in-hospital mortality used time points ranging from 30 days up to 365 days and longer. Nine of these studies (27%) reported significantly higher mortality in the more deprived group across all measures and timeframes (4,6,17,18,24,32,42,45,47), while 18 (55%) reported no significant difference in mortality by socioeconomic status regardless of which time point or measure was assessed (7,19–23,27,29,30,32,33,36,37,39,41,43,44,50). One study reported higher in-hospital mortality in areas with greater postsecondary education rates but no difference when area-level unemployment or median income were considered (48). Some studies reported differences in the association by length of follow-up; however, the effect direction was inconsistent. For example, Ho et al (46) reported no significant difference for in-hospital mortality but higher long-term mortality among the most deprived groups. Oh et al (38) found similar outcomes when stratified by occupational status but not when educational measures were used. Conversely, Schnegelsberg et al (31) found significantly higher risk of mortality for lower income groups at 30 days but not 180 days, while the risk using educational or cohabitation measures was not significantly different at either time point. Another study reporting subgroup differences only demonstrated an association between socioeconomic status and in-hospital mortality for patients over 50 years old (3). An obstetric cohort study used the composite outcome of maternal-fetal-neonatal mortality and demonstrated poorer outcomes with fewer years of maternal education (40). Supplementary Table 3 (https://links.lww.com/CCM/H267) demonstrates individual study mortality outcomes.
Meta-Analysis of Short-Term MortalityTwenty-three studies met the criteria for meta-analysis. For less than or equal to 30-day mortality following critical care admission comparing the lowest to the highest socioeconomic status, the pooled OR was 1.13 (95% CI, 1.05–1.22) (Fig. 1). The I2 value of 59% (95% CI, 35–74%) indicated moderate-to-substantial between-study heterogeneity (51).
 Figure 1.:
Figure 1.: Meta-analysis and pooled effect sizes of the association between socioeconomic status and mortality up to 30 d following admission to critical care. OR = odds ratio.
Post hoc subgroup meta-analysis, containing only studies adjusting for potential confounders, demonstrated findings consistent with the planned meta-analysis (Supplementary Fig. 2, https://links.lww.com/CCM/H267). Meta-regression did not identify any study characteristics as important predictors of effect size, with full results available in the Supplementary Appendix (https://links.lww.com/CCM/H267). Sensitivity analysis demonstrated consistent results for both effect size and heterogeneity in leave-one-out analysis (Supplementary Fig. 3, https://links.lww.com/CCM/H267). The Funnel plot demonstrated visual asymmetry (Supplementary Fig. 4, https://links.lww.com/CCM/H267), however, this was not confirmed with Egger test that calculated an intercept of 0.768 (95% CI, –0.27 to 1.81; t = 1.45; p = 0.16).
ICU Length of StayA smaller number of studies (n = 10) reported associations between socioeconomic status and ICU length of stay. Six of these demonstrated longer ICU length of stay among patients of lower socioeconomic status (3,7,23,30,35,45), and four found no significant difference (20,39,41,44).
Meta-Analysis of ICU Length of StayEight studies met the criteria for meta-analysis of ICU length of stay (6,7,18,31,36,39,44,50). No significant difference in length of stay across socioeconomic groups was noted, with pooled median difference for groups of lowest compared with highest socioeconomic status of –0.11 days (95% CI, –0.29 to 0.06 d) (Fig. 2). The I2 value of 45% (95% CI, 0–76%) indicated moderate between-study heterogeneity. Funnel plot and Egger test are illustrated in Supplementary Figure 5 (https://links.lww.com/CCM/H267).
 Figure 2.:
Figure 2.: Meta-analysis and pooled median difference of the association between socioeconomic status and ICU length of stay.
Functional, Social, and Readmission OutcomesThe impact of socioeconomic status on cognitive, physical, and disability indicators was considered in four studies (20,25,26,28). Two studies found that more deprived patients were more likely to be discharged to long-term care (7,39). Four further studies assessed the risk of readmission to critical care according to socioeconomic status (3,30,31,49). Their outcomes are included in Table 2.
TABLE 2. - Table of Nonmortality Outcomes Including Length of Stay, Functional or Social Outcomes, and Hospital or Critical Care Readmission References Outcomes LOS Barwise et al (3) No significant difference in ICU-free days between Q1 and Q2–Q4. Adjusted mean estimate 0.50 (–0.10 to 1.09) relative to Q1 Significantly more adjusted hospital-free days Q2–Q4 0.70 (0.08–1.32) relative to Q1 Garland et al (45) Steady declining ICU LOS with rising SES adjusted test-of-trend by Fisher exact p < 0.0001a Findlay et al (44) No significant difference in length of ICU stay unadjusted t test p = 0.975 Bigé et al (30) Homelessness associated with increased ICU LOS (adjusted means ratio, 1.16 [1.01–1.34]; p = 0.035) and hospital LOS (adjusted means ratio, 1.30 [1.12–1.49]; p = 0.0002) Mullany et al (7) Less advantaged patients had longer ICU stays (Kruskal-Wallis test p = 0.004) and shorter hospital stays (Kruskal-Wallis test p = 0.001)a Gabriel et al (23) Significantly longer adjusted log ICU LOS ratio 1.08 (1.01–1.14) for most deprived decile compared with least deprivedb Significantly longer adjusted log hospital LOS ratio 1.14 (1.07–1.20) for most deprived decile compared with least deprivedb Bastian et al (20) No significant difference in unadjusted ICU or hospital LOS Bein et al (35) Multivariate adjusted LOS ≥ 5 d low to high SES OR 1.50 (0.91–2.46) Quenot et al (39) No significant difference in unadjusted ICU (t test p = 0.557) or in-hospital (t test p = 0.576) LOSa Shippee et al (41) No significant difference in unadjusted LOS for income or education measuresa Functional or social outcomes Falvey et al (28) Living in a disadvantaged area was associated with a 14% increase in disability burden over 12 mo of follow-up; relative risk 1.14 (95% CI, 1.07–1.21) in a multivariate adjusted model Haddad et al (26) Multivariate adjusted significant difference in RBANS score of cognitive function at 3 and 12 mo for “years of education” 3 mo adjusted RBANS global score difference +3.61 p < 0.001 in multivariable linear regression model 12 mo adjusted RBANS global score difference +2.88 p < 0.001 in multivariable linear regression model Multivariate adjusted no significant difference in RBANS score of cognitive function at 3 and 12 mo for “SES index” 3 mo adjusted RBANS global score difference +0.10 p = 0.76 in multivariable linear regression model 12 mo adjusted RBANS global score difference +0.89 p = 0.43 in multivariable linear regression model Griffith et al (25) Multiple linear regression for Medical Outcomes Study Short Form 12 version 2 scores showed lower social deprivation was associated with better Mental Component Score health-related quality of life at 6 mo (β = 1.38 [0.03–2.74]; p = 0.045), but not Physical Component Score, or either when measured at 12 mo Mullany et al (7) More advantaged patients were more likely to be discharged to their own home and to have a postacute care rehabilitation hospital admissiona Quenot et al (39) Among those not resident in nursing home, deprivation associated with entry to nursing home at 3 mo OR 2.69 (1.40–5.17) and at 6 mo after discharge OR 6.06 (2.23–16.43) in multivariate analysis Bastian et al (20) One-yr SF-36 mental component scores nondeprived to deprived 59.3 (IQR, 37–78.1) vs 54.2 (IQR, 37.2–74.5; p = 0.189) One-yr SF-36 physical component scores nondeprived to deprived 54.5 (IQR, 35–78.8) vs 47.5 (IQR, 30–68.8; p = 0.01) One-yr no significant difference in IES-R scale posttraumatic stress disorder symptoms between nondeprived and deprived (p = 0.931) One-yr no significant difference in HADS-D scale for depression symptoms or HADS-A scale for anxiety symptoms between nondeprived and deprived (p = 0.348 and p = 0.899, respectively) Hospital or critical care readmission Bigé et al (30) Homeless patients were more frequently readmitted to the ICU after hospital discharge over the study period (p = 0.00026) Schnegelsberg et al (31) No significant difference in unplanned readmission at ≤ 180 d in Cox proportional hazards model for education level, income or cohabitation category Hua et al (49) For critical care survivors, no significant difference in early (≤ 30 d) rehospitalization HR 1.01 (0.99–1.04), but significantly greater risk of late (> 30 d) rehospitalization HR 1.08 (1.05–1.10) for the group living in the lowest median area income quartile Barwise et al (3) No significant difference for ICU readmission quartile 1 to quartiles 2–4 HR 1.35 (1.00–1.82)bHADS-A = Anxiety subscale of the Hospital Anxiety and Depression Scale, HADS-D = Depression subscale of the Hospital Anxiety and Depression Scale, HR = hazard ratio, IQR = interquartile range, LOS = length of stay, OR = odds ratio, RBANS = The Repeatable Battery for the Assessment of Neuropsychological Status, SES = socioeconomic status, SF-36 = 36-Item Short Form Survey.
aFurther data on magnitude of effect not presented.
bTransformed to maintain relationship of most deprived group to reference of least deprived group.
Individual studies have produced conflicting results on the impact of socioeconomic inequalities on mortality following admission to critical care. However, this meta-analysis demonstrated significantly higher short-term mortality following admission to critical care among the most deprived patients, compared with the least deprived.
Several mechanisms are plausible in the explanation of these inequalities. Reason for admission to critical care may differ by socioeconomic status. Three studies investigated the risk of sepsis, or septicemia, by socioeconomic status. One of which demonstrated increased odds of septicemia among patients resident in areas with high proportions below the federal poverty line (21), while two Scandinavian studies reported increased risk of admission with sepsis in patients with lower educational attainment and income (52,53). Other studies have shown that more deprived patients are more likely to be admitted with sepsis or trauma (7), acute exacerbations of chronic obstructive pulmonary disease (37), or substance misuse (3,30,50). The possibility that socioeconomic status may influence treatment delivery in critical care has been examined in several studies. Each found no difference in modalities of care (e.g., rate of mechanical ventilation, vasopressor use) or treatment withdrawal decisions (4,30,35,37,39). Another study found no association between socioeconomic status and frequency of family contact (35).
Socioeconomic differences in disease severity at the time of admission is another plausible mechanism for higher mortality in deprived groups. Three studies found that significant differences in unadjusted mortality between groups of varying socioeconomic status were mitigated when adjusted for initial disease severity (7,37,38). However, only one (37) of five studies (30,35,39,44) reporting an association between socioeconomic status and illness severity at admission found more severe illness in more deprived groups. Furthermore, other studies found a persistence of poorer mortality outcomes for socioeconomically deprived groups even after adjustment for initial disease severity (4,6,17,18,32,42,47). Future research should seek to define the causes of higher disease severity in the most socioeconomically deprived and how these may be mitigated.
The geographical availability of critical care may also be related to socioeconomic status. One study reported lower access to critical care in low-income communities in the United States, with only 51% of the lowest-income communities having ICU beds located within them, compared with 97% of the highest-income communities (54). Also, the risk of ICU admission has been shown to be higher in more deprived populations (47,50), and ICUs serving more socioeconomically deprived areas in Scotland experienced greater demand during the first wave of the COVID-19 pandemic (18).
While this review focused on the association between socioeconomic status and health outcomes following critical care, there is emerging research considering the effect of admission to critical care on subsequent socioeconomic outcomes. One study reported a negative impact on employment after discharge from critical care and a reduction in reported income (55).
Meta-regression demonstrated no significant difference in effect size estimate from pooling of studies that measured area-level socioeconomic status as opposed to individual-level markers. This contrasts with previous work in a noncritical care population, which reported only modest impact of area-level, compared with individual-level measures (56). It is plausible that our findings simply reflect a true similarity between area- and individual-level socioeconomic markers. Alternatively, area- and individual-level socioeconomic deprivation may each be independently associated with adverse outcomes through different mechanisms.
Relationship With Existing LiteratureThis work represents the first meta-analysis of the association between socioeconomic status and short-term outcomes following admission to critical care. It has explored the inconsistency of findings in the existing literature. An inclusive search strategy and recent publications allowed us to consider a greater number of sources than a previous systematic review (5).
Strengths and LimitationsThis review does have limitations. Significant heterogeneity was present in the literature with regard to differing measures of socioeconomic status and the relative positions on the spectrum of socioeconomic status of the compared groups.
Eligible studies reported a wide array of outcome measures, and there was a lack of standardization in the reporting of the same outcome; for example, in the follow-up period over which mortality was reported or the chosen measure of effect. The review did not include studies using only insurance status as a marker of socioeconomic status due to concern that this marker may not be generalizable across healthcare systems, however, this may have excluded potentially relevant studies.
Time-defined HRs and ORs were pooled without transformation. Although not ideal, this approach can be justified by the relatively rare event rate that therefore produced ratios close to 1. This approach was supported by meta-regression analysis between studies reporting HR and OR, which demonstrated that outcome measures accounted for none of the between-study heterogeneity (R2 = 0%). Additionally, effect measures with varying degrees of adjustment for confounders were pooled for meta-analysis. While this allowed the incorporation of the fullest breadth of existing literature, it has the potential to introduce bias. Post hoc meta-analysis of a subgroup reporting only those measures adjusted for confounders demonstrated a consistent effect to the original meta-analysis (Supplementary Fig. 2, https://links.lww.com/CCM/H267). Full analyses are reported in the Supplementary Appendix (https://links.lww.com/CCM/H267).
Most studies reporting length of stay associations did so for the full cohort (7,23,35,39,41,44,45). Therefore, paradoxically, an early death in ICU may represent a statistically favorable outcome, limiting the utility of these measures.
Moderate-to-substantial statistical heterogeneity was present in the studies included in meta-analysis of mortality outcomes, which may impair the interpretation of funnel plot asymmetry using Egger test; instead favoring visual interpretation, from which publication bias or small-study effects were suggested (57).
Our review benefits from robust methodology including standardized reporting using PRISMA guidelines, use of a random-effects model for pooled estimate, and a sensitivity analysis demonstrating consistent results after removing outlying studies.
CONCLUSIONSThis review and meta-analysis demonstrated that there are socioeconomic inequalities in health outcomes, even in the context of critical illness. While those working in critical care are limited in their ability to alter the socioeconomic status of their patients, a recognition of the higher risks of poor outcomes for people living with deprivation is crucial to ensure they receive optimum care during and after their admission (58).
On a system level, this review serves as further evidence that the inverse care law extends to critical care. Policymakers should ensure that the resourcing of critical care takes account of local socioeconomic patterns (59).
REFERENCES 1. Wilkinson RG, Marmot M: Social Determinants of Health: The Solid Facts. Denmark, World Health Organization, 2003 2. Marmot M, Friel S, Bell R, et al.; Commission on Social Determinants of Health: Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet. 2008; 372:1661–1669 3. Barwise A, Wi C-I, Frank R, et al.: An innovative individual-level socioeconomic measure predicts critical care outcomes in older adults: A population-based study. J Intensive Care Med. 2021; 36:828–837 4. Hutchings A, Raine R, Brady A, et al.: Socioeconomic status and outcome from intensive care in England and Wales. Med Care. 2004; 1:943–951 5. Jones JRA, Berney S, Connolly B, et al.: Socioeconomic position and health outcomes following critical illness: A systematic review. Crit Care Med. 2019; 47:e512–e521 6. Welch CA, Harrison DA, Hutchings A, et al.: The association between deprivation and hospital mortality for admissions to critical care units in England. J Crit Care. 2010; 25:382–390 7. Mullany DV, Pilcher DV, Dobson AJ: Associations between socioeconomic status, patient risk, and short-term intensive care outcomes. Crit Care Med. 2021; 49:e849–e859 8. Page MJ, McKenzie JE, Bossuyt PM, et al.: The PRISMA 2020
留言 (0)