
記住我










An initial bone mineral density (BMD) measurement is used to diagnose osteoporosis and decide whether patients need treatment, but the utility of repeating this test in those on treatment or on a drug holiday (ie, during a pause in bisphosphonate treatment) is controversial. Here, we present evidence for and against the use of BMD monitoring in patients receiving antiresorptive therapy or on a drug holiday, and give our recommendations, arguing against a one-size-fits-all approach.
KEY POINTSRecommendations for using BMD to make treatment decisions must be predicated on the availability of accurate, precise densitometry to minimize measurement error.
We recommend against measuring BMD again for patients already taking highly potent antiresorptive agents such as denosumab. However, we do suggest it for patients on less-potent antiresorptive agents. Changing to other, more-potent agents should be considered only if there is convincing bone loss, ie, if there is bone loss at more than 1 site or over more than 1 testing interval, or if there is bone loss and the patient’s levels of markers of bone turnover are not low (suppressed).
Further study is needed to assess the utility of repeating BMD measurement in those on treatment or on a drug holiday.
Dual-energy x-ray absorptiometry gives an estimate of bone mineral density (BMD) by measuring the differential attenuation of high-energy vs low-energy x-ray beams by mineralized bone matrix. Even though it does not tell us anything about thickness of the bone or its microarchitecture, and even though there is overlap in BMD between people who have fractures and those who do not,1 BMD is a strong predictor of fractures.2–4
A meta-analysis2 in 1996 indicated that a reduction in BMD of 1 standard deviation was associated with an increased risk of fracture, and the association was similar to the risk of stroke predicted by a 1-standard-deviation increase in blood pressure and better than the risk of cardiovascular disease predicted by a 1-standard-deviation increase in cholesterol levels. A more recent study3 suggested that each standard-deviation decrease in femoral neck BMD was associated with an approximately 3-fold increased risk of hip fracture in both men and women.
In view of these associations, BMD is used to diagnose osteoporosis,5 to monitor response to treatment,6–8 and to monitor for bone loss in patients not on treatment.9
However, while the utility of an initial BMD reading in assessing fracture risk is well established, the value of repeating it has been the subject of much debate. One reason proposed for measuring BMD again in patients on treatment is to verify whether the BMD is stable or increasing. For patients on a bisphosphonate drug holiday (ie, a pause in treatment after completing a course of the drug), the main reason proposed for measuring BMD again is to determine if it is time to resume treatment.
Guidelines from the Endocrine Society,10 the American Association of Clinical Endocrinologists,11 and the International Society of Clinical Densitometry12 recommend repeating BMD measurements during treatment and during the drug holiday, while guidelines from the American College of Physicians13 recommend not monitoring BMD after starting treatment. This dissonance of views has been confusing, highlighting the need for an objective measure for clinicians to use to follow patients during and after treatment.
Here, we present the evidence for and against monitoring BMD during treatment and during a drug holiday, we argue against using a one-size-fits-all approach, and we propose deciding on the basis of which drug the patient is receiving or has received and whether a stronger drug is available.
PATIENTS RECEIVING TREATMENT FOR OSTEOPOROSISFollowing up BMD measurements during treatment for osteoporosis makes sense only if the changes in BMD tell us whether the treatment is lowering the patient’s risk of fracture. If fracture risk were no different in those losing BMD compared with those gaining BMD on treatment for osteoporosis, it would make no sense to repeat the measurement.
While some early studies suggested that the increases in BMD during raloxifene treatment explained only a very small proportion of the reduction in fracture risk,14 most studies found that increases in BMD during treatment strongly predicted the reduction in fracture risk.15,16
Bouxsein et al17 performed a meta-regression analysis of 38 randomized controlled trials of 19 different treatments and concluded that increases in BMD during treatment strongly predicted lessening in fracture risk. The r2 values, or variance in fracture risk predicted by changes in BMD, were about 0.5, showing that about 50% of the improvement in fracture risk was accounted for by the change in BMD, and these associations were highly statistically significant.17
Therefore, despite the initial controversy, we consider this issue settled: improvement in BMD on treatment strongly predicts reduction in fracture risk on treatment.
Arguments against testingIf it is clear that improvements in BMD during treatment are meaningful, how then can one argue against monitoring BMD during treatment?
The main argument against it is that almost everyone receiving treatment has stable or improving BMD, and in the rest, most of the bone loss detected during treatment is actually due to measurement error, even when the bone loss reported exceeds the expected measurement error based on precision studies.18
Bell et al19 analyzed data from the Fracture Intervention Trial, which compared alendronate (specifically the name-brand Fosamax, which may be relevant—see “Arguments for testing,” below) vs placebo, and found that 97.5% of participants receiving active therapy gained BMD at the hip.
Cummings et al20 reanalyzed the same data and found that the group of patients who lost BMD while taking alendronate gained it back the next year, suggesting that they never truly lost BMD in the first place.
These 2 studies suggest that most people do not lose BMD while taking alendronate, and that when we find what looks like bone loss, it is usually measurement error that will regress to the mean and go back up the next year. So, while it is best to gain BMD on treatment, and it could be concerning to lose BMD on treatment, true bone loss on treatment is rare, and the bone loss that we do detect is usually not true bone loss.
Arguments for testingThis argument against monitoring BMD during treatment was rebutted in an editorial by Watts et al,21 who make several important points:
First, the data in the studies of Bell et al19 and Cummings et al20 were derived from a randomized controlled trial, from which patients were excluded if they had secondary risk factors for osteoporosis and in which the patients were highly adherent to taking their medications. This highly selected patient population is very different from that encountered in clinical practice, making generalization difficult. Dowd et al,22 for example, found that of 120 patients with osteoporosis seen in their clinic, only 3.3% to 20.8% would have qualified for inclusion in randomized controlled trials of anti-osteoporosis medications. The main reasons for exclusion were comorbidities, prior treatment for osteoporosis, and secondary osteoporosis.22
Furthermore, the analysis by Bell et al19 used data from the Fracture Intervention Trial, in which any participants losing significant BMD at the lumbar spine or total hip (> 8% over 1 year, > 10% over 2 years, and > 12% over 3 years) were excluded from the analysis, making it difficult to extrapolate these results to patients encountered in clinical practice.20,21
Moreover, the patients in the Fracture Intervention Trial received name-brand Fosamax. Generic formulations may not be as effective: 40% to 50% lesser gains in BMD were seen when generic formulations of alendronate were used compared with the brand-name preparation.23 In vitro studies found that different generic preparations differed in how fast they disintegrate, which may at least partially explain these findings.24,25
Furthermore, not all anti-osteoporosis drugs are equivalent. Alendronate preserved BMD more effectively than ibandronate,26 risedronate,27 and raloxifene28 in head-to-head trials, so even if most patients taking alendronate do not lose BMD, the same cannot be said for less-potent drugs.
How much observed bone loss is real?The questions then remain, how often do patients lose bone during treatment for osteoporosis and, of the observed bone loss, how much is real and how much is measurement error? Given the limitations in directly extrapolating from randomized controlled trials, let us examine real-world data regarding the utility of repeating BMD measurements in those taking anti-osteoporosis medications.
Kline et al29 retrospectively analyzed data from 1,369 women in Manitoba, Canada, who had at least 3 serial BMD measurements. Most (79.7%) of these women were taking bisphosphonates, and they had undergone repeat BMD testing at approximately 3-year intervals from baseline. Only 1.4% showed BMD losses at both treatment intervals.29
The large sample size, exclusion of those switching therapies, use of a province-wide centralized BMD program, and the high medication adherence rate (> 85%) were notable strengths of the study. Given that only 1.4% of participants lost BMD at both intervals, the study authors questioned the utility of repeating BMD measurement for postmenopausal women who were highly adherent to antiresorptive therapies.29
However, another way of looking at these data is that while only 1.4% of participants lost BMD at both intervals, among the 6.5% of participants who lost BMD at the lumbar spine in the first interval, 62.5% were determined to have loss of BMD at that site on long-term follow-up, while among the 13.4% of women who lost BMD in the first interval at the total hip region, 72.4% were determined to have loss of BMD on long-term follow-up.29
Our recommendationsWe estimate that two-thirds to three-quarters of the bone loss seen in patients receiving antiresorptives is real, while the remainder perhaps is “noise.” The likelihood of experiencing real bone loss is likely higher in those taking less-potent antiresorptives and in those not adherent to therapy. If one accepts the premise that bone loss on treatment is concerning and not uncommon, and if more-potent antiresorptives such as denosumab are available,30 following BMD on treatment seems a reasonable and defensible strategy.
The following are our recommendations:
Densitometry must be of high quality to be worthwhile.18 If the densitometry that is available is not of high quality, most of the bone loss that is discovered will be measurement error, and follow-up BMD measurements during treatment cannot be recommended. Best practices for bone densitometry have been published by the International Society for Clinical Densitometry Guidance.18
Few patients lose BMD while taking highly potent agents. In a number of studies,26–31 a substantial minority of patients lost BMD during treatment, but the more potent the antiresorptive, the less likely that patients will lose BMD.
Denosumab is more potent than alendronate in its effects on BMD and bone turnover,30 and few patients being treated with denosumab had significant bone loss in the Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) study (Figure 1).31 For this reason, we are inclined to accept the logic that argues against serial densitometry in patients receiving denosumab.19 Bone loss is unlikely with this drug, and even if we did find bone loss in patients on denosumab, what alternative do we have that is more effective? In this case, the patient is already receiving the most potent antiresorptive. If we found bone loss in a patient taking a less potent drug, we could switch to a more potent drug, but if we find bone loss in a patient taking a more potent drug, where do we go from there?
 Figure 1
Figure 1 Waterfall plots demonstrating the percent changes in bone mineral density on treatment with denosumab vs placebo at the lumbar spine (A) and total hip (B) over 36 months in the Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months study. While many patients in the placebo group lost bone mineral density, few in the denosumab group did. Almost none of the participants on denosumab lost a significant amount of bone mineral density (> 5%) over 36 months.
Reprinted from Bolognese MA, Teglbjærg CS, Zanchetta JR, et al. Denosumab significantly increases DXA BMD at both trabecular and cortical sites: results from the FREEDOM study. J Clin Densitom 2013; 16(2):147–153. doi:10.1016/j.jocd.2012.02.006 with permission from Elsevier.
True bone loss must be distinguished from measurement error. Although some bone loss during treatment is real, some is clearly due to measurement error.20,29 If we do perform serial densitometry on treatment, how is the clinician to know if the observed bone loss on treatment is real or due to measurement error? Switching all patients losing BMD on alendronate to denosumab when only a fraction of them are really losing BMD is not recommended. Switching treatments is recommended only if the observed bone loss is convincing.
Convincing bone loss would be bone loss at more than 1 site or over more than 1 interval, or bone loss associated with elevated markers of bone turnover such as cross-linked C-telopeptide of type-1 collagen (CTx) greater than 300 pg/mL.32 If a patient on treatment loses BMD at 1 site over 1 interval with a low CTx, we would presume that the bone loss might be due to measurement error, and we would continue the current treatment and continue to monitor. This recommendation is similar to that made by the International Osteoporosis Foundation on inadequate response to osteoporosis treatment.33
PATIENTS ON A DRUG HOLIDAYA drug holiday is appropriate only for patients who have completed a course of bisphosphonate treatment, since bisphosphonates such as alendronate and zoledronate are known to continue to protect for years after a course is completed. A holiday is not suggested after a course of estrogen, raloxifene, denosumab, or anabolic treatments, since patients will lose BMD after stopping these agents.
The concept of a drug holiday after bisphosphonate treatment is based on the idea that after a course of bisphosphonates, BMD remains fairly stable and bone turnover is substantially depressed for years, though the duration of stability varies based on the half-life and potency of the bisphosphonate used.
Bone et al34 found that in patients who had completed 5 years of alendronate treatment, spine BMD remained stable and mean hip BMD decreased by 1.8% over the subsequent 5 years. While mean urine cross-linked N-telopeptide of type 1 collagen had been suppressed to 70% below baseline on treatment and rose during the drug holiday, it remained suppressed to about 50% below baseline. Turnover was more suppressed without any hip BMD loss in those who continued alendronate out to 10 years.34
A larger study of 5 vs 10 years of treatment with alendronate35 and a study of 3 vs 6 years of zoledronate36 yielded similar findings. These 2 studies also demonstrated a lower risk of fractures with the longer course of bisphosphonates, which came at the cost of the risk of overtreatment syndromes such as atypical femoral fractures, which start to rise in incidence to about 1 in 1,000 per year with longer duration of therapy.37,38
These studies provide the evidence for letting patients with osteoporosis suspend bisphosphonate treatment after completing a course of treatment, after which they can continue to enjoy some protection for some time. Of note, there are no data that patients can enjoy protection after stopping a course of ibandronate or risedronate, though it is common practice to give them a drug holiday as well to avoid the potential for overtreatment syndromes such as osteonecrosis of the jaw or atypical femoral fractures.11
How should patients be followed during the drug holiday?Since improvement in BMD during treatment correlates with a reduction in fracture risk, it seems likely that loss of BMD during the drug holiday would correlate with an increase in fracture risk. But how often do we see significant bone loss during the drug holiday?
McNabb et al39 reported that of 406 patients who took alendronate for 5 years and then had 5 years of follow-up off alendronate in the long-term extension of the Fracture Intervention Trial, 29% had more than a 5% reduction in mean hip BMD, and some had a reduction of more than 10% (Figure 2).39 Based on this analysis, if we are concerned about bone loss during a drug holiday, there is a substantial minority of patients losing BMD during the drug holiday who could be identified with serial densitometry and then undergo another course of treatment.
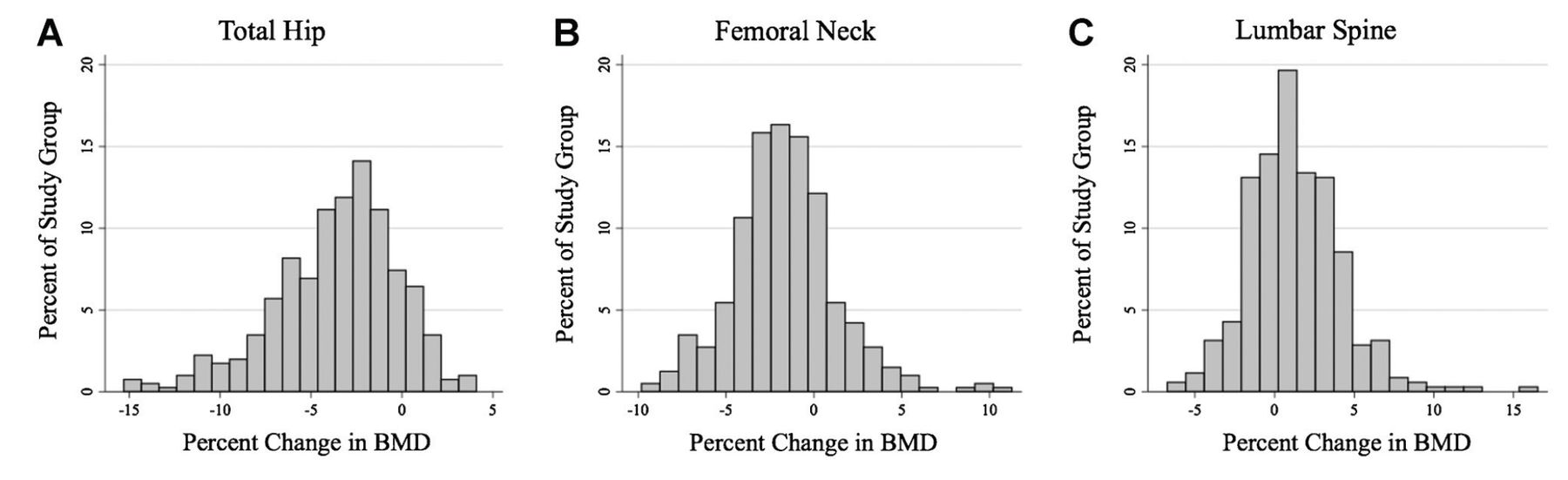 Figure 2
Figure 2 Changes in total hip bone mineral density (BMD) 5 years after completing a 5-year course of treatment with alendronate in the long-term extension of the Fracture Intervention Trial. Many patients had no significant hip bone loss, but a substantial minority had more than 5% bone loss, and an even smaller minority had more than 10% bone loss.
Reprinted from McNabb BL, Vittinghoff E, Schwartz AV, et al. BMD changes and predictors of increased bone loss in postmenopausal women after a 5-year course of alendronate. J Bone Miner Res 2013; 28(6):1319–1327. doi:10.1002/jbmr.1864 with permission from John Wiley and Sons.
Arguments for and against testingThe main argument against serial densitometry during the drug holiday was made by Bauer et al.40 Analyzing the same cohort of participants followed off alendronate for 5 years, they reported that the tertile of hip BMD loss at 1 year did not predict the risk of fracture during the drug holiday, but age and T-score at the time of discontinuation of alendronate did. They concluded that changes in BMD off treatment with alendronate are not predictive of fracture risk, and monitoring BMD during the drug holiday is not warranted.40
While Bauer et al make a cogent point, they reported that while 1-year changes in hip BMD did not predict fracture risk during the drug holiday, 2-year changes did.40 We must consider as well that there is always some measurement error around each measurement of BMD, so that the annual bone loss determined at a 1-year interval may have more noise than annual bone loss determined at a 2- or 3-year interval. This point harkens back to the discussion above about “convincing” bone loss: it is very likely that bone loss at 2 sites, or bone loss at 1 site over multiple measurements, or bone loss at 1 site with clearly increasing CTx predicts fracture more than does isolated bone loss at 1 site.
In addition, fracture risk is largely determined by the T-score at the time one enters a drug holiday. But if a patient is on a drug holiday, a determination has already been made based on fracture risk and duration of treatment that it was time to start the drug holiday. The real question we are confronted with when a patient is on a drug holiday is whether the protection from the prior course is wearing off. If the protection is wearing off, then it is necessary to give more treatment to prevent further bone loss, and it should be safe from the perspective of overtreatment syndromes such as osteonecrosis of the jaw to resume treatment. So the challenge is not how best to predict fractures during the drug holiday, but rather to determine when there is evidence for dissipation of protection based on serial measurements of BMD and measurements of turnover.
In practice, do patients do better with all this monitoring during the drug holiday, or would they do just as well if we pick a fixed duration of drug holiday (3 or 5 years), after which they would resume treatment? This question has unfortunately never been directly studied. The closest information we have available is through follow-up of patients starting a drug holiday, suggesting that bone loss is common on a drug holiday following treatment with risedronate and less common but not rare following alendronate or zoledronate treatment.39,41 Therefore, BMD may be monitored at a shorter time interval during a drug holiday after taking risedronate compared with that for alendronate or zoledronate.
Until a dedicated randomized study is done to inform the utility of monitoring, the clinician needs to choose an approach that makes sense. If the clinician would like to make this decision based on the imperfect monitoring tools we have, that is reasonable. If the clinician is unconvinced that we can get clear and meaningful guidance from monitoring, at the beginning of the drug holiday the clinician should choose how long the holiday should be, after which treatment should be resumed. Our opinion, and that of many osteoporosis organizations11,12,18 is that we can get meaningful information from monitoring, but only if we have high-quality bone densitometry available.
Our recommendationsWe believe that the duration of the drug holiday should depend on how likely it is that the patient is losing BMD. Again, we argue against a one-size-fits-all approach and make the following recommendations regarding repeating BMD while on a drug holiday:
Rationale for repeating BMD: Does the patient need to resume treatment? The rationale for repeating BMD on a drug holiday should be to determine when the effect of bisphosphonate treatment is dissipating and the patient is a candidate for more treatment. Availability of high-quality bone densitometry is a precondition to repeating BMD.
Testing interval depends on the agent used. Given the data regarding loss of BMD while on drug holiday, and taking into account the relative duration of effect of individual agents, we believe that BMD should be repeated in 1 year after pausing risedronate, and 2 to 3 years after pausing alendronate or zoledronate. This recommendation is similar to that by the task force by the American Society for Bone and Mineral Research on managing osteoporosis for those on drug holidays.42
Resume treatment if necessary. We recommend resuming treatment if there is convincing evidence for dissipation of the effect of treatment, as demonstrated by convincing bone loss at more than 1 site, or over more than 1 interval, or that associated with nonsuppressed markers of bone turnover such as CTx.
Some patients can resume without testing. Patients who have already had a long drug holiday and patients whose drug holiday began after a course of risedronate might be candidates for restarting treatment with any sign of bone loss, while patients who had been on alendronate or zoledronate and have had a less than 5-year drug holiday might not be candidates for restarting until we see more convincing bone loss.
NO CLEAR ANSWERThere is no clear answer to the question of how patients with osteoporosis should be followed while on treatment and during a drug holiday. Changes in BMD during these periods are likely meaningful but are confounded by measurement error. For this reason, some clinicians will choose to treat with an agent for a specified duration, and then stop treatment for a drug holiday for a period of time. A perfectly reasonable alternative that we and many specialty societies recommend is to follow patients while on treatment to assure stability of BMD, and during the drug holiday to determine when to resume treatment.11,12
Again, monitoring BMD is reasonable only if high-quality densitometry is available.
Furthermore, monitoring BMD on treatment makes sense if more-potent treatments are available, and makes less sense if the patient is already taking a highly potent treatment and deterioration of BMD is not likely to change treatment. Further study is needed to assess the utility of repeating densitometry as a measure of treatment adequacy in patients on treatment and drug holiday on specific antiresorptive agents.
DISCLOSURESDr. Khan has disclosed teaching and speaking for Amgen, Boehringer Ingelheim, Eli Lily Canada, IPSEN, Janssen, and NovoNordisk Canada, and working as advisor or review panel participant for Eli Lily Canada. The other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
留言 (0)