
記住我

Twenty-seven patients (20 medulloblastoma, 7 ependymoma) enrolled on the protocol who underwent imaging response assessment were included with a median follow-up of 3.0 years (95% confidence interval [CI], 1.8–7.4; Supplemental Fig. 1). Of the 13 medulloblastoma patients with molecular subtyping, most (9, 45%) were non-WNT/non-SHH. One patient with medulloblastoma had underlying Li-Fraumeni Syndrome with a pathogenic germline p53 mutation (Table 1). Median age at cRIT initiation was 12 years (range, 3–40).
Table 1 Baseline patient and disease characteristicsAt cRIT initiation, 9 (45%) medulloblastoma and 4 (57%) ependymoma patients had radiologically MD (Table 2). One patient with medulloblastoma was radiologically NED but had malignant cells in the CSF and therefore was categorized as having MD. Median number of cRIT injections was 3 (range, 1–4) with median total dose of 72 mCi (range, 2–192). Two patients (both with medulloblastoma) only received a single test dose (2 mCi). Eight patients (30%) had previously received cRIT with 131-I-3F8 before receiving cRIT with 131-I-omburtamab.
Table 2 Disease Status at I-131-Omburtamab cRIT InitiationExternal beam radiotherapy prior to 131-I-omburtamabAll patients had EBRT at a median time of 0.9 years (range 0.1–5.2) preceding cRIT (Supplemental Table 1). Most patients received CSI (22, 81%), with a median dose of 2340 cGy (range 2300–3960 cGy) with a boost to 5400 cGy (range 5040–6000 cGy). Ten (37%) CSI treatments were delivered with protons, all for patients with medulloblastoma. Most patients (20, 74%) received a focal course of EBRT, five of which were delivered with protons. Among patients with medulloblastoma, the maximum dose of EBRT pre-cRIT ranged from 1800 to 5000 cGy (median 3000 cGy). For ependymoma, the maximum dose of EBRT pre-cRIT ranged from 4720 to 5940 cGy (median 5700 cGy). Prior to cRIT, 15 (56%) medulloblastoma and 6 ependymoma (86%) patients received more than one course of EBRT. None of the patients received multiple courses of CSI pre-cRIT.
Disease responseMedulloblastomaAll 20 patients received EBRT prior to cRIT at a median time of 0.6 years (range, 0.1–4.9). Most patients (12, 60%) received EBRT as part of bridging therapy, nearly all (11, 92%) of which were re-irradiation and three were with protons (2 CSI, 1 focal; Table 2). Surgical resection was commonly (12, 60%) used as part of bridging to cRIT. One patient received 131-I-3F8 as part of the bridging regimen to 131-I-omburtamab. Only three patients received additional systemic therapy after cRIT initiation. Nine patients had MD at cRIT initiation: multifocal radiologic disease in eight and isolated cytologic disease in one. Of the patients with baseline MD, five progressed on initial assessment, two had stable MD, and two achieved CR to cRIT. Of the two complete responders, one recurred 4 months after cRIT but is still alive and the other remained in remission 1.5 years after cRIT (Fig. 1).
Fig. 1
Swimmer’s plot demonstrating timing of treatments received and progression events. An arrowhead indicates that the patient was alive at the time of last follow-up. Those without an arrowhead indicate that the patient died at that time. *One patient was lost to follow-up and died of unknown causes. MB medulloblastoma; EP ependymoma; MD measurable disease; CSF cerebrospinal fluid; 8H9, I-131-omburtamab; cRIT compartmental radioimmunotherapy. TTwo patients (both with medulloblastoma) only received a single test dose (2 mCi)
Four patients remain in remission: at cRIT initiation, three had NED and one had multifocal leptomeningeal disease in the spine. Sixteen patients ultimately had disease progression at a median time of 0.8 years (range, 0.2–4.0) after most recent relapse and 0.2 years (range, 0.1–3.4) after cRIT initiation. Half of those who progressed had NED at cRIT initiation: four progressed focally intracranially, two progressed multifocally intracranially, and one had LMD in the spine per outside report (Supplemental Fig. 2). The other half who progressed had MD at cRIT initiation, and these progression patterns were nearly all multifocal and/or diffuse with LMD, with the exception of one patient with isolated cytologic disease at baseline who ultimately developed focal intracranial LMD.
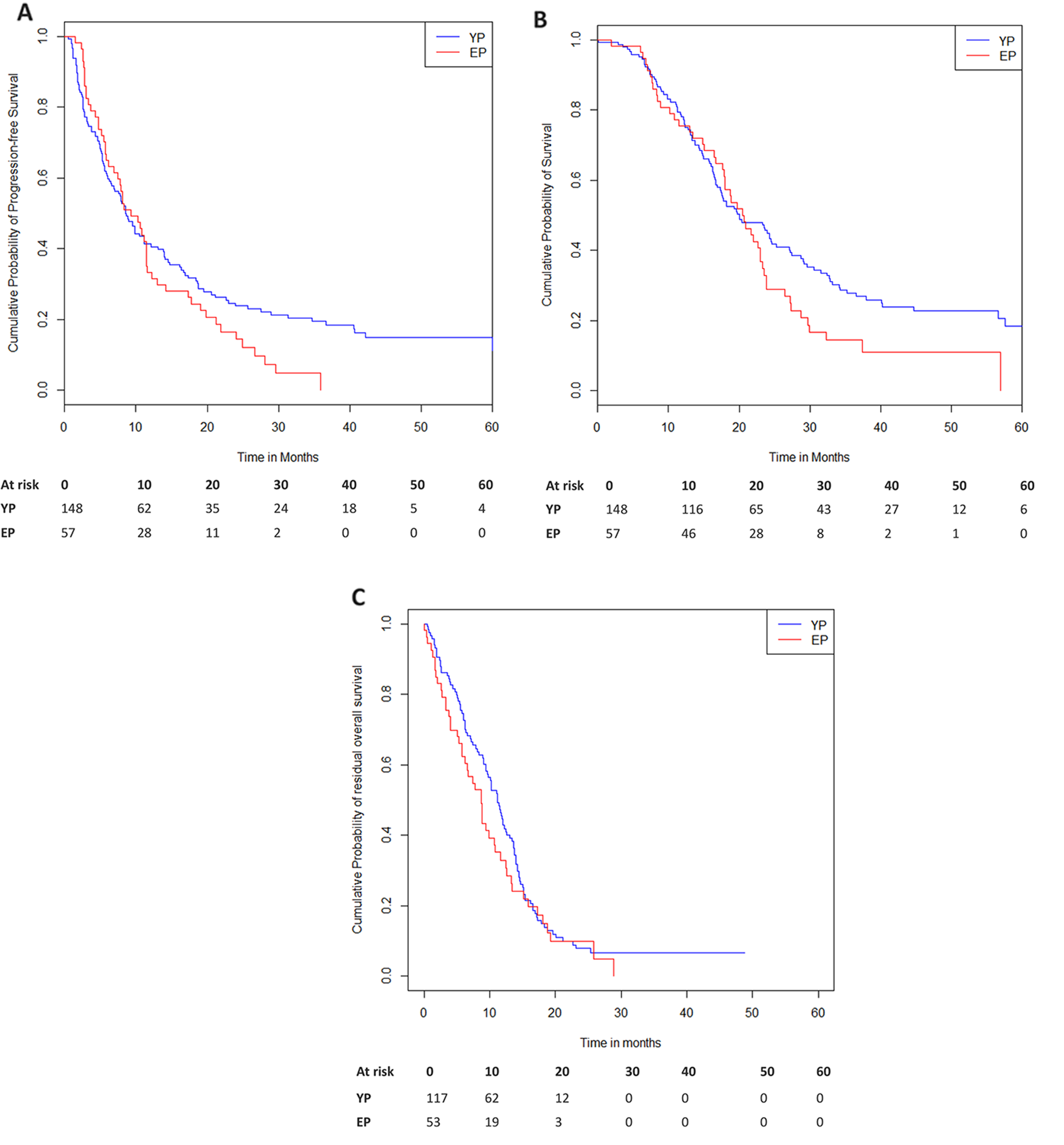
Median PFS following cRIT for the medulloblastoma cohort was 0.4 years from cRIT initiation (95% CI 0.1–1.7; Fig. 2A) and 1.2 years from the most recent relapse preceding cRIT (95% CI 0.4–2.6). Patients who were NED at cRIT initiation had significantly improved PFS compared to those with MD (1.7 vs 0.1 years, p = 0.002; Fig. 3A). Median OS was 1.9 years after cRIT initiation (95% CI 0.9–10.9; Fig. 2B) and 2.3 years from most recent relapse pre-cRIT (95% CI 1.2–11.1). OS was improved among patients who were NED vs those who had MD at cRIT initiation (p = 0.048, Fig. 3B). The median PFS was numerically lower among non-SHH/WNT patients than SHH-activated patients (0.21 years [95% CI 0.07–3.24] vs 1.74 years [95%CI 1.73–1.92]; log-rank p = 0.23; Supplemental Fig. 3A). Similarly, the OS was also numerically lower among the non-SHH/WNT patients (0.44 years [95%CI 0.07-NR] vs 1.91 years [95%CI NR-NR]; log-rank p = 0.020; Supplemental Fig. 3B).
Fig. 2
Survival outcomes among patients with medulloblastoma (top) and ependymoma (bottom) calculated from the time of pre-cRIT relapse. A Progression-free and B overall survival among patients with medulloblastoma. C Progression-free and D overall survival among patients with ependymoma. Note: one patient with ependymoma was lost to follow-up and was therefore not included in the progression free survival calculation
Fig. 3
Survival outcomes among patients with medulloblastoma based on disease status at cRIT initiation. A Progression free and B overall survival from cRIT administration among patients with medulloblastoma. cRIT, compartmental radioimmunotherapy
Among medulloblastoma patients, three underwent additional focal EBRT following cRIT for future recurrences. One patient received partial brain EBRT (2000 cGy), one patient received focal EBRT to the spine (2000 cGy), and one patient received three additional focal EBRT courses to the brain (maximum dose 3000 cGy). No patients received CSI post-cRIT.
EpendymomaWhile all the patients with ependymoma had received EBRT at a median time of 1.2 years (range, 0.2–5.2) preceding cRIT, none had received EBRT as a bridge to cRIT after the most recent relapse (Table 2). All patients underwent surgical resection as a bridge to cRIT. Four patients had MD at cRIT initiation: two had LMD (one spinal alone, one both intracranial and spinal) and one with parenchymal disease. None had evidence of CSF involvement at cRIT initiation. No patients received additional systemic therapy after cRIT initiation.
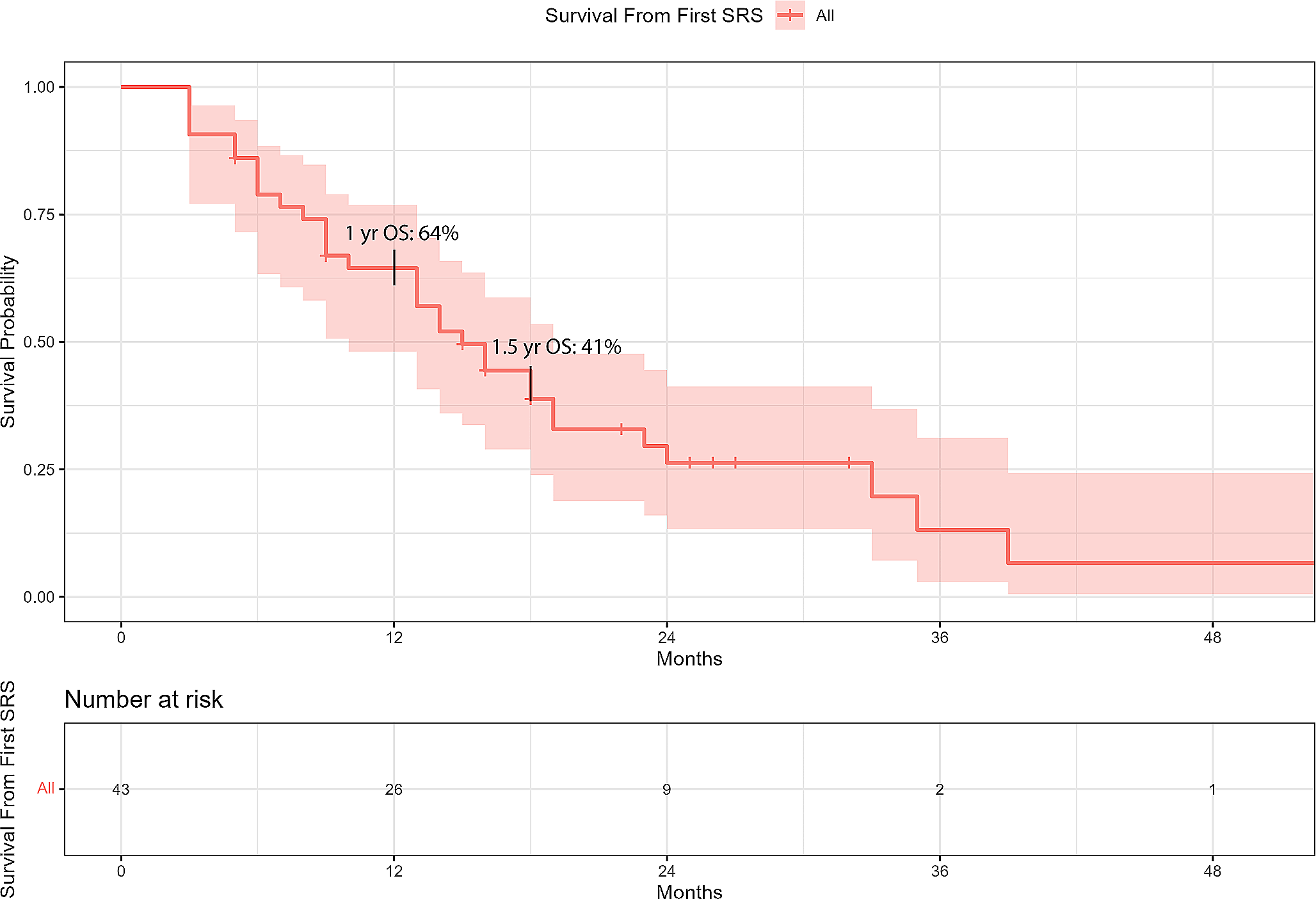
Five patients ultimately had progression at a median time of 0.4 years (range, 0.2–1.9) after most recent relapse and 0.2 years (range, 0.1–1.4) after cRIT initiation: two who were NED at cRIT initiation ultimately relapsed at or adjacent to the site of initial intraparenchymal disease, one had progression of the pre-cRIT measurable LMD disease in the spine but had PR in the intracranial LMD, one failed both at the measurable pre-cRIT site in the brain as well as developed new LMD in the spine, and one failed in both the brain parenchymal and had LMD in the spine (Supplemental Fig. 1). One patient who had measurable spine LMD at cRIT initiation was lost to follow up after initial post-cRIT MRI showed stable disease and he ultimately died 12.8 years after cRIT initiation (Fig. 1). Median PFS (excluding the patient lost to follow-up who died of unknown causes) was 1.2 years from relapse (95% CI 0.2-NR) and 0.8 years from cRIT initiation (95% CI 0.1-NR; Fig. 2C).
Three patients underwent additional focal EBRT to the brain following cRIT for progression (one patient received 5940 cGy) or recurrence (one patient received 4 additional courses to multiple sites in the brain with a maximum dose of 5400 cGy, another patient underwent stereotactic radiosurgery of unknown total dose). No patients received CSI post-cRIT. The one patient who is alive at last follow-up without evidence of disease was originally NED at cRIT initiation. Median OS was 7.1 years from pre-cRIT relapse (95% CI 0.5–12.9) and 6.7 years from cRIT initiation (95% CI 0.4–12.9; Fig. 2D).
Radiologic eventsOf the 13 patients who had radiologic findings following cRIT, there were no cases of radionecrosis (Supplemental Table 2). The most common event identified was cavernoma (6, 46%), although all were asymptomatic and none required intervention. Three patients (23%) had hydrocephalus, one of whom was symptomatic secondary to acute cerebral aqueduct stenosis requiring shunt placement. One patient did ultimately develop posterior reversible encephalopathy syndrome (PRES) in the setting of pre-existing infarcts. However, this clinic-radiographic syndrome was diagnosed after the developing acute myeloid leukemia (AML). One patient had had ventricular prominence, one had subdural effusions, and one had intramedullary hemorrhage.
留言 (0)