
記住我

Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver worldwide, with approximately 782 000 deaths due to HCC each year, placing it in the top four causes of cancer death worldwide [1]. Treatment options for HCC include surgical resection, radiofrequency ablation, transcatheter arterial chemoembolization (TACE) and liver transplantation, but radical resection remains the mainstay of HCC treatment today. However, high rates of recurrence and metastasis significantly reduce the overall survival (OS) of HCC patients [2–4]. The 5-year recurrence rate after radical surgery for HCC is as high as 70%, and the mortality rate is as high as 50% [5]. Postoperative recurrence of HCC is divided into early recurrence and late recurrence. Patients with early recurrence have poor and aggressive tumor biology and a worse prognosis than patients with late recurrence [6].
The histopathological pattern of HCC is divided into the steatohepatitic, clear cell, macrotrabecular-massive (MTM), scirrhous, chromophobe, fibrolamellar, neutrophil-rich and lymphocyte-rich HCC according to the ‘WHO Classification of Digestive System Tumours 5th edition’ [7]. A new histological subtype, the MTM subtype, proposed by the French pathologist Calderaro, was also included in the ‘WHO Classification of Tumours of the Digestive System 5th edition’. MTM-HCC refers to HCC characterized by macrotrabecular structures accounting for more than 50% of trabeculae (trabeculae >6 cells thick), and it accounts for approximately 10–20% of all HCC. This type of HCC is more aggressive than other types and is an independent risk factor for early postoperative recurrence [8,9].
At present, many scoring systems and prediction models are available to predict the early recurrence of HCC, for example, the American Joint Committee on Cancer 8th edition (AJCC 8th) and Barcelona Clinic Liver Cancer (BCLC) staging systems [10]. However, these traditional scoring criteria are only used to assess the prognosis of different subgroups of patients and cannot predict the probability of recurrence in specific individuals. Nomograms, prediction charts based on multiple independent risk factors, have been used to predict the postoperative recurrence of HCC, and their predictive performance is better than that of traditional HCC staging [11–13]. Currently, most of the nomograms for predicting postoperative early recurrence are based on clinical data such as alpha-fetoprotein (AFP) level, tumor size and microvascular invasion (MVI) in patients [12,13], and few studies have analyzed the predictive value of HCC pathology, such as MTM-HCC, for early recurrence [8,9,14,15].
Therefore, by analyzing the clinical and pathological data of postoperative HCC patients, our study aimed to analyze the predictive factors on early postoperative recurrence of HCC and establish a new nomogram that incorporated MTM-HCC to more effectively predict early postoperative recurrence of HCC.
Patients and methods PatientsFrom January 2015 to September 2020, a total of 507 patients underwent surgery in the Department of Hepatobiliary and Pancreatic Surgery, Li Huili Hospital of Ningbo Medical Center, China. Clinical and pathological and postoperative follow-up data, including patient sex, age, AFP concentration, surgical condition and tumor pathological features, were collected. HCC histopathological patterns were classified into the microtrabecular subtype, pseudoglandular subtype macrotrabecular subtype, solid subtype and MTM according to the ‘WHO Classification of Tumours of the Digestive System 5th edition’. There was no significant difference in prognosis among the first several types in the preliminary analysis, and they were combined into a non-MTM-HCC group for comparison with the MTM-HCC group. This study protocol complied with the ethical standards established by the Declaration of Helsinki in terms of patient data confidentiality. And this study was approved by the Ethics Committee of Ningbo Medical Centre Lihuili Hospital (KY2020PJ200). all patients or their families signed informed consent before the surgery.
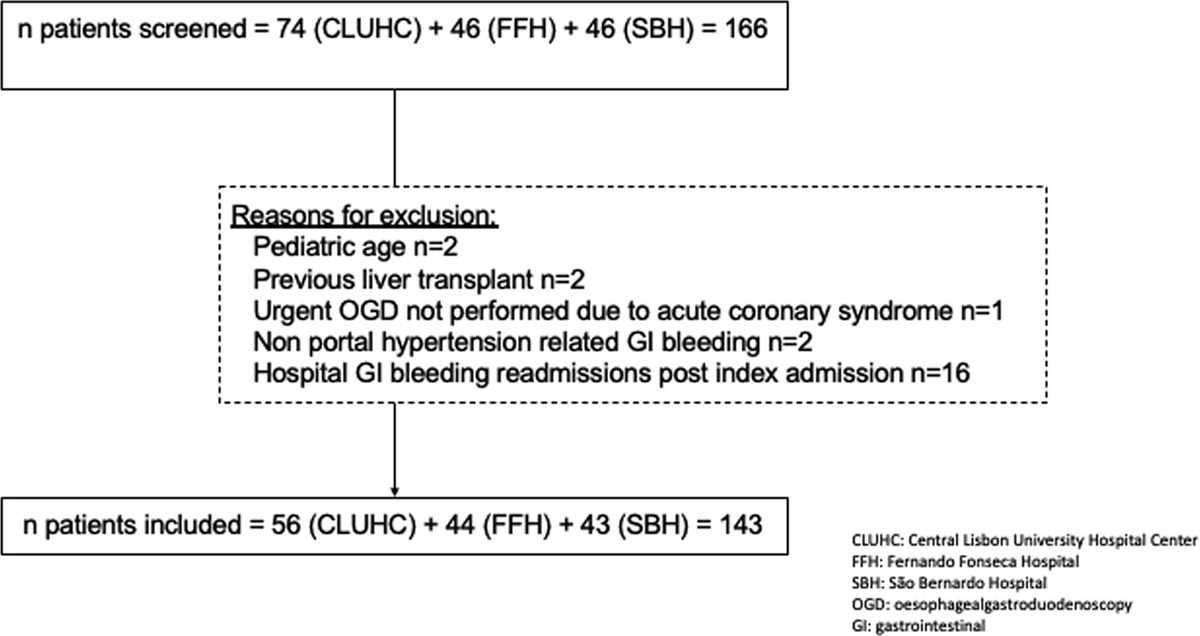
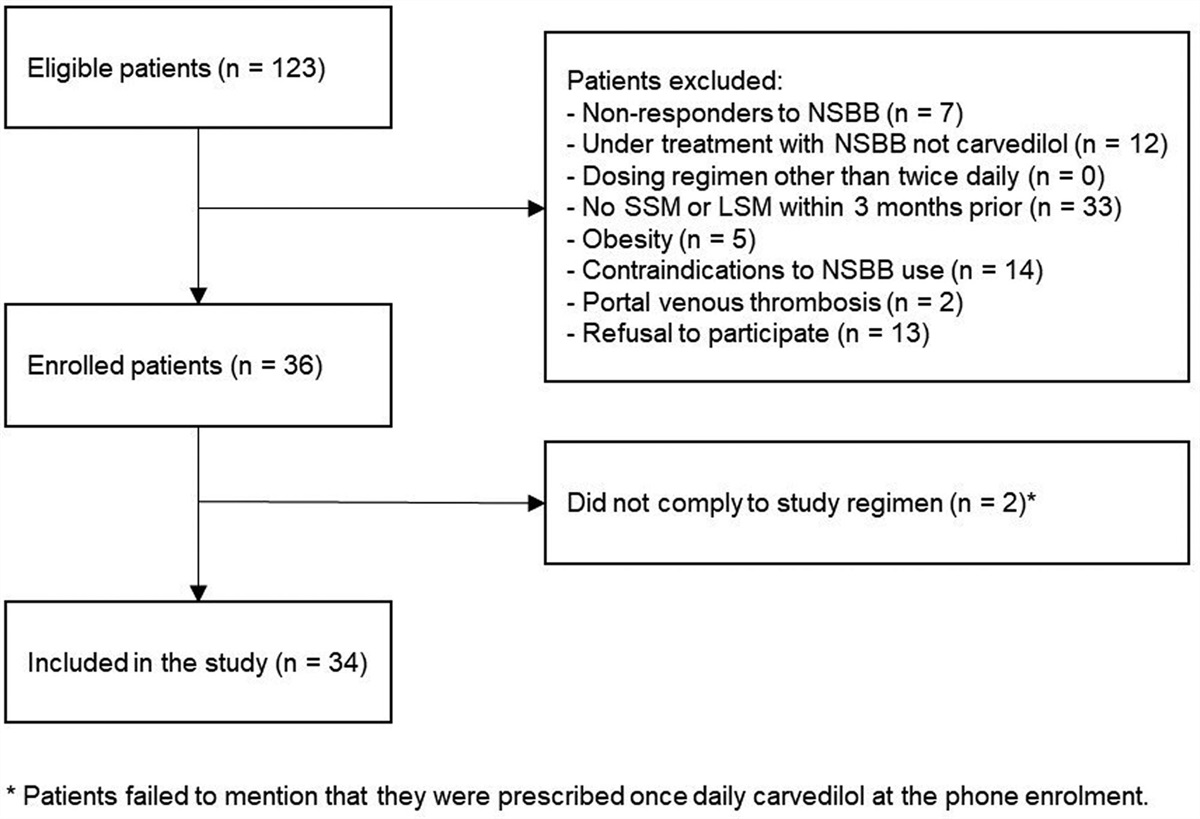
The inclusion criteria were as follows: (1) radical resection; (2) postoperative pathologically diagnosed HCC and (3) no other malignant diseases. The exclusion criteria were as follows: (1) perioperative death; (2) incomplete clinical and pathological data or follow-up information; (3) the follow-up time was less than 1 year; (4) postoperative use of tyrosine kinase receptor inhibitor and (5) surgical resection for recurrent HCC. A total of 314 patients were screened according to the inclusion and exclusion criteria (Fig. 1). These predictive factors on early postoperative recurrence were analyzed and compared between the early recurrence group and the nonrecurrence group.
 Fig. 1.:
Fig. 1.: Flow chart of the study population.
Postoperative follow-upThe postoperative follow-up protocol for patients was as follows: review at the first month after discharge, every 3 months for 2 years and every 6 months after 2 years. The follow-up included liver function, AFP concentration and liver ultrasound. Enhanced computed tomography (CT) or enhanced MRI of the abdomen was performed every half year.
Survival times were calculated as follows: disease-free survival (DFS): time of HCC resection until the detection of tumor recurrence; OS: time of HCC resection to the date of the patient’s death or the date of last follow-up visit. The cutoff follow-up date for this study was September 2021. All tumor recurrences were diagnosed via CT or MRI images. Early recurrence was defined as recurrence within 1 year after surgery.
Statistical analysisThe Kaplan–Meier method was used to analyze the survival curve, and the log-rank test was used to compare DFS and OS between the two groups. Univariate and multivariate Cox regression analyses were used to compare the cumulative risks of HCC recurrence. Then, a nomogram was formulated to predict early postoperative recurrence of HCC based on the results of the multivariate Cox regression analysis. Nomogram performance was assessed via internal validation and calibration curve statistics (the concordance index was calculated to measure discrimination with 1000 bootstrap samples). Decision curve analysis (DCA) was conducted to determine the clinical usefulness of the nomogram by quantifying the net benefits along with the increase of threshold probabilities. The predictive ability of the model, AJCC and BCLC for tumor recurrence was compared by receiver operating characteristic (ROC) curve analysis.
Statistical Product and Service Solutions (SPSS) 25.0 (IBM Corporation, 2020, USA) was used for the survival analysis, Cox regression analysis and ROC analysis. Using R version 3.6.2, the nomogram was constructed, and the survival figures were plotted. P values are derived from two-tailed tests. P < 0.05 was considered statistically significant.
Results Patient characteristicsA total of 383 patients were included in this study with a median follow-up time of 34.0 months (12–83 months). Among them, 317 (82.8%) were male, and 66 (17.2%) were female, with a mean age of 59.6 ± 10.8 years. A total of 286 (74.7%) patients had a history of hepatitis B, and 149 (38.9%) had received standardized antiviral therapy. The preoperative AFP level of patients was 28.7 (5.0, 505.3) (ng/ml); 10 (2.6%) patients had Child-Pugh scores of grade B and the rest had Child-Pugh scores of grade A. Thirty-four (8.9%) patients had preoperative TACE, and 67 (17.5%) patients had received an intraoperative blood transfusion. In terms of tumors, most patients had one tumor; only 69 (18.0%) patients had multiple tumors. The tumor size was 4.9 ± 3.1 cm. A total of 210 (54.8%) patients had no MVI; 173 (45.2%) patients had MVI; 238 (62.1%) patients had tumors of well differentiation; 145 (37.9%) patients had tumors of poorly differentiation and 88 (23.0%) patients had MTM-HCC.
A total of 152 patients developed recurrence after surgery, of which 83 (54.6%) had recurrence within 1 year. Of 152 patients, there were 131 patients developed intrahepatic recurrence, 7 patients with extrahepatic metastasis and 14 patients with multiple metastases. The median recurrence time was 10 months.
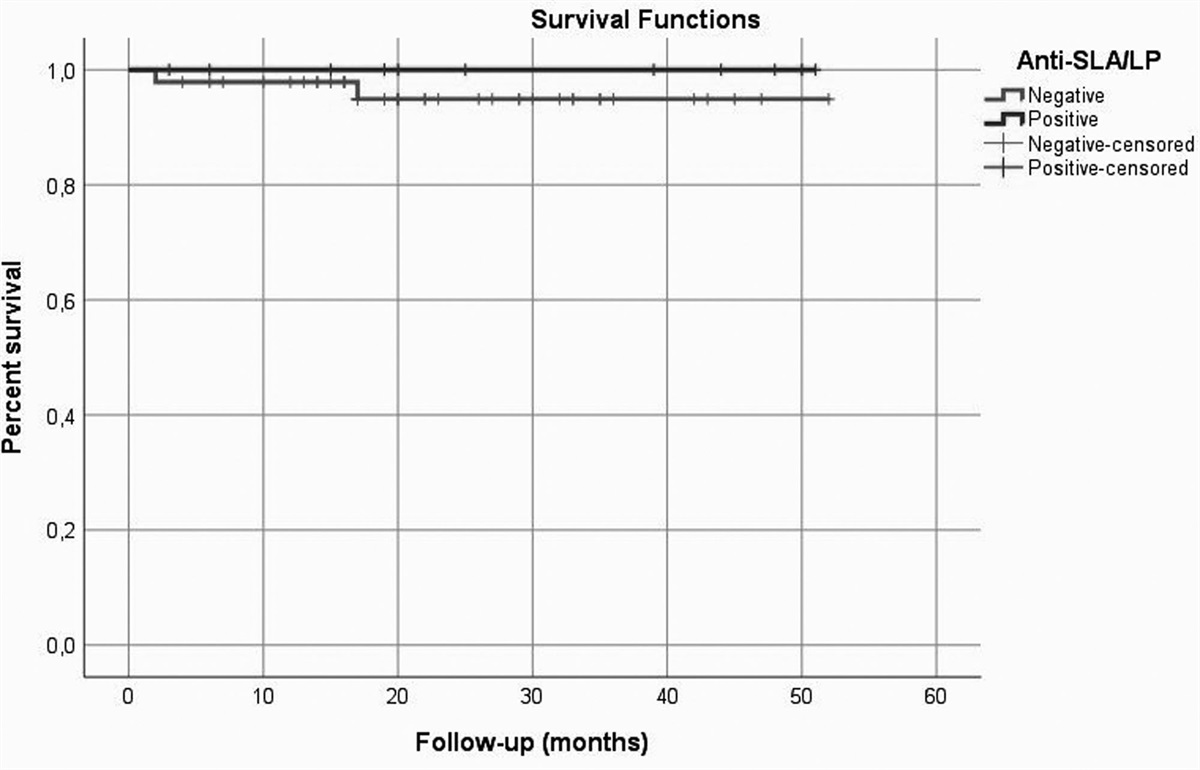
At 1, 3 and 5 years, the OS was 100, 83.9 and 60.3% in the late recurrence group and 85.5, 24.4 and 20.9% (P < 0.001) in the early recurrence group, respectively (Fig. 2).
 Fig. 2.:
Fig. 2.: Kaplan–Meier estimates of overall survival (OS) for patients between the late recurrence group and early recurrence group.
Clinical and pathological factors affecting early recurrenceUnivariate Cox regression analysis showed that sex, age, history of hepatitis B, antiviral therapy, Child grade, preoperative TACE, number of tumors, macrovascular invasion and satellite nodules had no significant relationship with early recurrence of HCC (all P > 0.05, Table 1). However, preoperative AFP level (P < 0.001), intraoperative blood transfusion (P = 0.014), tumor diameter (P < 0.001), MVI (P < 0.001), degree of tumor differentiation (P = 0.001) and pathological type (P < 0.001) were associated with early recurrence of HCC. Multivariate Cox regression analysis showed that preoperative AFP level ≥400 ng/ml [hazard ratio (HR) = 2.18; 95% confidence interval (CI), 1.36–3.46; P = 0.001], tumor diameter ≥5 cm (HR = 1.66; 95% CI, 0.99–2.78; P = 0.009), MVI (HR = 1.97; 95% CI, 1.21–3.22; P = 0.007) and MTM-HCC (HR = 2.04; 95% CI, 1.27–3.27; P = 0.003) were independent risk factors for early postoperative recurrence of HCC (Table 2).
Table 1. - Univariate cox regression analysis predictors early recurrence of hepatocellular carcinoma Factor Early recurrence group (n = 83) Nonrecurrence group (n = 231) HR (95% CI) P value Sex Male:female 73:10 185:76 1.62 (0.84–3.14) 0.15 Age (years) <65:≥65 63:20 149:82 0.63 (0.38–1.04) 0.068 HBV Positive:negative 61:22 167:64 0.96 (0.75–1.22) 0.73 Antiviral therapy Yes:no 25:58 95:136 0.74 (0.46–1.18) 0.20 AFP (ng/ml) <400:≥400 43:40 187:44 2.97 (1.93–4.56) <0.001 Child-Pugh A:B 80:3 226:5 0.78 (0.44–1.38) 0.39 Preoperative TACE Yes:no 9:74 21:210 0.91 (0.64–1.28) 0.57 Blood transfusion Yes:no 21:62 30:201 1.86 (1.13–3.04) 0.014 Tumor diameter (cm) <5:≥5 34:49 157:74 2.64 (1.70–4.09) <0.001 Number of tumors Single:multiple 63:20 195:36 0.78 (0.61–1.01) 0.055 MVI Negative:positive 27:56 148:83 3.17 (2.00–5.02) <0.001 Tumor differentiation Well:poorly 41:42 161:70 1.46 (1.18–1.81) 0.001 Macrovascular invasion Negative:positive 79:4 227:4 2.24 (0.82–6.12) 0.12 Satellite nodules Negative:positive 72:11 204:27 0.98 (0.52–1.85) 0.095 Histopathological MTM:non-MTM 37:46 33:198 3.42 (2.21–5.27) <0.001AFP, alpha-fetoprotein; CI, confidence interval; HBV, hepatitis B virus; HR, hazard ratio; MVI, microvascular invasion; MTM, macrotrabecular-massive; TACE, transcatheter arterial chemoembolization.
AFP, alpha-fetoprotein; CI, confidence interval; HCC, hepatocellular carcinoma; HR, hazard ratio; MVI, microvascular invasion; MTM, macrotrabecular-massive.
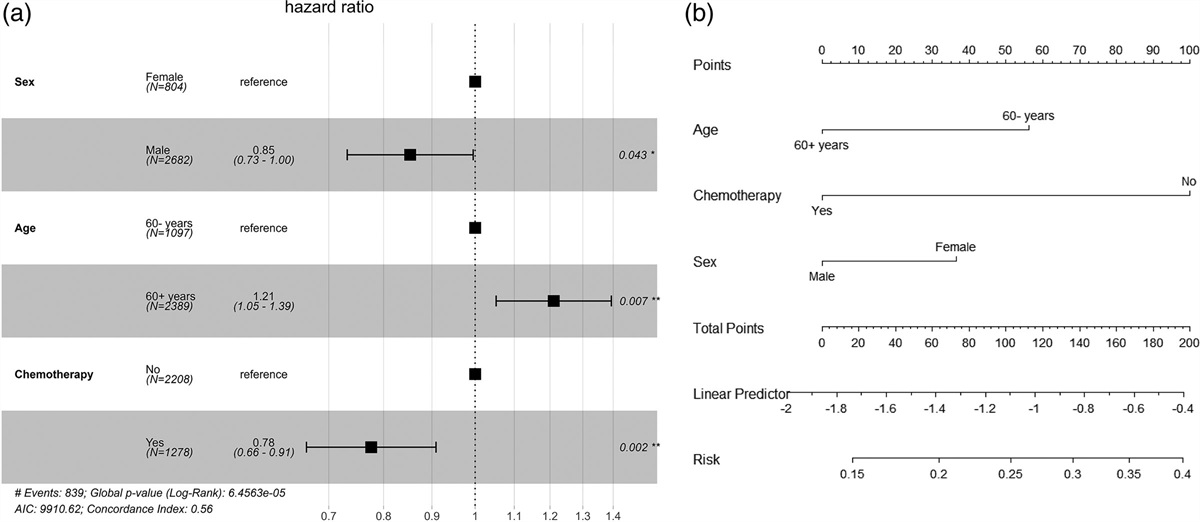
According to the independent risk factors, we developed a nomogram to predict HCC early recurrence based on the AFP level, tumor diameter, MVI and MTM-HCC (Fig. 3a). The concordance index was 0.74 (95% CI, 0.69–0.79) with 1000 bootstrap samples for predicting early recurrence (Fig. 3b). DCA analysis revealed that the nomogram model could augment net benefits and exhibited a wider range of threshold probability than the AJCC T stage and BCLC stage (Fig. 4).
 Fig. 3.:
Fig. 3.: Developed prognosis nomogram model for 1-year RFS. (a) Nomogram for predicting the 1-year probability of RFS. (b) Calibration curve plots of the nomogram. RFS, recurrence-free survival.
 Fig. 4.:
Fig. 4.: The decision curve analysis for the developed nomogram model.
ROC curve analysis was performed to compare the predictive abilities of our nomogram and conventional HCC staging (Fig. 5). Our nomogram [area under the curve (AUC), 0.767; 95% CI, 0.706–0.828] had better predictive accuracy than the BCLC (AUC, 0.618; 95% CI, 0.543–0.693) and AJCC staging systems (AUC, 0.654; 95% CI, 0.581–0.727). The sensitivity was 68.7%, and the specificity was 72.7%, respectively.
 Fig. 5.:
Fig. 5.: ROC analysis of recurrence-free survival at 1 year using the nomograms, and the MVI, tumor size, MTM, AFP and the AJCC T staging, BCLC staging. The AUC for our model (AUC, 0.767; 95% CI, 0.706–0.828) developed for recurrence-free survival was significantly higher than those for the BCLC (AUC, 0.618; 95% CI, 0.543–0.693) and AJCC staging systems (AUC, 0.654; 95% CI, 0.581–0.727). AFP, alpha-fetoprotein; AJCC, American Joint Committee on Cancer; AUC, area under the curve; BCLC, Barcelona Clinic Liver Cancer; CI, confidence interval; MVI, microvascular invasion; MTM, macrotrabecular-massive; ROC, receiver operating characteristic.
DiscussionRecurrence, especially early recurrence is the main problem affecting the treatment of liver cancer. However, the definition of early recurrence is still controversial. In previous studies, recurrence within 6 months, 1 year and 2 years after surgery has been defined as early recurrence respectively [11,16,17]. Hirokawa et al. [17] found that patients with recurrence within 6 months after surgery are associated with poorer survival. Liu et al. [11] found that nearly 2/3 of patients had a postoperative recurrence of HCC within 1 year, and early recurrence was a risk factor for patient prognosis. It has also been shown that recurrence within 2 years after surgery is associated with tumor MVI and the presence of satellite lesions, whereas recurrence after 2 years is associated with a background of liver disease [16]. In this study, a total of 152 patients developed recurrence after surgery, of which 83 (54.6%) had recurrence within 1 year, the prognosis of these patients was poor significantly than those with recurrence of more than 1 year. Therefore, we defined postoperative recurrence within 1 year as early recurrence.
A large number of studies have been conducted to identify the high-risk factors affecting early postoperative recurrence of HCC, such as tumor size, tumor number, tumor differentiation, MVI, AFP level and Protein Induced by Vitamin K Absence or Antagonist II (PIVKA-II) level [6,18,19]. However, there are few reports on the effect of the MTM-HCC HCC pathological type on early postoperative recurrence of HCC [8,9,14,15,20], and the predictive value of the histological type has not received much attention from the general public. MTM-HCC is more aggressive than other types of HCC, showing more vascular invasion (including large vessels and microvessels), low differentiation and high proliferation, and it is an independent risk factor for early recurrence and total recurrence [8,9]. The MTM-HCC incidence rate of approximately 7–18% has been reported in different studies [8,9,15,21,22]. In our study, 88 (23.0%) patients of MTM-HCC were identified among 383 patients, MTM was the independent risk factor of early recurrence (HR = 2.04). In the present study, Ziol et al. [9] reported that MTM-HCC was identified in 16% of 237 resected HCCs and the MTM-HCC subtype was an independent predictor of early recurrence (HR = 2.37). Calderaro et al. [8] found that MTM-HCC represented 10% of the HCCs, and MTM-HCC was significantly associated with early tumor relapse (HR = 1.70) in multivariate analysis.
Calderaro et al. [8] further found that the genotype of MTM-HCC showed more TP53 mutations, FGF19 amplification and activation of the angiogenic pathway compared to other types of HCC, and TP53 mutations were associated with cell proliferation, epithelial-mesenchymal transition and activation of angiogenesis [8], which may be the cause of the aggressiveness of MTM-HCC. Liu et al. [23] found that Programmed death ligand 1 (PD-L1) and CKLF like MARVEL transmembrane domain containing 6 (CMTM6) expression was significantly high in MTM-HCC, whereas CMTM6 promoted PD-L1 expression in tumor cells to counteract T cells [24], further leading to immunosuppression in the tumor microenvironment, so immunotherapy in MTM-HCC patients might achieve better efficacy, which also needs to be verified in future studies.
AJCC and BCLC staging are currently the most commonly used international staging criteria for HCC. However, these traditional staging criteria have unsatisfactory results in predicting postoperative recurrence, and several studies have reported that nomograms are better than traditional HCC staging criteria [25–27]. Cho et al. [25] constructed a column line diagram for predicting postoperative recurrence of HCC based on patient age, AFP level, surgical bleeding, incisional margin status, tumor size and satellite lesions, and Liu et al. [11] constructed a nomogram based on the Tumor Node Metastasis (TNM) stage and risk score model for predicting 1-year recurrence. Yang et al. [26] constructed a new nomogram for predicting the recurrence of HCC after surgery based on traditional prognostic indicators combined with various serological indicators. However, no study has developed a nomogram based on MTM pathological type, so the role of pathological type in predicting postoperative recurrence has not been examined. Our study was the first to develop a nomogram based on MTM-HCC, tumor size, AFP level and MVI. The performance of this new MTM-based nomogram [C-index: 0.74 (95% CI, 0.68–0.81)] was superior to that of the AJCC and BCLC staging systems, and it was also superior to that of the nomogram developed based on traditional prognostic indicators such as AFP, tumor size, tumor differentiation and MVI [25–27]. Therefore, our MTM-based nomogram can more accurately predict the probability of early postoperative recurrence of patients and can be used to more precisely develop individualized follow-up and adjuvant treatment strategies for each patient.
Of course, there are limitations to our study. First, this was a single-center retrospective cohort, which makes it prone to selection bias. Second, our MTM-based nomogram performed internal validation solely, lacks external or multicenter validation, and additional multicenter, large-sample studies are needed to validate the predictive ability of the MTM-based nomogram for clinical application. Finally, the heterogeneity of postoperative treatment also has an impact on HCC recurrence.
In conclusion, our study found that tumor size, AFP level, MTM and MVI are independent risk factors affecting the early recurrence of HCC after surgical resection, and the proposed nomogram based on MTM can effectively predict early postoperative recurrence of HCC, which can aid in the formulation of appropriate follow-up and adjuvant treatment strategies for patients after HCC surgery.
AcknowledgementsThe authors are grateful to the patients and doctors who assisted in the study.
The study was funded by Ningbo Health Branding Subject Fund (PPXK2018-03); Ningbo Natural Science Foundation of China (2019A610214) and Ningbo Municipal Natural Science Foundation (2022J262).
Conflicts of interestThere are no conflicts of interest.
References 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68:394–424. 2. Bruix J, Reig M, Sherman M. Evidence-Based diagnosis, staging, and treatment of patients with hepatocellular carcinoma. Gastroenterology 2016; 150:835–853. 3. Dhir M, Melin AA, Douaiher J, Lin C, Zhen WK, Hussain SM, et al. A review and update of treatment options and controversies in the management of hepatocellular carcinoma. Ann Surg 2016; 263:1112–1125. 4. Sugawara Y, Hibi T. Surgical treatment of hepatocellular carcinoma. Biosci Trends 2021; 15:138–141. 5. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet (London, England) 2018; 391:1301–1314. 6. Jung SM, Kim JM, Choi GS, Kwon CHD, Yi NJ, Lee KW, et al. Characteristics of early recurrence after curative liver resection for solitary hepatocellular carcinoma. J Gastrointest Surg 2019; 23:304–311. 7. Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, Schirmacher P, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020; 76:182–188. 8. Calderaro J, Couchy G, Imbeaud S, Amaddeo G, Letouzé E, Blanc JF, et al. Histological subtypes of hepatocellular carcinoma are related to gene mutations and molecular tumour classification. J Hepatol 2017; 67:727–738. 9. Ziol M, Poté N, Amaddeo G, Laurent A, Nault JC, Oberti F, et al. Macrotrabecular-massive hepatocellular carcinoma: a distinctive histological subtype with clinical relevance. Hepatology (Baltimore, Md.) 2018; 68:103–112. 10. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis 1999; 19:329–338. 11. Liu H, Yan Y, Chen R, Zhu M, Lin J, He C, et al. Integrated nomogram based on five stage-related genes and TNM stage to predict 1-year recurrence in hepatocellular carcinoma. Cancer Cell Int 2020; 20:140. 12. Ang SF, Ng ES, Li H, Ong YH, Choo SP, Ngeow J, et al. The Singapore Liver Cancer Recurrence (SLICER) score for relapse prediction in patients with surgically resected hepatocellular carcinoma. PLoS One 2015; 10:e0118658. 13. Xu W, Li R, Liu F. Novel prognostic nomograms for predicting early and late recurrence of hepatocellular carcinoma after curative hepatectomy. Cancer Manage Res 2020; 12:1693–1712. 14. Renne SL, Woo HY, Allegra S, Rudini N, Yano H, Donadon M, et al. Vessels Encapsulating Tumor Clusters (VETC) is a powerful predictor of aggressive hepatocellular carcinoma. Hepatology (Baltimore, Md.) 2020; 71:183–195. 15. Jeon Y, Benedict M, Taddei T, Jain D, Zhang X. Macrotrabecular hepatocellular carcinoma: an aggressive subtype of hepatocellular carcinoma. Am J Surg Pathol 2019; 43:943–948. 16. Imamura H, Matsuyama Y, Tanaka E, Ohkubo T, Hasegawa K, Miyagawa S, et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J Hepatol 2003; 38:200–207. 17. Hirokawa F, Hayashi M, Asakuma M, Shimizu T, Inoue Y, Uchiyama K. Risk factors and patterns of early recurrence after curative hepatectomy for hepatocellular carcinoma. Surg Oncol 2016; 25:24–29. 18. Hong YM, Cho M, Yoon KT, Chu CW, Yang KH, Park YM, et al. Risk factors of early recurrence after curative hepatectomy in hepatocellular carcinoma. Tumour Biol 2017; 39:1010428317720863. 19. Yamamoto Y, Ikoma H, Morimura R, Konishi H, Murayama Y, Komatsu S, et al. Optimal duration of the early and late recurrence of hepatocellular carcinoma after hepatectomy. World J Gastroenterol 2015; 21:1207–1215. 20. Sessa A, Mulé S, Brustia R, Regnault H, Galletto Pregliasco A, Rhaiem R, et al. Macrotrabecular-massive hepatocellular carcinoma: light and shadow in current knowledge. J Hepatocell Carcinoma 2022; 9:661–670. 21. Rastogi A, Maiwall R, Ramakrishna G, Modi S, Taneja K, Bihari C, et al. Hepatocellular carcinoma: clinicopathologic associations amidst marked phenotypic heterogeneity. Pathol Res Pract 2021; 217:153290. 22. Rhee H, Cho ES, Nahm JH, Jang M, Chung YE, Baek SE, et al. Gadoxetic acid-enhanced MRI of macrotrabecular-massive hepatocellular carcinoma and its prognostic implications. J Hepatol 2021; 74:109–121. 23. Liu LL, Zhang SW, Chao X, Wang CH, Yang X, Zhang XK, et al. Coexpression of CMTM6 and PD-L1 as a predictor of poor prognosis in macrotrabecular-massive hepatocellular carcinoma. Cancer Immunol Immunother: CII 2021; 70:417–429. 24. Burr ML, Sparbier CE, Chan YC, Williamson JC, Woods K, Beavis PA, et al. CMTM6 maintains the expression of PD-L1 and regulates anti-tumour immunity. Nature 2017; 549:101–105. 25. Cho CS, Gonen M, Shia J, Kattan MW, Klimstra DS, Jarnagin WR, et al. A novel prognostic nomogram is more accurate than conventional staging systems for predicting survival after resection of hepatocellular carcinoma. J Am Coll Surg 2008; 206:281–291. 26. Yang J, Bao Y, Chen W, Duan Y, Sun D. Nomogram based on systemic immune inflammation index and prognostic nutrition index predicts recurrence of hepatocellular carcinoma after surgery. Front Oncol 2020; 10:551668. 27. Shim JH, Jun MJ, Han S, Lee YJ, Lee SG, Kim KM, et al. Prognostic nomograms for prediction of recurrence and survival after curative liver resection for hepatocellular carcinoma. Ann Surg 2015; 261:939–946.
留言 (0)