
記住我

Early gastric cancer (EGC) is defined as gastric cancer confined to the mucosa or submucosa, regardless of the presence or absence of lymph node metastasis. With improvements in endoscopic technology in recent years, endoscopic submucosal dissection (ESD) has become the standard treatment for EGC because it preserves gastric function, causes less trauma, and shortens hospital stays [1]. The 5-year overall survival (OS) rate for EGC patients who underwent curative resection was over 90% [2]. However, ESD can only be as effective as surgery under the condition that a curative resection is performed. According to previous studies, there are still 24.6–39.5% of patients with non-curative resection (NCR) [3–5] who face the risk of local recurrence and lymph node metastasis and may require additional gastrectomy. Previous studies have identified tumor size, depth of infiltration, gender, presence of ulceration, certain endoscopic findings, and postoperative pathologic results as independent risk factors for NCR [6,7]. However, the features listed above were either lacking in specificity or could only be obtained after the ESD procedure. A simple and objective indicator to help endoscopists assess the risk of NCR before ESD and choose the most suitable treatment for patients individually has yet to be discovered.
Studies have shown that inflammation plays a significant role in carcinogenesis, tumor invasion, and migration [8,9]. Some inflammation indices, such as neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been shown to have great prognostic value in various cancer patients [10,11]. The systemic immune-inflammation index (SII), an inflammation index based on platelet, neutrophil, and lymphocyte, has been shown to be more accurate than other inflammation indices in predicting the prognosis of gastric cancer patients [12]. However, the majority of studies on SII focused on patients with advanced gastric cancer who underwent gastrectomy, whereas the efficacy of SII in predicting the prognosis and NCR risk of EGC patients remains to be determined [13]. Therefore, we conducted a retrospective analysis of the predictive value of SII for NCR of EGC patients.
Materials and methods PatientsWe reviewed data from patients who underwent ESD at the Department of Gastroenterology, Affiliated Hospital of Qingdao University between October 2013 and March 2021. Inclusion criteria included gastric adenocarcinoma confirmed by postoperative histopathology; availability of all clinical and pathologic data; and no prior chemotherapy, radiotherapy, or immunosuppressive treatment.
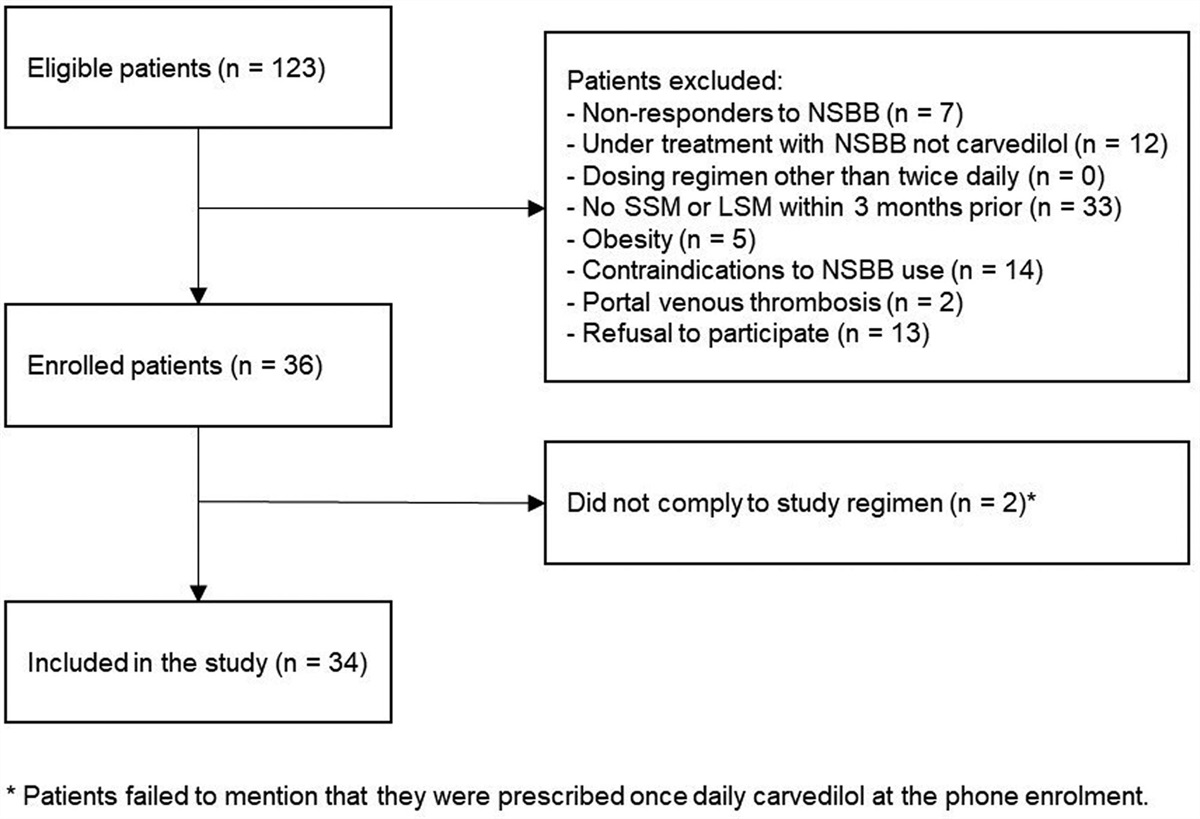
Patients were excluded if any of the following conditions were met: history of other malignant tumors; history of gastrectomy due to gastric carcinoma; and clinical evidence of infection, cardiovascular disease, or systemic inflammatory disease. The study design is shown in Fig. 1.
 Fig. 1.:
Fig. 1.: Study design. A total of 326 patients, including both the curative and non-curative resection groups, were reviewed retrospectively.
Data collectionThe following data were collected from our hospital’s medical record database: age, sex, expense and length of hospitalization, endoscopic features (tumor location, tumor size, and gross type), pathologic features (depth of invasion, lymphatic invasion, vascular invasion, horizontal margin, vertical margin, histological type, and tumor differentiation), preoperative serum carcinoembryonic antigen (CEA), neutrophil count, lymphocyte count, and platelet count. Preoperative blood samples (neutrophil, lymphocyte, mono, and platelet) were collected within 7 days prior to ESD. SII was calculated using the formula platelet × neutrophil/lymphocyte (109/L). PLR and NLR were calculated using the formulas platelet/lymphocyte and neutrophil/lymphocyte, respectively. Cutoff values for age, tumor size, and CEA were set according to previously published studies.
Written consent was obtained from all patients prior to ESD. This study was approved by the ethics committee of the Affiliated Hospital of Qingdao University.
Endoscopic submucosal dissectionThe ESD procedure involves marking the surrounding area of the lesion, submucosal injection of saline solution to lift the lesion, circumferential incision around the marking sites, and submucosal dissection. All ESD procedures were performed by a senior endoscopist with experience in over 100 gastric ESDs or by a junior endoscopist under the supervision and guidance of an experienced senior endoscopist. The main device used for ESD was the FLUSH knife (Olympus, Tokyo, Japan).
Gross and pathologic evaluationAccording to the Japanese Gastric Cancer Association Classification, lesions were categorized into three types (elevated, depressed, and flat) [14]. Endoscopically tumor size and location were also observed and reported. Before a general histological assessment, each specimen was fixed in 10% formalin and serially sectioned at 2 mm intervals. Before general assessment, all slides were stained with hematoxylin-eosin, which included the depth of invasion, lesion size, lymphatic and vascular invasion, and tumor involvement on lateral and vertical margins. Well-differentiated adenocarcinoma (tub1) or moderately differentiated adenocarcinoma (tub2) was defined as the differentiated type, whereas poorly differentiated adenocarcinoma (por) or signet ring carcinoma (sig) was defined as the undifferentiated type [1]. EGC with a mixture of differentiated and undifferentiated type components was classified based on the histological predominance.
Evaluation of resection efficacyEn-bloc resection is defined as the removal of a lesion in a single piece without any fragments (complete resection is achieved when histopathological examination confirms that a tumor is free of horizontal and vertical margin invasion after an en-bloc resection). According to the guidelines published by the Japanese Gastric Cancer Association (JGCA), curative resection is defined as en bloc resection without evidence of margin invasion or lymphatic/vascular involvement. The criteria are as follows: predominantly differentiated type, regardless of size, pT1a, without ulceration; predominantly differentiated type, ≤3 cm, pT1a, with ulceration; predominantly undifferentiated type, pT1a, ≤2 cm, without ulceration; and predominantly differentiated type, tumor size ≤3 cm, pT1b (SM1, <500 µm from the muscularis mucosa). NCR is defined as the failure of resection to meet any of the above criteria [1]. The endoscopic curability of patients was also divided into endoscopic curability A (eCura A), endoscopic curability B (eCura B), and endoscopic curability C (eCura C) according to the guideline of JGCA to help decide whether additional gastrectomy should be performed after NCR. All patients that were rated as eCura C were advised to receive surgical treatment.
Statistical analysisContinuous variables are presented as the mean ± SD. Categorical variables are represented as numbers with percentages. The area under the receiver operating characteristic (ROC) curve (AUC) was used to investigate the prognostic value of SII, PLR, and NLR. The Youden Index was used to determine the optimal cutoff values for SII, PLR, and NLR. A χ2 test was used to categorize the factors associated with the NCR of ESD in a univariate analysis. Variables with P < 0.05 were further included in the multivariate analysis using a binary logistic analysis to identify independent risk factors for NCR. Following that, a nomogram was constructed based on the logistic regression influence factors. Validation of this nomogram included evaluation of discrimination and calibration. We applied the concordance index and the AUC to assess the discriminative ability of the nomogram. The AUC was calculated by running the predictive model through a ROC curve. The AUC or concordance index of 0.5 indicates that the model has no predictive effect, while the AUC or concordance index of 1.0 indicates that there is perfect concordance between the actual results and those predicted by the model. Calibration was carried out using the bootstrap method, which consisted of 1000 bootstrap sample corrections. Variables with P < 0.05 were considered statistically significant. All the calculations were carried out using the latest version of SPSS software, version 26.0 (SPSS, Chicago, Illinois, USA). The nomogram was constructed and validated using R Software 4.0.4 (www.r-project.org).
Results Baseline characteristics and follow-up dataA total of 326 patients who underwent ESD were enrolled, with 232 being male and 94 female. The average age was 63 years (ranging from 39 to 91 years). The number of curative resections was 251 (76.99%). Among the 75 patients (23.01%) who were unable to undergo curative resection, 3 were not resected en bloc. Twenty-six patients underwent additional gastrectomy within 3 months of ESD, the rest 49 patients refused to undergo additional treatment of any kind. Recurrence was detected in 1 patient 4 years after ESD, and no sign of local recurrence or tumor metastasis was observed in the rest 48 patients until March 2021.
Receiver operating characteristic analysisThe ROC analysis was conducted to determine the optimal cutoff value for each inflammation index, with non-curative resection serving as the endpoint. The optimal cutoff value for each index with the highest sensitivity and specificity was 1.21, 140, and 414.8 for NLR, PLR, and SII, respectively: (sensitivity and specificity: 0.918 and 0.249, 0.425 and 0.775, and 0.562 and 0.648 for NLR, PLR, and SII, respectively). And patients were grouped based on the SII cutoff value for further investigation [SII ≤ 414.8 (low) and SII > 414.8 (high)]. Figure 2 shows the ROC curve for each index.
 Fig. 2.:
Fig. 2.: ROC curves for SII, PLR, and NLR. AUC, area under the receiver operating characteristic (ROC) curve; PLR, platelet-to-lymphocyte ratio; NLR, lymphocyte ratio; SII, systemic immune-inflammation index.
Comparison between inflammation indicesThe AUC was used to compare the prognostic value of all inflammation indices for non-curative resection. The AUC for non-curative resection of SII, NLR, and PLR was 0.611, 0.602, and 0.593, respectively (sensitivity: 0.918, 0.425, and 0.562, and specificity: 0.249, 0.775, and 0.648 for NLR, PLR, and SII, respectively), indicating that the prognostic value of SII for NCR is superior to that of NLR and PLR.
Relationship between preoperative systemic immune-inflammation index and clinicopathological factorsAs shown in Table 1, the high SII group was more prone to developing a non-curative resection than the low SII group. (Χ2 = 10.832, P = 0.001). A higher SII was also correlated with larger tumors, male gender, older age, submucosal invasion, a higher eCura grade, and larger hospital expenses. The difference was statistically significant (P < 0.05). There was no between-group difference in tumor localization, ulceration, differentiation, or gross type, which is consistent with previous studies [12,15].
Table 1. - The relationship between preoperative systemic immune-inflammation index and clinicopathological features Parameters Number (%) Low SII < 414.87 High SII ≥ 414.87 χ 2 P Cases (n) 326 n = 197 n = 129 Age 0.356 0.551 >65 133 (40.8) 87 46 <65 193 (59.2) 120 73 Sex 4.457 0.035 Male 232 (71.2) 139 93 Female 94 (28.8) 68 26 Location 0.126 0.939 Upper 1/3 29 (8.9) 18 11 Middle 1/3 129 (39.6) 79 50 Lower 1/3 168 (51.5) 100 68 Size 6.165 0.013 >3cm 43 (13.2) 20 23 <3cm 280 (86.8) 187 96 CEA (ng/mL) 4.883 0.057 >2.34 113 (34.7) 59 54 <2.34 213 (65.3) 138 75 Differentiation 0.671 0.715 Poorly differentiated 71 (21.8) 40 31 Moderately differentiated 136 (41.7) 83 53 Well differentiated 119 (36.5) 74 45 Depth of invasion 5.069 0.024 Mucosa 267 (81.9) 169 98 Submucosa 59 (18.1) 28 31 Gross type 3.550 0.169 Elevated 164 (50.3) 101 63 Flat 19 (5.8) 9 10 Depressed 143 (43.9) 97 46 BMI (kg·m2) 0.694 0.405 <25 196 (60.1) 128 68 >25 130 (29.9) 79 51 Sex 4.457 0.035 Male 232 (71.2) 139 93 Female 94 (28.8) 68 26 Ulceration 0.023 0.880 Yes 39 (12.0) 24 15 No 287 (88.0) 173 114 PLR <140.08 240 (73.6) 180 60 80.772 <0.001 >140.08 86 (26.4) 17 69 NLR <1.21 69 (21.2) 68 1 53.192 <0.001 >1.21 257 (78.8) 129 128 Hospital stay (days) 0.201 0.654 <7 197 (60.4) 133 64 >7 129 (39.6) 84 45 Hospital expense (CHY) 5.763 0.016 <28 688 196 (60.1) 142 54 >28 688 130 (39.9) 78 52 Curability of endoscopic resection (eCura) 9.815 0.007 A 211 (64.7) 144 67 B 40 (12.3) 26 14 C 75 (23.0) 36 39 Non-curative resection 9.663 0.002 Yes 251 (76.9) 170 81 No 75 (23.1) 36 39CNY, Chinese Yuan; NLR, lymphocyte ratio; SII, systemic immune-inflammation index.
According to univariate analysis, patients with non-curative resection were more likely to have larger tumors, a poorly differentiated histological type, elevated CEA, PLR, SII, and NLR levels, and an increased risk of submucosal infiltration than patients with curative resection. Patients who underwent non-curative resection had a high tendency to develop upper stomach tumors [6,16]. As for the multivariate analysis, we found that higher SII [odds ratio (OR) = 1.003, P = 0.001], PLR (OR = 1.009, P = 0.019), NLR (OR = 1.043, P = 0.029), larger tumor size (OR = 2.055, P < 0.001), tumor on the upper third of the stomach (OR = 16.393, P < 0.001), poorly differentiated type (OR = 29.754, P < 0.001), ulceration (OR = 4.814, P = 0.001), and submucosal invasion (OR = 48.91, P < 0.001) were associated with NCR and could be considered as the independent risk factors (Table 2).
Table 2. - Comparative multivariate analysis of curative resection and non-curative resection Parameters Multivariate analysis OR 95% CI P value Tumor size (cm) 2.055 1.563 2.701 <0.001 CEA 1.083 0.911 1.289 0.366 SII 1.003 1.001 1.004 0.001 PLR 1.009 1.001 1.016 0.019 NLR 1.520 1.043 2.215 0.029 Location Lower 1/3 1 Middle 1/3 1.082 0.513 2.280 0.836 Upper 1/3 16.393 5.035 53.377 <0.001 Differentiation Well differentiated 1 Moderately differentiated 1.627 0.649 4.080 0.300 Poorly differentiated 29.754 10.655 83.090 <0.001 Ulceration No 1 Yes 4.814 1.846 12.566 <0.001 Infiltration depth <0.001 Mucosa 1 17.383 149.728 Submucosa 51.017CEA, carcinoembryonic antigen; CI, confidence interval; NLR, lymphocyte ratio; OR, odds ratio; SII, systemic immune-inflammation index.
The nomogram was built using independent variables derived from the binary logistic regression (SII, tumor size, location, ulceration, pathology, and depth of invasion). Since the depth of invasion can only be identified through pathological examination after ESD while all other four variables could be obtained during the evaluation before ESD, it was excluded when constructing this nomogram. Each variable was assigned a score on a point scale ranging from 0 to 100, and a total score for the prediction of NCR was calculated by adding the scores that each variable corresponds to (Fig. 3). The total points subsequently could be used to predict the probability of NCR by applying a vertical line to the ‘Risk of NCR’ scale as shown in Fig. 3. We also created a scoring table that combines all five variables to simplify this scoring system (Table 3). A calibration curve generated using the bootstrap method for internal validation (repetition of sample correction = 1000) demonstrated a high degree of concordance between the deviation correction prediction and the ideal interface line (Fig. 4). The AUC (95% confidence interval) of the ROC curve (Fig. 5) for discrimination evaluation was 0.858, and the concordance index of this nomogram was 0.942.
Table 3. - The scoring table based on the nomogram, the total points could be utilized to estimate the chance of non-curative resection in the nomogram SII <414.87 >414.87 Points 0 39 Size <2cm >2cm Points 0 51 ulceration Yes No Points 0 55 location Middle1/3 lower1/3 upper1/3 Points 0 1 82.5 Differentiation WellSII, systemic immune-inflammation index.
 Fig. 3.:
Fig. 3.: Nomogram for predicting non-curative resection in EGC patients undergoing ESD. EGC, early gastric cancer; ESD, endoscopic submucosal dissection; M, moderately differentiated adenocarcinoma; P, poorly differentiated adenocarcinoma; SII, systemic immune-inflammation index; W, well-differentiated adenocarcinoma.
 Fig. 4.:
Fig. 4.: Calibration curve of the nomogram. NCR, non-curative resection.
 Fig. 5.:
Fig. 5.: ROC curve for the nomogram. Area under the ROC curve (AUC) = 0.8578. ROC, receiver operating curve.
DiscussionInflammation, as one of the 10 hallmarks of cancer, has been linked to tumor growth, invasion, and metastasis [17]. Inflammatory cells such as neutrophils, platelets, and lymphocytes engage in this process through various pathways. As the most common kind of leukocyte in circulating blood, neutrophils were believed to be a protective factor against tumor invasion in most cases. However, recent studies have shown that a subset of neutrophils known as tumor-associated neutrophils can promote tumor growth and metastasis by secreting cytokines and chemokines such as matrix metalloproteinase-9, vascular endothelial growth factor, and hepatocyte growth factor [18–20]. They can also produce neutrophil extracellular traps to act as a carrier of circulating tumor cells, thereby facilitating tumor metastasis [19]. Platelets have also been shown to have pro-metastatic functions. Besides protecting tumor cells from natural killer cell attack, they can also promote epithelial to mesenchymal transition, which enhances the motility and aggressiveness of tumor cells and hence accelerates tumor metastasis [21,22]. Lymphoc
留言 (0)