
記住我
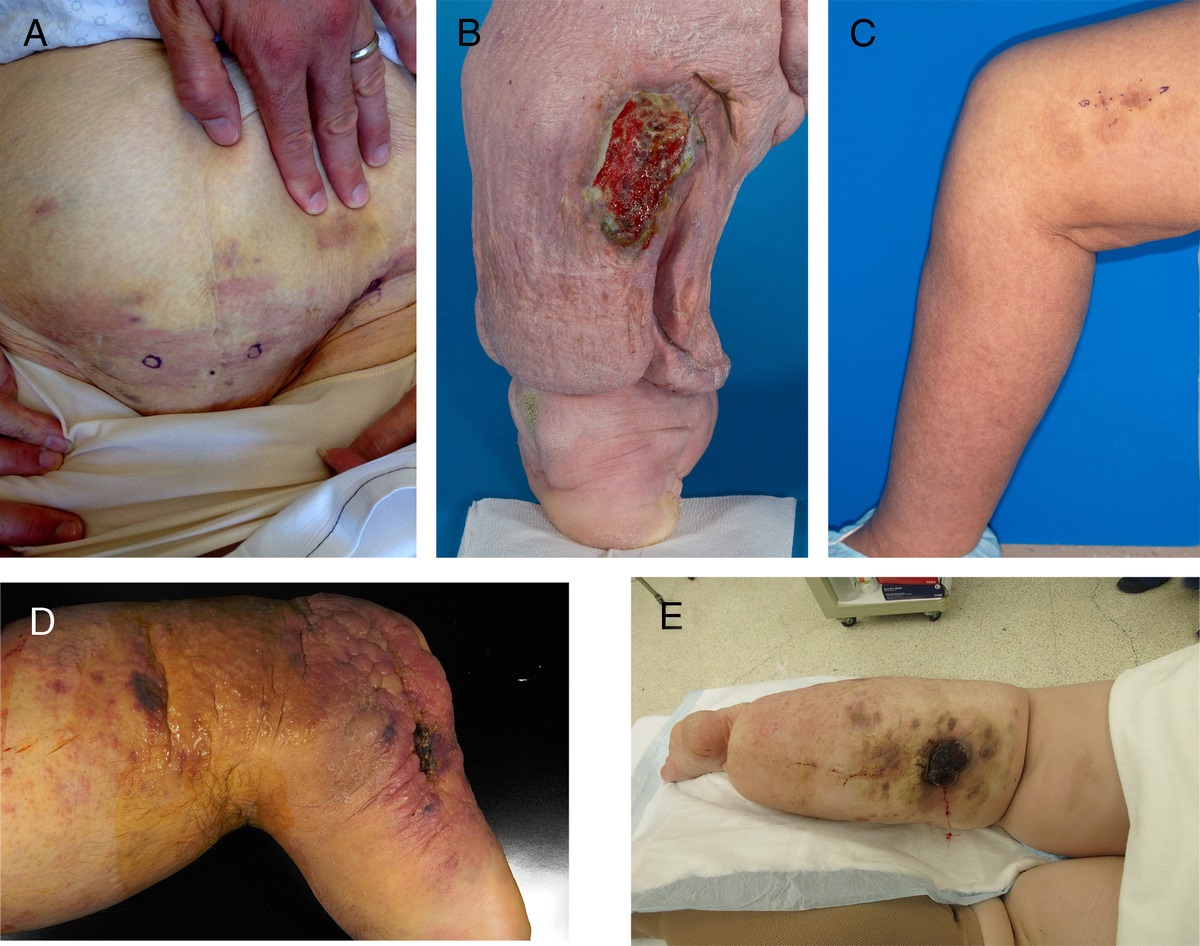
Patients at end of life (EOL) may experience avoidable and unavoidable skin breakdown prior to their death.1,2 Avoidable skin breakdown includes some pressure injuries (PIs), whereas unavoidable skin breakdown includes Kennedy terminal ulcers (KTUs),3 Trombley-Brennan terminal tissue injury (TB-TTI),4 skin failure,5 and Skin Changes At Life’s End (SCALE).6 Although the exact etiology of unavoidable skin injuries is unknown, it is theorized these skin changes occur because of hypoperfusion and multiorgan system failure.5,7 Since Kennedy’s3 seminal work on KTU, research in this area has been limited for several reasons, including the ongoing global debate on the existence of EOL wounds and confusion around their classification as PIs.5,8,9 However, many specialist clinicians and researchers consider terminal ulcers (TUs), which include KTU and TB-TTI, unavoidable injuries associated with dying.5,10,11 These TUs have characteristics and development patterns that distinguish them from PIs; however, few clinicians are aware of these differences.8,12,13 Terminal ulcers are pear-, horseshoe-, or butterfly-shaped red, black, or maroon skin ulcers/injuries that quickly develop in the absence of external pressure on the buttock, sacrum, spine, and extremities.8,9 Unlike most PIs, TUs can develop in a matter of hours from intact skin to a deep wound exposing muscle and bone and often develop in the months, weeks, days, or hours before death.8,9
Between 1989 and 2020, the reported TU prevalence and incidence data in various clinical settings were 2.7% to 55.7%.8,14 The limited number of studies and their poor methodological quality8,14 mean caution is required when interpreting or using this evidence. Compounding this, many TUs are misclassified and reported as PIs.5,10,15 A recent systematic review of patients receiving palliative care across all settings reported a PI prevalence and incidence of 12.4% and 11.7%, respectively.16 The authors acknowledged the existence of KTU in palliative patients; however, they did not include TU studies in their review.16 This highlights the potential inaccuracies of current data, with the review authors asserting the inclusion of palliative patients in PI reporting systems needs to be reviewed.16
Misclassifying TU has major implications for patients, clinicians, and organizations. For patients, families, and clinicians, TU care planning should focus on comfort care rather than wound healing. For individuals and organizations, regulatory and financial penalties may be imposed,12,17,18 along with potential legal implications related to malpractice or abuse.19,20
The lack of a TU classification system and assessment tool has unintended consequences for clinicians and researchers because it compels them to use tools designed for the assessment, classification, and subsequent reporting of PI.14,16,21 For example, care and management strategies for PI in individuals at EOL are described in the international PI clinical practice guidelines; however, care and management strategies for unavoidable injuries such as KTU and TB-TTI are not.22 Jakobsen and colleagues’14 multisite prospective observational study of patients with cancer in five Italian hospices used the international PI classification system to assess patients for KTU and to determine their incidence, highlighting a significant research and practice gap.
Having a TU assessment tool would contribute to the accurate collection of prevalence and incidence data and guide clinicians’ delivery of specialized treatment and management strategies, a position confirmed by researchers and experts.5 Accordingly, the aims of this study were to develop a TU wound assessment tool; gain consensus on TU definition, wound descriptors, and characteristics; and evaluate the tool’s content and face validity.23,24
METHODSUsing a modified online reactive Delphi technique (Figure 1), a draft TU wound assessment tool, developed by the research team and informed by the literature,8,9 was presented to the panel members. Delphi panels engage experts in a structured methodological approach to help answer clinical questions where limited evidence exists.25,26 This technique has previously been used in research into SCALE6 and PI27,28 and the definition of EOL,29 making it a suitable study method.
 Figure 1:
Figure 1: DELPHI PROCESS FLOWCHARTAbbreviations: EOL, end of life; KTU, Kennedy terminal ulcer; TU, terminal ulcer.
The panelists in this study were asked to anonymously “react” to the tool content post priori rather than asking the experts to suggest items for inclusion, as is the process in Delphi studies.25,26,30 A major benefit of this anonymous modified approach is the researchers’ ability to control conflicts in the experts’ opinions.30 An online approach was selected because the global dispersion of potential panel members and the COVID-19 pandemic restricted researchers’ ability to conduct face-to-face group interviews. Finally, construct validity was achieved through the experts’ item validation and agreement.31
This study followed the CREDES (Conducting and REporting DElphi Studies) checklist.32 Study approval was granted by the appropriate Human Research Ethics Committees (hospital: HREC/2020/QGC/54403; university: 2020/379).
Sample and RecruitmentAlthough there is no agreement concerning the exact number of Delphi panel members,23,33 six or more experts from the area under investigation are recommended.25,34 Recent reviews found limited published TU literature,8,9 restricting the pool of experts from which to draw; accordingly, investigators decided to include international experts in KTU, TU, PI, TB-TTI, and SCALE7,8 as potential panel members. Panel heterogeneity is paramount,33,35 so the aim was to recruit 12 to 15 global clinical/research experts, an achievable sample. The Delphi panel selection criteria included interdisciplinary members selected based on their clinical and/or research expertise in KTU, TU, TB-TTI, PI, and SCALE. Potential members were contacted in August 2020 via email or telephone. Willing experts received a study information sheet and link to the online anonymous survey via email. Launching and completing the online survey constituted consent.
Tool DevelopmentUsing an iterative process, the draft TU wound assessment tool presented to the Delphi panel was developed by the research team and informed by their published KTU and TU literature reviews.8,9 The draft tool consisted of five sections and a total of 20 items: instructions (two items), TU definition (one item), screening (six items), assessment (eight items), and management (three items). A shortened description of each item is presented in Table 1. The instructions provided clinical guidance on the use of the tool (eg, Do you suspect a TU or PI?). The TU definition was described as an unavoidable clinical phenomenon seen in some individuals at EOL and included KTU and TB-TTI.5,12,36 The screening section consisted of four questions aimed at distinguishing TU from PI: (1) receiving regular PI prevention care, (2) patient is actively dying as determined by the medical team, (3) sudden development of skin injury/ulcer, and (4) the absence of local skin trauma or pressure. A yes/no response was required for each question, with four “yes” responses needed to progress to the assessment section.
Table 1 - DELPHI ROUND ONE (N = 16) AND TU ASSESSMENT TOOL ITEMS (N = 20) No. Items Shortened Item Description Experts in Agreement, n (%) a Relevance I-CVI Experts in Agreement, n (%) a Importance I-CVI Average, Relevance, and Importance Clarity I-CVI Condition Action 2 Items Instructions 1 Use this assessment tool if you suspect a skin ulcer or blister is a TU and not a pressure injury/ulcer. 15 (93.6) 0.94 16 (100) 1.00 0.97 0.56 Met Reworded 2 Complete this assessment as frequently as necessary. 10 (62.5) 0.63 11 (68.8) 0.69 0.66 0.25 Revise Removed 1 Item TU definition 3 TUs are defined as an unavoidable clinical phenomenon seen in some dying individuals. TUs include KTUs and TB-TTI. 15 (93.6) 0.94 15 (93.6) 0.94 0.94 0.63 Met Retain 6 Items Screening 4 Patient receives regular pressure injury prevention strategies including repositioning. 15 (93.6) 0.94 15 (93.6) 0.94 0.94 0.56 Met Retain 5 Patient’s medical team assesses them as actively dying. 14 (87.5) 0.88 15 (93.6) 0.94 0.91 0.75 Met Retain 6 The patient develops reddish/purple skin discoloration, skin ulcer, or blister within the previous 2-8 h. 15 (93.6) 0.94 15 (93.6) 0.94 0.94 0.50 Met Retain 7 Absence of skin trauma or pressure to the area of skin breakdown or blistering. 12 (75.0) 0.75 15 (93.6) 0.75 0.75 0.44 Revise Removed 8 If you answered “yes” to ALL FOUR screening questions, proceed to Section 2 and complete the assessment. 11 (68.8) 0.69 12 (75.0) 0.75 0.72 0.69 Revise Reworded 9 Cease your assessment if you answer “no” to ANY of the screening questions because your patient does not currently meet the criteria for this tool. 12 (75.0) 0.75 12 (75.0) 0.81 0.78 0.63 Revise Removed 8 Items Assessment 10 Location(s): Coccyx, sacrum, or buttock (unilateral or bilateral), leg, heel, arm, shoulder, thoracic and lumbar spine 14 (87.5%) 0.88 14 (87.5%) 0.88 0.88 0.81 Met Retain 11 Appearance (one or combination): Bruise-like appearance; stages 2-4, etc 12 (75.0%) 0.75 12 (75.0%) 0.75 0.75 0.19 Revise Reworded 12 Skin intact: Skin may or may not be intact 13 (81.3%) 0.81 13 (81.3%) 0.81 0.81 0.63 Met Retain 13 Shape: Pear, horseshoe, butterfly (on sacrum), or linear 10 (62.5%) 0.63 10 (62.5%) 0.63 0.63 0.56 Revise Reworded 14 Color: Red, yellow, and black; pink, purple, or maroon; may have a white center 14 (87.5%) 0.88 13 (81.3%) 0.81 0.84 0.50 Met Reworded 15 Speed of change: Increase in reddish/purple skin discoloration, skin ulcer, or blister size within 2-8 h 14 (87.5) 0.88 14 (87.5) 0.88 0.88 0.69 Met Retain 16 Healing: Skin ulcer or blister does not resolve despite wound treatment 11 (68.8) 0.69 11 (68.8) 0.69 0.69 0.63 Revise Removed 17 If you answer “yes” to MOST of the TU descriptors in Section 2, contact your pressure injury/ulcer or wound specialist, or occupational therapist for confirmation. 11 (68.8) 0.69 11 (68.8) 0.69 0.69 0.50 Revise Reworded 3 Items Management 18 This section is to be completed by your pressure injury/ulcer or wound specialist or occupational therapist. 9 (56.3) 0.56 10 (62.5) 0.63 0.59 0.50 Revise Reworded 19 Is this a TU? (circle one): 14 (87.5) 0.88 15 (93.6) 0.94 0.91 0.94 Met Retain 20 TU management plan developed? (circle one): 14 (87.5) 0.88 13 (81.3) 0.81 0.84 0.56 Met RetainAbbreviations: I-CVI, item content validity index; KTUs, Kennedy terminal ulcers; TB-TTI, Trombley-Brennan terminal tissue injury; TU, terminal ulcer.
aAgreement was reached by expert selecting 3, “agree”, or 4, “strongly agree”, for the item.
The assessment section included TU descriptors related to the skin injury/ulcer location, appearance, intact skin, lesion shape and color, speed of wound change, and wound healing. A yes/no response was required for each descriptor, with an answer of “yes” to most items requiring referral to a wound specialist or occupational therapist. The management section was designed to be completed by the wound specialist or occupational therapist. They confirmed the presence of a TU and the development of a management plan.
Data CollectionData were collected in September and October 2020 (Figure 1). An online survey gathering quantitative and qualitative data was developed by the research team and deployed using their university’s online research survey tool (LimeSurvey software). Two anonymous, consecutive Delphi panel surveys, or rounds, were distributed to recruited experts.33 Those panel members who responded in round 1 were subsequently invited to participate in round 2. Each online survey was estimated to take 20 to 30 minutes to complete, with 3 weeks between each round, providing panel members with enough time to consider and return their responses. On day 10 of each round, an email reminder was sent to all participants. Feedback from round 1 informed the refinement of the tool items and round 2 survey.33 Although the Delphi method is an iterative process with the identification of participants known only to the research team,25 those participating in both rounds were offered the option to remain anonymous or be identified for acknowledgement in this publication.
Delphi panel members were invited to review and assess the TU wound assessment tool’s content and face validity, including the wound descriptors,37 location, stage, speed of development, current PI prevention care,12 and the patient’s healthcare status (dying/not dying).5 Panelists were asked to confirm the wound characteristics that do not constitute a TU and invited to suggest additional items for inclusion.
As recommended in CREDES,32 quantitative data were collected using a four-point Likert-type scale (strongly disagree-strongly agree) assessing each item’s relevance, importance, and clarity.38 A four-point scale for content items was used because it avoids the selection of a neutral midpoint.32,39 Open-ended questions were used to gather qualitative feedback on all sections and items in the tool. Demographic and professional data were also collected.
Data AnalysisValidity of the TU assessment tool items was tested using the content validity index (CVI),31 a recommended method to measure interrater agreement among Delphi panel members.38 Data analysis focused only on item-level CVI and not on scale (or tool)-level CVI. Defined a priori, the CVI of each survey item (item level CVI) was achieved when most panel members agreed on the inclusion of an item.31,34,40 Although some recommend a minimum CVI of 80%,41 regardless of the number of panel experts, a recommended item CVI greater than 78% is considered excellent.38 Therefore, items with an item CVI lower than 78% were considered items for revision, and those with very low values were considered for deletion.38
The item CVI for importance and relevance was calculated from the percentage of panel member ratings of 3 or 4 on the Likert scales (agree or strongly agree) for each item and then averaged across all the experts.38 The item CVI for clarity was used to help improve the items during revision. To reduce bias, reliability measures included the use of two Delphi rounds, the iterative nature of the survey, and the anonymity of the panel members.31
Descriptive statistics were used to describe the panel members’ demographic characteristics, including their professional role, and the number of years employed at their organization. The data were analyzed using IBM SPSS version 25.0. Open-ended text responses were analyzed using content analysis,42 and respondents’ feedback were used to refine the tool for re-review in round 2.
RESULTSTwenty-nine international wound experts within clinical, research, and/or education roles were invited to participate in the Delphi panel; 16 (55.2%) agreed. More than two-thirds (n = 10) of experts were PhD qualified, and some identified more than one area of wound expertise (Table 2). The average length of experience in their role was 27.6 ± 10.0 (range, 15-50) years. The panel members were predominately located in Australia (n = 7; 43.8%) and the US (n = 7; 43.8%).
Table 2 - DELPHI EXPERTS’ CHARACTERISTICS (N = 16) Characteristic n % Wound expert type Clinical 7 43.8 Research 5 31.3 Education 2 12.5 Clinical and researcher 1 6.3 Education and researcher 1 6.3 Area of expertise Pressure injuries 13 81.3 Kennedy terminal ulcers 5 31.3 Skin Changes At Life's End 5 31.3 Skin failure 4 25.0 General chronic wounds 3 18.8 Trombley-Brennan terminal tissue injuries 2 12.5 Psychometric evaluation 1 6.3 Education PhD 10 62.5 Master's degree 4 25.0 Diploma 1 6.3 Family nurse practitioner 1 6.3 Current role Wound consultant 5 31.3 Academic 5 31.3 Researcher 3 18.8 Clinician 2 12.5 Education 1 6.3 Location Australia 7 43.8 US 7 43.8 Ireland 1 6.3 The Netherlands 1 6.3Round 1 had a 100% (n = 16) survey response rate. The median time experts spent on the online survey was 32.3 minutes, with a range of 10 to 147 minutes. The quantitative summary of the results for round 1 is shown in Table 1.
From the initial 20 items reviewed by the panel, agreement for item relevance and importance ranged between 0.54% and 0.94%, whereas item clarity was scored 0.25% to 0.94%. Using a combined item CVI for relevance and importance with a cutoff 0.78 or higher,38 as well as the overall item CVI, four items were removed, and the wording revised for seven items (Table 1).
The research team used qualitative feedback from the panel to further refine the tool, including suggestions to (1) change the tool name to “EOL wound assessment tool;” (2) change the TU definition to an “EOL wound definition” including KTU, TU, and SCALE; and (3) organize the tool into three main sections (screening, assessment, and confirmation and management).
Round 2The 16 panelists in round 1 were invited to participate in round 2, with a response rate of 81.3% (n = 13). Because of the high round 1 consensus, panel members received a revised online survey asking for qualitative feedback only. Experts provided feedback on the EOL wound assessment tool instructions, definition, and three main sections (screening, assessment, and confirmation and management); the remaining revised items; and the overall presentation of the tool itself.
Five panel members (39.0%) reported that the tool instructions were clear and succinct. To improve the clarity of the EOL wound definition, eight panel members (62.0%) suggested removing the words “ulcer” and “skin intact” because of the potential association with the current PI classification system. From this feedback, the authors decided to only remove the word “ulcer” from the tool because EOL wounds can present as bruising with intact skin.
Nine panel members (69.0%) provided positive and affirmative comments on the screening questions, with seven (54.0%) suggesting minor rewording to screening questions 1 and 3. In the first screening question, three panel members (23.0%) recommended changing “actively dying” to “dying” to better reflect the potential time period up to months. In the third screening question, removing injury descriptors “reddish and purple” was suggested so a range of wound colors could be included. It was unanimously agreed (100%) that a yes response to all three screening questions was required to progress to the assessment section of the tool.
In the assessment section, eight panelists (62%) suggested no change, whereas two members (15%) proposed minor changes to the wound characteristics of shape, color, and speed of change. For wound shape, including “other shape” was recommended because this would encompass the range of shapes in which EOL wounds can present. In terms of wound color, the inclusion of “tissue darkening for dark skin tone individuals” was suggested. The words “rapid and sudden” were also added to the speed of change item.
Given the specific characteristics of EOL wounds, eight panel members (61.5%) concurred that two or more yes responses to the wound characteristics were sufficient for a clinician to progress to the confirmation and management section. Three panel members (23%) suggested two minor rewording changes in section 3. First, the inclusion of patients and families in care decisions was suggested, and second, the removal of the “not applicable” option for the development of a wound management plan was recommended.
Overwhelmingly, panel members provided positive feedback on the tool refinements, flow, and structure, with a few suggesting the development of a tool training manual: a document the research team was drafting. The final version of the EOL wound assessment tool is provided in Table 3.
 Table 3:
Table 3: END-OF-LIFE WOUND ASSESSMENT TOOL
DISCUSSIONSome patients develop EOL wounds in the months, weeks, days, and hours before their death.1,2 Recent reviews8,9 identified limited TU prevalence data, highlighting a compelling need for rigorous clinical research to facilitate the gathering of these data.16 The Delphi panel comprised international experts in KTU, TU, PI, TB-TTI, and SCALE.7,8 This was a major strength because their expertise in this little-known area helped to establish the face and content validity of the EOL wound assessment tool.43 The Delphi panel technique also enabled consensus by experts engaged in clinical care, academia, research, and education across four countries, increasing the tool’s clinical relevance and applicability.
The sample size of 16 international clinical/research experts exceeded our recruitment target of 12 to 15 people with a high panel retention rate between rounds (81.3% retained). This was particularly pleasing considering the study was conducted during the uncertainties associated with the first year of the global COVID-19 pandemic (2020) during which the health and safety of individuals were potentially impacted and drastic changes occurred in the living and work arrangements of many people. Keeney et al43 acknowledge that recruiting and retaining panelists are especially difficult because the Delphi technique “asks much more of respondents than a simple survey.” Therefore, the authors implemented several recruitment and retention strategies including personalized introductory contact (via email) that outlined a realistic time commitment and, as a way of ownership, acknowledging each potential panelist’s contribution to their field of expertise.24 Follow-up emails were also sent to nonresponders,43 and online support was offered to panelists by one of the researchers during each round.
The high level of panelist consensus achieved in round 1 suggests the researchers’ selection of the tool items accurately reflected current evidence.7–9 The second round qualitative comments were also closely aligned with many of the experts making similar suggestions for important word changes, particularly with the EOL wound definition. The experts’ suggestion to rename the tool from a TU wound assessment tool to an EOL wound assessment tool and improve the clarity of the EOL wound definition also reflects published literature in this area.7,29 Schüttengruber et al29 recently used a Delphi technique to reach a consensus on the definition of EOL involving criteria such as the variable nature of the EOL phase (months, days, hours), the inclusion of family, and the involvement of clinicians in providing individualized physical and psychosocial care. These criteria were also suggested by panelists for inclusion in the present tool.
The EOL wound assessment tool addresses several potential clinical, policy, financial, and legal issues for adults at EOL, their families, clinicians, and organizations. It is clear that some EOL wounds are misclassified as PI,5,10,15 increasing the uncertainty of the available prevalence and incidence data for EOL wounds. Gathering accurate data could be used to inform the appropriate allocation of scarce healthcare resources,14,18 which have been further stretched by the COVID-19 pandemic.44 An accurate diagnosis of unavoidable EOL wounds would enable clinicians to implement individualized, specialist wound and EOL care that is guided by the premise of comfort rather than healing.8,9 This would also avoid financial penalties,12,17 along with the associated legal and policy implications for families, clinicians, and organizations.7,19
Currently, many of the KTU and TU recommendations are based on level 4 evidence, highlighting the need for rigorous research into EOL wounds and clinical care.7–9 With the recent consensus on the definition of EOL,29 now is the time to actively progress funded research into EOL wound care; hence, the pressing need to develop and validate an EOL wound assessment tool to ensure the accurate and comparable collection of prevalence data and develop targeted clinical practice strategies, a stance confirmed by eminent international researchers, clinicians, and experts on the panel.
Strengths and LimitationsThe decision to implement a structured first round using the modified reactive Delphi panel25,26 enabled progression from the TU integrative review to providing experts with items that reflect current definitions and descriptions of EOL wounds. There may exist a risk of bias or limited responses given the structured form of the reactive method.25,26 However, providing for and encouraging comments on each item and round of online Delphi review allowed experts to share their expertise and views on the assessment tool.43
Predefining the level of consensus sought for item retainment and revision stages determined the number of rounds required. The methods of communication (via email and online survey) provided access at an international level and allowed experts to complete the survey at a convenient time, providing rapid individual response times. The consistency of responses between both rounds and the feedback provided from round 2 led to the decision to finalize the EOL wound assessment tool for future validation of the tool in the clinical setting.
Finally, the authors acknowledge that panel members were drawn from four developed countries and therefore may not represent experts globally. However, this reflects current evidence that suggests most published KTU and TU research is/has been conducted in the US.8,9
CONCLUSIONSUnavoidable EOL wounds can develop in some patients. These wounds differ from PI in terms of their appearance, development patterns, and subsequent management. The limited available rigorous TU research meant developing an EOL wound assessment tool required the input of experts in this field. The authors used a modified online reactive Delphi technique to gain consensus on the definition and characteristics of EOL wounds and establish the face and content validity of a new tool for use in adults at EOL. Using this tool in clinical settings may potentially increase the accurate identification of EOL wounds and confirm the extent of this clinical issue. Over the long term, implementation of the tool could also inform financial and legal concerns associated with these wounds and enable the deli
留言 (0)