
記住我






Schistosomiasis, a neglected water-borne tropical disease, is the second most common worldwide parasitic disease after malaria. As of 2021, the World Health Organization (WHO) reported a worldwide prevalence of 236 million people with an annual incidence of 140 million globally.1 Over 90% of the new cases occur in the socioeconomically challenged rural populace of sub-Saharan Africa.1 The 5 main species that affect the human populations are Schistosoma hematobium, Schistosoms mansoni, Schistosoma japonicum, Schistosoma intercalatum and Schistosoma mekongi.1,2 Successful transmission of species is highly dependent on the suitability of an environment to support the survival of its snail intermediate host.2 Although acute illness and atypical manifestations are most common in nonimmune travelers to endemic areas, chronic infections are frequently acquired by older children in susceptible communities.2 The parasite burden often peaks at about 15–20 years of age. The most common manifestation of S. hematobium is painless terminal hematuria. Possible complications are obstructive uropathy, growth failure, glomerulonephritis, squamous cell carcinoma and reproductive dysfunction.2 Rarely, there is embolization of the egg granuloma to produce a chronic lung disease, transverse myelitis and cerebral involvement.2
Despite the promotion of mass chemotherapy with praziquantel by WHO in endemic communities, a limited resource has hampered its successful implementation in most African countries.1,2 On the other hand, quality public health control measures have been successful in countries such as Japan, China, Brazil and Egypt.1,2 Warmer temperatures from climate change may expand the geographical areas that are supportive of schistosomiasis transmission.3 We described 3 adolescent immigrants from Africa living in Brooklyn with urinary schistosomiasis, all of whom had an initial misdiagnosis that led to a considerable delay of appropriate treatment.
CASE 1A 17-year-old male was referred to us for evaluation of painless terminal hematuria that was reported during hospitalization for relapsing schizophrenia. He also had intermittent episodes of dysuria and urinary frequency since 2015 (Table 1). He immigrated from North Sudan in East Africa to the United States in 2018. There is a history of recreational swimming at the Nile River while he was living in Sudan. His father and other family members had no physical exposure to the Nile River. He was evaluated by a pediatric urologist more than 3 years ago who failed to reach a substantive diagnosis. Urine analyses showed microscopic hematuria. He had an absolute eosinophil count of 890/mm3. An abdominal computerized tomography scan showed a diffuse mucosal thickening and dystrophic calcification of the bladder wall (Fig. 1). An enzyme-linked immunosorbent assay performed at a commercial laboratory was positive for S. mansoni IgG. However, urine microscopy showed multiple S. hematobium eggs and larvae. He was treated successfully with 2 weekly courses of Praziquantel.
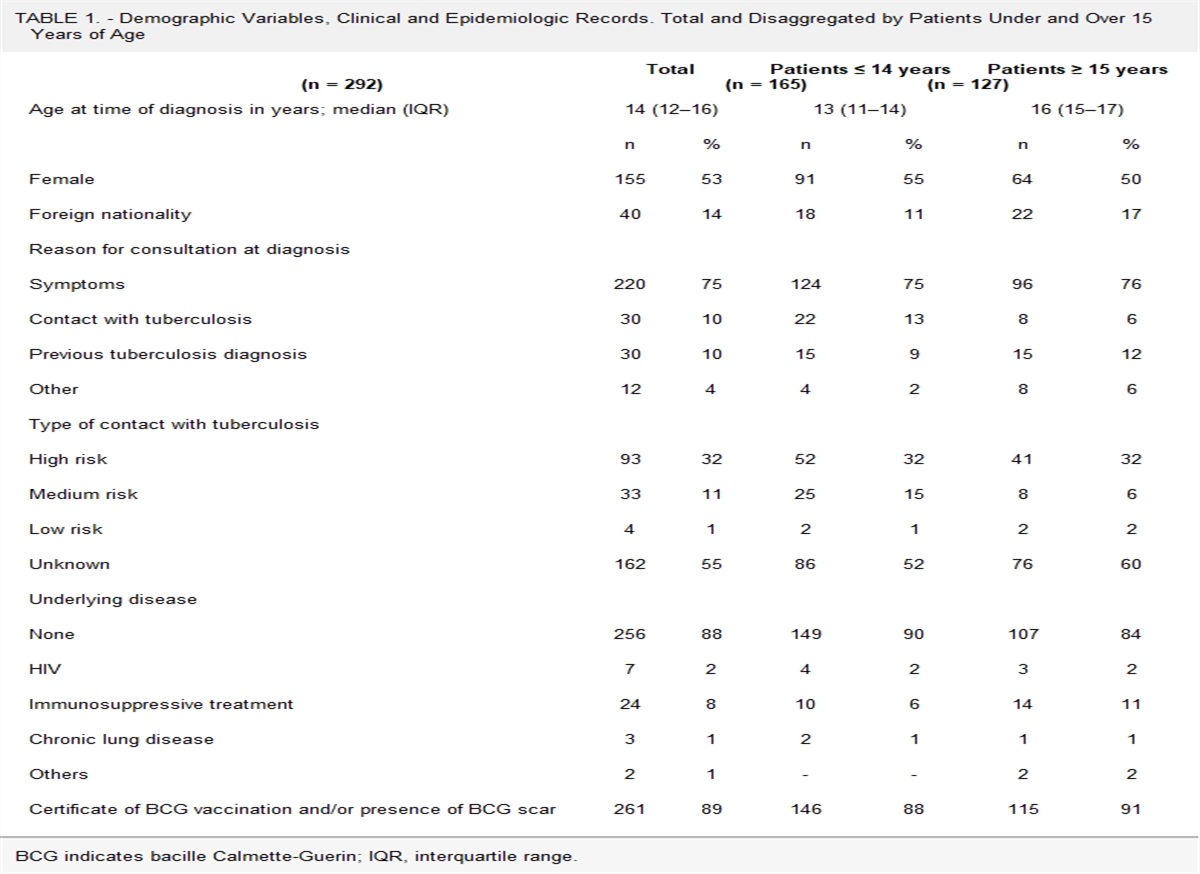
TABLE 1. - Case Summaries of Three Male Adolescent Foreign-born African Immigrants With Urinary Schistosomiasis From Brooklyn in New York City Case Age (y) Gender Height (m) (%) Weight (kg) (%) Duration of Symptoms Before Diagnosis (y) Country of Origin Serology Renal and Bladder Imaging 1 17 Male 1.7 (58%) 67.3 (46%) 6 Sudan, East Africa Schistosoma mansoni IgG CT scan: Bladder mucosal thickening and dystrophic calcification 2 16 Male 1.8 (68%) 46.3 (<1%) 7 Senegal, West Africa Schistosoma hematobium IgG US: Bladder wall thickening and blood clots 3 18 Male 1.7 (60%) 58.1 (28 %) 8 Senegal, West Africa Schistosoma hematobium IgG US: Echogenic kidneys and thickened bladder wall with polypoid blood clotsCT indicates computerized tomography.
 FIGURE 1.:
FIGURE 1.: An abdominal computerized tomography scan showing a dystrophic calcification of the bladder wall in a 17-year-old male adolescent with urinary schistosomiasis fromSchistosoma hematobium infection.
CASES 2 AND 3Two brothers, 16 and 18 years old, presented with a history of intermittent painless terminal hematuria for 7 and 8 years, respectively (Table 1). Both had a subnormal weight for height. They immigrated from Senegal in West Africa 2 years before the presentation. There had been reports of recreational swimming in community rivers and terminal hematuria among the youths in their village. The father recalled mass chemotherapy for school children was a common public interventional program. Unaware of the possible diagnosis of urinary schistosomiasis, an extensive workup of the hematuria was carried out by the primary care provider before referral. Urine microscopy revealed numerous red cells in both patients. Renal ultrasound showed increased echogenicity of both kidneys in the older brother. A bladder ultrasound showed thickened wall, multiple polypoid blood clots and features of urinary debris (Figure, Supplemental Digital Content 1, https://links.lww.com/INF/E916). The absolute eosinophil counts were 1390/mm3 and 940/mm3 in the older and younger brothers, respectively. Serologic studies for S. hematobium performed at a commercial laboratory were negative for both patients. The commercial laboratory uses the microsomal fraction of adult S. mansoni adult microsomal antigen (MAMA).4 However, repeat serologic testing performed by the Centers for Disease Control using immunoblot assay revealed a positive S. hematobium IgG. A fresh voided urinary examination showed multiple eggs and miracidia of S. hematobium. They were both treated with 2-weekly sequential doses of praziquantel leading to a parasitologic and clinical cure.
DISCUSSIONA strong clue to the diagnosis in the 3 patients was prolonged painless terminal hematuria in the setting of immigration from endemic zones in West and East Africa. Before referral, an extensive but costly laboratory workup for gross hematuria was performed. The patient from Sudan was initially referred to a pediatric urologist who did not consider a diagnosis of urinary schistosomiasis. A European study found that compared with African urologists and European urologists who had worked in Africa, there was a significant deficiency in the practical knowledge of tropical diseases among European-trained surgeons.5 After more than 6–8 years of symptoms in our patients, the diagnosis of urinary schistosomiasis was eventually considered by an experienced physician who migrated from Africa.
The diagnosis was confirmed in all 3 patients by the detection of S. hematobium eggs and motile miracidia in a fresh voided urine specimen performed by a foreign-trained tropical parasitologist. Confocal laser microscopy is a modern technique that enhances the detection of larvae in the urinary eggs as evidence of an active S. hematobium infection.6 Nevertheless, urine microscopy methodology remains the standard for diagnosis of schistosomiasis in endemic areas.2 It is simple, noninvasive and inexpensive. However, its accuracy depends on adequate training of laboratory staff which is frequently lacking in the least-affected countries. In addition, at the early phase of infection, due to a low number of parasites and egg production, the urinary examination is less sensitive than serologic analysis.2
The serologic assays performed at a commercial laboratory on 2 patients were probably false negative. The third patient had a positive result (S. mansoni antigen) which cross-reacted with S. hematobium. However, plasma samples sent to the CDC were positive for S. hematobium IgG in all 3 patients. Sensitivity and specificity vary widely among the tests for Schistosoma infection and are dependent on the type of antigen preparations used (crude, purified, egg, adult worm or cercaria).7 The methodology used by the commercial laboratories utilized S. mansoni MAMA. The CDC uses a combination of serologic tests for multiple Schistosoma species using purified antigens from adult worms.8 Specimens are first tested by a Falcon assay screening test-enzyme linked immunosorbent assay using S. mansoni MAMA. Because test sensitivity with the Falcon assay screening test-enzyme linked immunosorbent assay is reduced for species other than S. mansoni, immunoblots of the species which are appropriate to the patient’s travel history are also tested to improve the detection of S. hematobium infections (using Hematobium adult microsomal antigen). The presence of antibodies indicates that Schistosoma infection occurred at some point in the past and may not correlate with a current clinical status.8 Travelers from the United States to endemic regions who had exposure to fresh water via reactional swimming, rafting and kayaking in host countries are infected by the trematode. They are often asymptomatic or may have atypical clinical manifestations, and therefore serologic analysis is the mainstay of diagnosis.2 Furthermore, Schistosoma DNA can be detected in the filtered urine sediments using polymerase chain reaction even in the absence of egg excretion with 84% sensitivity and 97% specificity.9
There are peculiar radiologic features of S. hematobium that may help in arriving at a diagnosis while assessing structural alterations of the genitourinary system. Bladder wall imaging may reveal a circumferential calcification pattern with a pathognomonic feature termed “a fetal head in the pelvis.”10 The pelvic computerized tomography scan in case 1 revealed a dystrophic calcification of the mucosal wall of the bladder. The findings on bladder ultrasound of cases 2 and 3 are consistent with WHO criteria for diagnosis including an abnormal wall thickness, distorted morphology, and pseudo-polyp masses. However, there were no changes in the ureteral orifice or renal pelvis.11 Although a renal loss of corticomedullary differentiation may suggest a Schistosoma glomerulopathy in case 3, the absence of a significant proteinuria excluded such pathology.2
All 3 patients had onset of disease before 15 years of age, they were all males, all immigrated from Africa and all had a suboptimal nutritional status. These findings are consistent with a recent systematic review that revealed the most endemic zones for S. hematobium were East Africa and West Africa with a predominantly young male involvement.12 The patients presented here were immigrants to the United States and lived in Brooklyn. The delay in diagnosis was partly due to an immediate lack of health insurance and limited English language proficiency. Given the innocuous presentation in individuals affected by S. hematobium and the poor knowledge of the disease in the United States, most existing patients are likely to be undiagnosed. In a recent meta-analysis of 88 studies on immigrant populations from endemic countries in Europe and the United States, the pooled prevalence of schistosomiasis (14.6%; 95% confidence interval: 7.1–24.2) was highest among immigrants from sub-Saharan Africa.12 Although some of these events may represent an inactive disease, a pre- or postdeparture empirical treatment with praziquantel has been suggested as a useful preventive strategy. Furthermore, these findings underline the importance of routine community-wide surveillance of the at-risk population and targeted training of physicians with clinical practice in such populations for early recognition.
REFERENCES 1. World Health Organization. Global health estimates 2016: Deaths by cause, age, sex, by country and by region, 2000-2016. Geneva, Switzerland: World Health Organization; 2018. 2. Bamgbola OF. Urinary schistosomiasis. Pediatr Nephrol. 2014;29:2113–2120. 3. Yang GJ, Bergquist R. Potential impact of climate change on schistosomiasis: a global assessment attempt. Trop Med Infect Dis. 2018;3:117. 4. Maddison SE, Slemenda SB, Tsang VC, et al. Serodiagnosis of Schistosoma mansoni with microsomal adult worm antigen in an enzyme-linked immunosorbent assay using a standard curve developed with a reference serum pool. Am J Trop Med Hyg. 1985;34:484–494. 5. Mantica G, Van der Merwe A, Terrone C, et al. Awareness of European practitioners toward uncommon tropical diseases: are we prepared to deal with mass migration? results of an international survey. World J Urol. 2020;38:1773–1786. 6. Fritzsche C, Stachs O, Holtfreter MC, et al. Confocal laser scanning microscopy, a new in vivo diagnostic tool for schistosomiasis. PLoS One. 2012;7:e34869. 7. Hinz R, Schwarz NG, Hahn A, et al. Serological approaches for the diagnosis of schistosomiasis - a review. Mol Cell Probes. 2017;31:2–21. 8. Centers for Disease Control and Prevention. 2022. Available at: https://www.cdc.gov/parasites/schistosomiasis/health_professionals/index.html#dx Accessed April 6, 2022. 9. Ibironke OA, Phillips AE, Garba A, et al. Diagnosis of Schistosoma haematobium by detection of specific DNA fragments from filtered urine samples. Am J Trop Med Hyg. 2011;84:998–1001. 10. Shebel HM, Elsayes KM, Abou El Atta HM, et al. Genitourinary schistosomiasis: life cycle and radiologic-pathologic findings. Radiographics. 2012;32:1031–1046. 11. Onile OS, Awobode HO, Oladele VS, et al. Detection of urinary tract pathology in some Schistosoma haematobium infected Nigerian adults. J Trop Med. 2016;2016:5405207. 12. Asundi A, Beliavsky A, Liu XJ, et al. Prevalence of strongyloidiasis and schistosomiasis among migrants: a systematic review and meta-analysis. Lancet Glob Health. 2019;7:e236–e248.
留言 (0)