
記住我










Pharmaceutical technologies include methods, techniques, and instrumentation in the compounding of drugs and other preparations used in the diagnosis and treatment of patients. These drugs can be sterile or non-sterile. In the case of sterile drugs, the work environment is a cleanroom with a laminar flow hood or isolator, and aseptic techniques are required to maintain sterility throughout the process.
Healthcare simulation is a technique that creates a situation or environment to allow persons to experience a representation of a real healthcare event for the purpose of practise, learning, evaluation, testing, or to gain understanding of systems or human actions.1 In other words, simulation makes an experimental situation as close to reality as possible.
The efficacy of simulation methods depends on the trainer’s perspective of the three axes of simulation fidelity2: environmental fidelity, concerning the extent to which the simulator duplicates sensory information from the environment (a simulated cleanroom that looks like a real one); equipment fidelity, concerning the degree to which the simulator duplicates the appearance and feel of the real system (isolator or laminar flow hood identical to the one used daily); and psychological fidelity, concerning the degree to which the trainee perceives the simulation to be a believable surrogate for the real task.3
The French National Authority for Health lists three categories for simulation techniques in healthcare4: human simulation (standardised patients, role-playing), synthetic simulation (procedural simulators, patient simulators), and electronic simulation (3D environments, serious games, virtual reality, augmented reality). This classification is representative in medicine, and particularly in surgery or anaesthesia where simulation is regularly used, but is less appropriate for pharmaceutical courses and especially for hospital pharmaceutical technologies (HPT) where simulation is still in its infancy.
Several studies have shown the positive impact of using simulation in the training of pharmacy students and pharmacists to improve technical skills5–7 (medicines reconciliation, medical emergencies, order verification) and non-technical skills8–10 (communication, attitude, empathy). The above competencies mainly concern clinical pharmacists and their relationships with patients. It is hard to find simulation-based training dedicated to pharmacists working in pharmaceutical technologies, especially in hospital.
However, using simulation could enhance numerous pharmaceutical technology skills such as developing technical and functional expertise (training in routine or exceptional technical manipulations and implementing individual or team procedures such as hygiene or preparation of an isolator), building problem-solving and decision-making skills (in risk management—reproduction of adverse events, ability to cope with exceptional situations—of medication errors, broken vials, or extravasation and training in diagnostic and therapeutic clinical reasoning such as the analysis of prescriptions or preparation sheets), and promoting interpersonal, communication, and team-based skills (behaviour management of professional situations, teamwork, and communication using stress management or effective team communication).11 12 Considering these potentials, we decided to review the literature about the different uses of simulation in HPT. We believe that this literature review could help pharmacists in the conception and promotion of educational actions involving the use of simulation for HPT.
The present study’s objectives were: (1) to provide an overview of simulation’s current place in the field of HPT education; (2) to create a classification specific to HPT inspired by the HAS classification; and (3) to discuss how simulation in HPT could be better used in the future.
Material and methodsData sourcesThis systematic review was performed according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.13 The research strategy consisted of searching for relevant article titles and abstracts in the PubMed, Embase, and Web of Science databases. Keywords were chosen by consensus between the authors, with regards to our objectives. The words ‘pharmaceutical technology’ or ‘pharmaceutical technologies’ are rarely used in scientific articles which usually focus on a specific area of that field. That is the reason why the words ‘cytotoxic OR chemotherapy OR aseptic OR parenteral nutrition’ were selected for the pharmaceutical technologies axis. The word ‘education’ would have been too discriminating, therefore, it was not included among our keywords and only ‘AND simulation’ was used for the pedagogical method axis. An additional manual search was also conducted in the bibliographic reference lists of selected articles and in the journals and archives of specific congresses on pharmaceutical technologies.
Inclusion and exclusion criteriaInclusion criteria were: design or use of simulation tools for education in pharmaceutical technologies, in initial education (university) or continuing education (hospital), published articles in English or French, and availability of the whole article. Exclusion criteria were: mathematical, computer, molecular, robotic, or cost simulation models.
AnalysisTwo pharmacists (AG and RV), working independently, searched the literature on 21 July 2020 using the chosen keywords, and selected articles based on their titles. These articles were sorted using their abstracts, and duplicate entries were eliminated. An analysis file spreadsheet (Excel) was created to collect the relevant data from each article. After a reconciliation of the results (comparing Excel spreadsheets), any discrepant opinions about article selection were discussed with a third author (PB) in order to reach a consensus. A final synthetic table was created from the detailed analysis file: author; title; year of publication; journal; country; study objectives; type of education—initial or continuing; field—chemotherapy or aseptic techniques; number and types of participants—pharmacists or pharmacy technicians; study length; evaluations of study limitations, impact, and Kirkpatrick evaluation levels (Reaction, Learning, Behaviour, Results) which are commonly used for evaluating training.14
ResultsThe search strategy is presented in figure 1 and summaries of the included studies can be found in tables 1 and 2.
 Figure 1
Figure 1 Flow diagram of the review article selection strategy of the literature.
Table 1Summary of the articles about the use of simulations in hospital pharmaceutical technologies initial education
Table 2Summary of the articles about the use of simulations in hospital pharmaceutical technologies continuing education
Most of the simulation studies were carried out in France (54%; n=7), with the others occurring in Switzerland (15%; n=2) and the USA (31%; n=4). Continuing education for professionals was represented (77%; n=10) more than initial education for students (23%; n=3). The training topics were competencies in the preparation of chemotherapies (31%; n=4) or parenteral nutrition (8%; n=1) and aseptic techniques for handling chemotherapies or other products (61%; n=8). Simulation-based training (SBT) sessions were proposed in different settings, including real-life cleanrooms in daily use (42%; n=5), simulated cleanrooms (42%; n=5), and virtual cleanrooms (16.7%; n=2). Participation was mandatory (8.3%; n=1), voluntary (16.7%; n=2), or not mentioned (75%; n=9).
When participants were pharmacists and pharmacy technicians (62%; n=8), the number of participants ranged from nine to 20 people. Sometimes participants were gathered from several hospitals (15%; n=2), thus increasing the number of participants from 45 to 72 people. When students were involved (23%; n=3), this number ranged from 109 to 150.
DiscussionTo our knowledge, this is the first systematic literature review investigating the use of SBT in HPT. It highlights the limited number of published articles on this subject, since only 13 articles were reviewed, both in academic teaching and professional practice. Our research revealed that the use of SBT in HPT could be separated into three categories summarised in figure 2: the use of simulation as a playful tool, simulation using electronic tools, and simulation as a contamination verification tool.
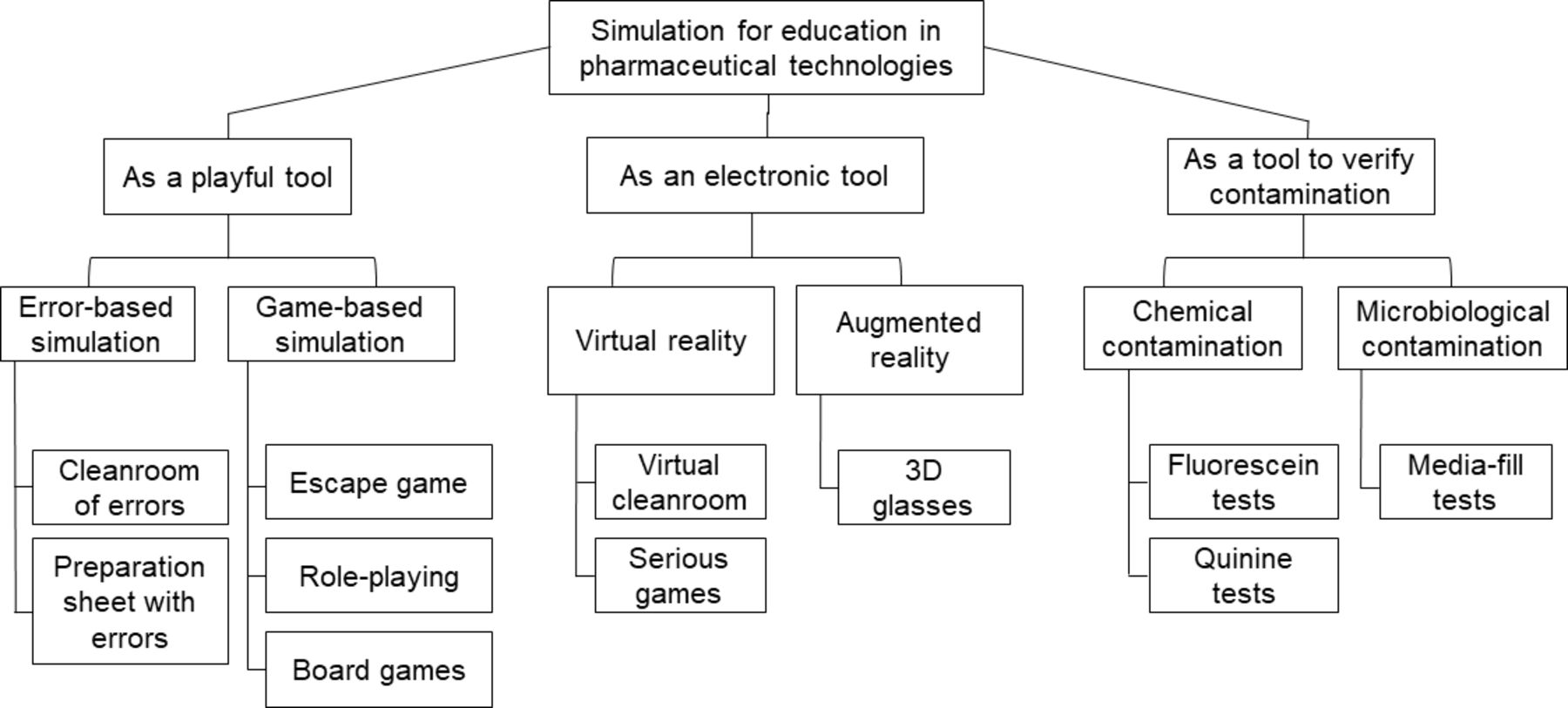 Figure 2
Figure 2 Ways of using simulation for education in hospital pharmaceutical technologies.
Simulation as a playful toolThe error-based simulationThe chamber of errors, also called the cleanroom of errors,15 16 the isolator of errors,17 18 or the controlled atmosphere area of errors,19 20 is an SBT approach where participants are asked to observe and report any of the several mistakes intentionally presented in a training room21 22 or on chemotherapy preparation sheets.23 24 The global objective of these studies is to assess pharmacy technicians’ knowledge of appropriate chemotherapy preparation practices. Some of these mistakes, which could lead to consequences for the patient (administering an expired medication or an overdose of vincristine, dispensing the wrong form of a drug), are major errors which participants are expected to spot.21
Integrating learning through errors into simulation approaches probably improves several competencies because trainees actively explore their environment and are explicitly encouraged to make and learn from mistakes, while competencies requiring improvement are pointed out. Error-based simulation is not only a game but also a cognitive model of safety improvement.
The game-based simulationUsing games—structured tasks forcing participants to interact according to a set of rules—captures the essence of real-life situations. Very few published, innovative, game-based simulations exist in the field of pharmaceutical technologies. One good example is the escape room for learning good manufacturing practices.25 In addition to testing learners’ theoretical and practical knowledge, the game aims to provide an instrument with which to study the processes involved in the actors’ interactions. However, the success of these studies differs according to the participants’ degree of involvement (better when they are deeply involved), the type of role being played (better when they play their own roles), and the response specificity (better when they feel free to behave as they want).26 In the HPT field, this role-playing method has been used to help students understand the role of an oncology pharmacist.27 Despite the discrepancy between role-playing and reality, students were able to apply (or identify gaps in) their knowledge and reinforce their critical thinking skills. Finally, several board-game-based simulations have been created to allow pharmacy technicians to check all the knowledge needed for the preparation of chemotherapies, such as a Trivial Pursuit-type game, a 37-card game, or a snakes-and-ladders board game.28–30 All of them have been well received thanks to their engaging visual, interactive, playful, and collaborative aspects.
Simulation using electronic toolsVirtual realityIn 2011 the first virtual cleanroom was created to cultivate students’ confidence in preparing intravenous medications appropriately while emphasising safe medication practices.31 At that time, it was challenging to find a suitable facility to host the sessions, access knowledgeable individuals capable of validating the virtual environment, and work within the limits of technology. Then a cleanroom simulator called LabQuest was developed to show that professionals trained using this system performed better than those trained using the traditional methods of video, quizzes, and PowerPoint presentations.32 This study is particularly interesting because it compared two homogeneous populations undergoing two different types of training.
As a mix between virtual reality and error-based simulation, the Association for the Digital and the Information for Pharmacy (ADIPH) created a serious game including 60 errors in its SimUPAC 360° virtual cleanroom.33
Augmented realityAugmented reality’s use in the field of educating employees about pharmacy technologies is still in its infancy, but results are encouraging. For the preparation of injectable drugs, 3D glasses can be used to reduce the number of medication errors related to a lack of information, by giving the step-by-step instructions to the pharmacy technician in an ergonomic and practical way.34 Test feedbacks are positive, but efficiency results are unavailable for the moment.
Simulation as a contamination verification toolChemical contaminationThe fluorescein test is a chemical contamination simulation process with two big advantages: it is safe, and contamination is easily visible under ultraviolet (UV) light. This method enables an assessment of the actions leading to contamination, as well as the frequency, location, and volumes of those contaminations. All these parameters are essential to knowing and controlling the exposure faced by pharmacy technicians, and this method, developed 25 years ago,35 36 is still used for validating them.37–39 Other studies replace fluorescein with quinine. Quinine solution is non-toxic and fluorescent under UV light, but it is also colourless, preventing pharmacy technicians from seeing contamination directly and modifying their actions during production. One of the studies reviewed showed no correlation between contamination rates and pharmacy technicians’ experience, but provided specific, individualised training when contamination quantities were over 10 µL.40 Others used the same method to insist on collective awareness of contamination risks and to work on improving manipulation gestures.41
These educational approaches are interesting because pharmacy technicians can visualise and account for chemical contamination in real-time. It seems more appropriate to use quinine in such evaluations because its solution resembles the drugs handled regularly in hospital pharmacies, being mostly colourless. These tests thus appear essential for validating new pharmacy technicians and requalifying them periodically in order to detect any problems during manipulation.
Microbiological contaminationThe media-fill test (MFT), sometimes known as ‘process simulation’, validates the pharmacy technician’s ability to maintain sterility throughout the manufacturing process. Microbiological growth medium is used in place of the drug solution to test whether aseptic procedures are adequate to prevent contamination during real-life drug production. As there is a significant microbiological risk during the preparation of parenteral nutrients or chemotherapies, the MFT is a very good means of evaluating pharmacy technicians. The result necessary for the validation of an MFT is zero microbiological growth. It was found that cases of microbiological growth were always linked to Enterococccus faecalis and directly correlated to poor aseptic technique,42 and that contamination during aseptic compounding was linked to human errors rather than environmental contamination.43 The MFT is used to validate how pharmacy technicians manipulate their equipment and is thus considered a pedagogical tool. If a pharmacy technician’s manipulations lead to microbiological growth, then they must be retrained in that particular manipulation gesture.
Perspectives for improvementEvaluation and educational contentStrengthening and improving the use of simulation in educating pharmacy technicians about HPT requires permanent evaluation and adjustment of the methods used. Only five of the 12 articles considered reported collecting information on trainee satisfaction (Kirkpatrick’s level 1). This ranged from a group discussion during a meeting21 to an individual survey composed of three questions using Likert scale responses.31 Such heterogeneity and subjectivity could be reduced by evaluating the relevance of the training content and the trainee’s involvement as the training progresses, as suggested in the New World Kirkpatrick Model.44 Although level 2 evaluation was more common, with seven out of 12 articles reporting a pre/post-assessment of knowledge, we believe that it is still not enough to justify scientifically the use of simulation over other training methods. Level 3 evaluation measures the impact of training on daily practice and is considered the most difficult part of training to evaluate. Indeed, none of the studies included in this review reported it.
Finally, level 4 aims to evaluate the impact of the training on patients, which none of our reviewed studies managed, or on the institution. LabQuest claims a training cost saving of at least €1500 per new employee45 but, in this review, only two studies mentioned its costs in terms of material, time, and human resources.31 46 If a positive return on investment represents the holy grail of SBT, the lack of studies including this aspect does not work in this educational approach’s favour. Some authors have proposed a framework for calculating the return on investment in the field of healthcare, and this might be adaptable to the field of HPT.47 However, it is more likely that the future evaluation of SBT is based on the return on expectations, a collaborative process where the sponsor’s expectations are identified and transformed into criteria of success, which are themselves transformed into assessment criteria.
Monitoring non-technical skillsA competency is the sum of knowledge, skill, and attitude. A study assessing 11 non-technical skills in a group of 15 pharmacy technicians showed a low score in leadership, commitment and work quality, which are all related to teamworking attitude.48 However, the importance of teamwork, communication, and collegiality—as non-technical skills—was neither assessed nor discussed in any of the studies reviewed. There is a need, in the future, to develop this field.
ConclusionThis study reviews all the simulation-based training used for education in hospital pharmaceutical technologies, both in academic teaching and professional practice. The classification proposed in this paper—playful tool, electronic tool, and verification tool—provides a state of the art but will certainly evolve in parallel with the evolution of evaluation methods and the recognition of non-technical skills as a fully-fledged subject of learning. Further studies are needed to confirm the usefulness of this innovative technique in training as efficiently as possible actual and future pharmacy professionals.
Data availability statementData are available upon reasonable request. Not applicable.
Ethics statementsPatient consent for publicationEthics approvalThis study does not involve human participants.
留言 (0)