
記住我




After participating in this CME activity, physicians should be better able to:
Identify the subtle radiographic findings in ankle fracture malreduction, shortening of lateral malleolus, and persistent talar translation. Evaluate patients with persistent pain after ankle fracture ORIF, and treat such patients with early joint degeneration with revision ORIF. Understand the role of corrective osteotomy for malunion in treating failed ankle fracture ORIF.Ankle fractures are common orthopedic injuries, occurring in between 71 and 187 per 100,000 people annually.1 Ankle fractures make up about 9% of all fractures and are the second most common fracture of the lower extremity.2,3 Almost half of the ankle fractures require surgical treatment to restore ankle stability and function, with open reduction and internal fixation being the typical route.4,5 A malunited ankle fracture, or malunion, is a fracture that has healed but results in a medial or lateral malleoli that has healed in a less than optimal position.6 Malunions can occur after operative fixation or conservative treatment and can occur in diaphyseal and articular fractures.7 Malunions can be seen in all different patterns of ankle fractures, namely: supination-external rotation, pronation-external rotation, pronation-abduction, and supination-adduction. An ankle fracture malunion that has even small amounts of malalignment will have substantially altered ankle biomechanics.8 Pathologic shortening, angulation, rotation, and/or irregularities of the joint surface can be present in malunions.7 All of these conditions can lead to abnormal weight transfer and can cause arthritic joint destruction, increasing the risk of post-traumatic arthritis. It has been previously established that the ankle joint has a limited ability to withstand asymmetry within the joint.9 In fact, lateral displacement of the talus by merely 1 mm produces a 42% reduction in the area of tibiotalar contact, thus increasing stress on the articular cartilage. Thus, operative treatment is imperative for any degree of shortening of the fibula.10 Restoring proper fibular length and rotation is crucial to restore stability and symmetry to the ankle joint.6 As such, the goal in treating malunion ankle fractures is to restore the ankle anatomic alignment and stable mortise, as well as to decrease the risk of post-traumatic arthritis.
Ankle fracture malunions can be surgically corrected with revision open reduction internal fixation (ORIF) with or without reconstructive osteotomy or by arthrodesis when significant joint degeneration has occurred. Revision ORIF is necessary when there is unrecognized syndesmotic injury, complete failure of fixation, or malposition of the medial malleolus during initial surgery.11 In addition, persistent shortening or external rotation of lateral malleolus can also result in suboptimal articular congruence in the ankle joint. Although the rate of complication after ankle fracture ORIF is low, malunited fractures should be treated with revision ORIF to prevent joint deterioration.6,12 The presence or absence of post-traumatic arthritis should be determined to know whether or not the ankle joint is salvageable.6 Joint-sparing osteotomies and reconstruction are contraindicated if severe, end-stage post-traumatic arthritis is present. In most cases, though, the joint remains salvageable even if some degree of arthritis exists. Unsalvageable ankle deformity with severe arthritis is best treated with total ankle arthroplasty or arthrodesis.
There is limited literature on patient-reported outcomes, radiographic outcomes, and postoperative complications after revision open reduction and internal fixation or arthrodesis for ankle fracture malunion. Previous studies have indicated that even when moderate ankle arthritis is present, restoring a malunion ankle fracture can improve pain, restore function, and preserve the longevity of the joint.6 However, revision ankle surgery may result in nontrivial complications such as deep infection, hardware failure, or persistence of pain.8 The objective of this study was to determine clinical and functional outcomes of revision ORIF for ankle fracture malunion through patient-reported outcomes and radiographic analysis. Determining these outcomes is essential to contribute to the currently limited information available about the efficacy and consequences of revision ORIF for ankle fracture malunion, and further elucidate whether revision ORIF is an effective technique to restore anatomic alignment and ankle function in select patients with malunion.
METHODSAfter approval by the Institutional Review Board, the Enterprise Data Warehouse was queried for patients with malunion or nonunion ankle fracture who underwent a revision ankle ORIF procedure by fellowship trained Foot and Ankle surgeon in a tertiary referral center between January 1, 2017, and October 19, 2020. Seven patients were identified, with all having malunion ankle fractures and undergoing revision ankle surgery with the goal of aligning the joints (Figs. 1–3). Each patient underwent a preoperative CT scan to further characterize the malunion and deformity and also aid with surgical planning (Fig. 4). A tibia, lateral, or medial malleolus osteotomy was conducted in all patients to correct the deformity (Fig. 5). Each of the 7 patients’ medical charts were reviewed to identify patients’ demographic factors, medical comorbidities, complications after surgery, and radiographic images. Patient variables obtained included age, sex, body mass index, race, ethnicity, medical comorbidities, operative reports, progress notes, subsequent procedures/additional operative reports, and baseline PROMIS survey responses. Four of the participants had baseline PROMIS scores reported in their electronic medical record before the procedure. Three of the participants were contacted postoperatively to obtain baseline PROMIS scores. All of the participants were contacted by phone from January to April 2021 to obtain postoperative PROMIS survey responses. To reduce the risk of bias, the patients were asked survey questions and provided with standard response options without coaching that might influence a response in a specific direction. The patients were given electronic tablets in clinic or given a link via email to complete the questionnaire. The obtained data were analyzed to assess patient-reported outcomes, postoperative complications, and radiographic outcomes.
 FIGURE 1:
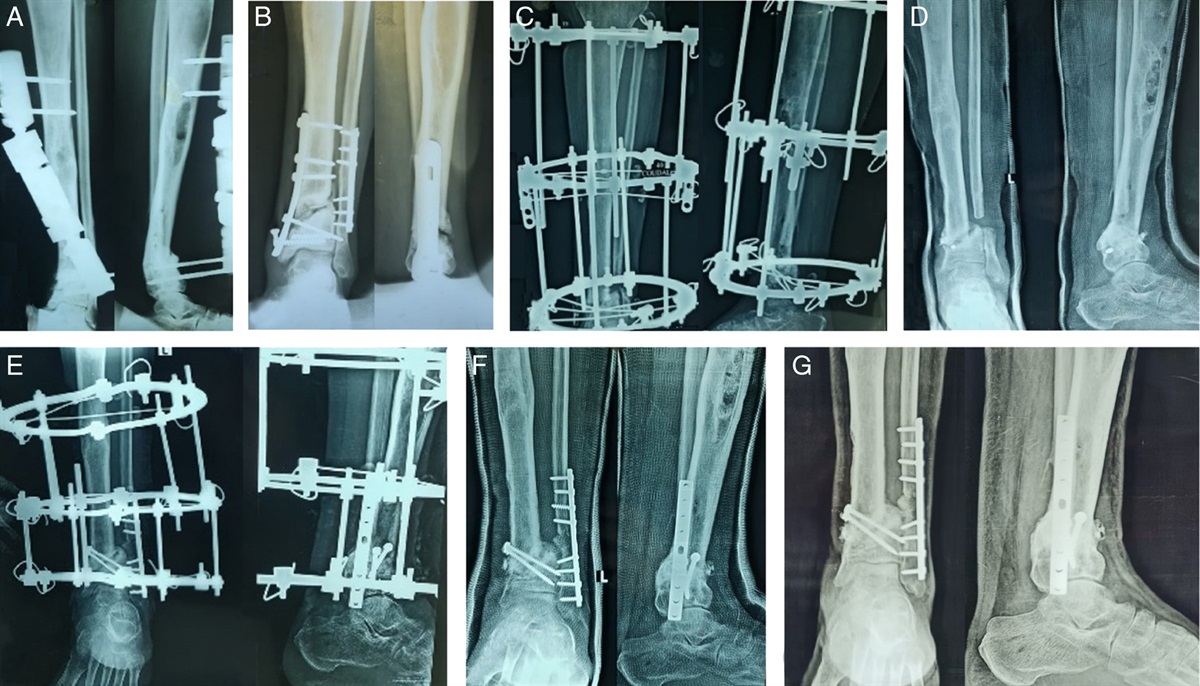
FIGURE 1: A 57-year-old female with previous right ankle fracture, pilon variant. She presented 3.5 months status post-ORIF and has been non–weight-bearing. A–C. Injury films reveal medial malleolus and anterolateral (Chaput) tibia fracture fragments.
 FIGURE 2:
FIGURE 2: A–C, At 2 weeks post op, patient remains non weight bearing in a splint.
 FIGURE 3:
FIGURE 3: At 10 weeks anterior posterior view (A), lateral view (B), and oblique view (C). Interval healing of the medial malleolus is seen. However, there is also a displaced malunited Chaput fragment.
 FIGURE 4:
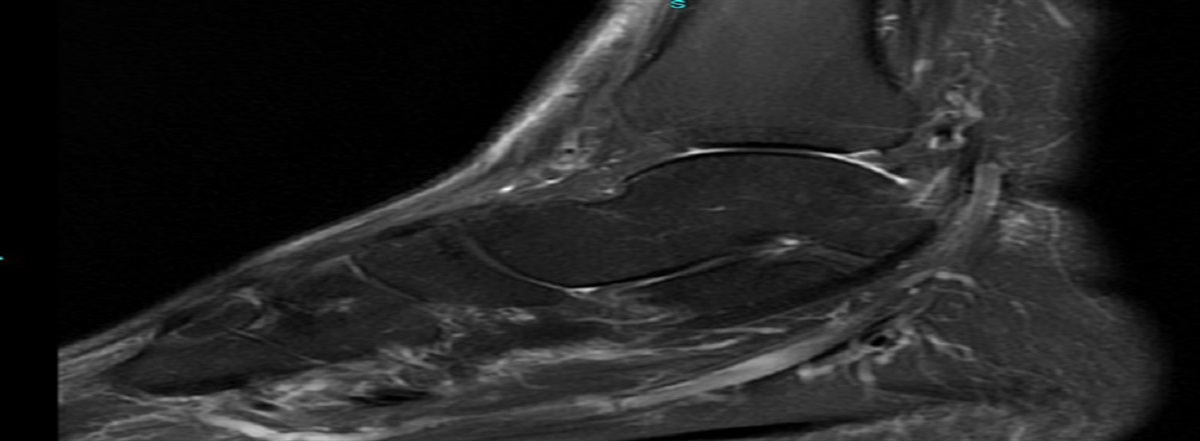
FIGURE 4: A-C, Computed tomography scan at 10 weeks demonstrates shortening of the Chaput fragment with varus angulation of the tibial plafond with incongruous tibiotalar joint and anterior talus translation.
 FIGURE 5:
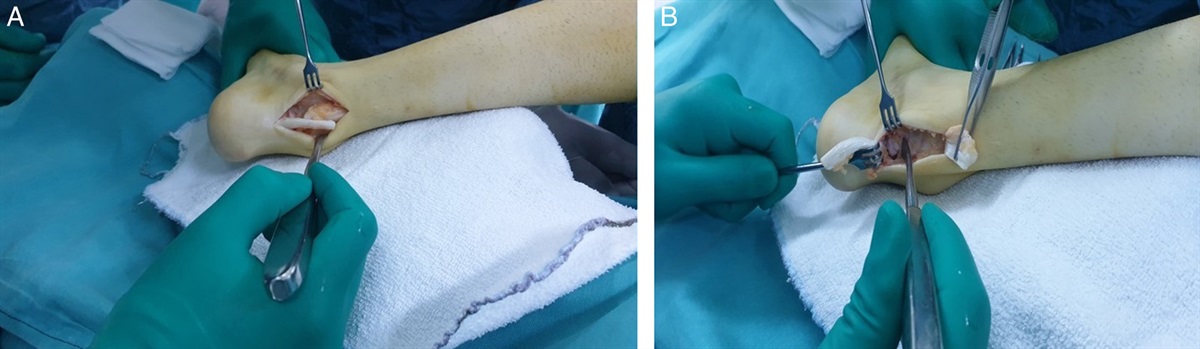
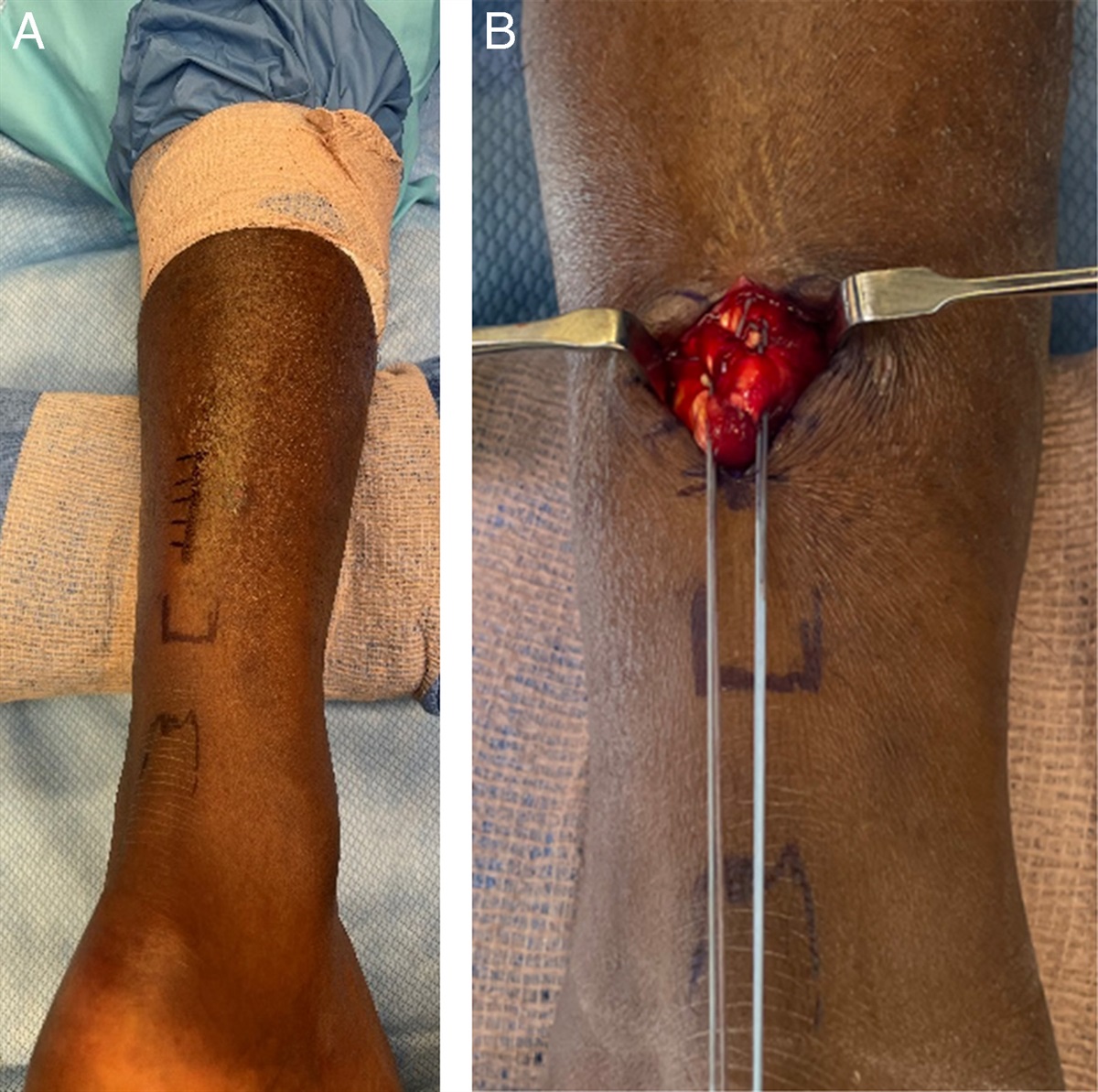
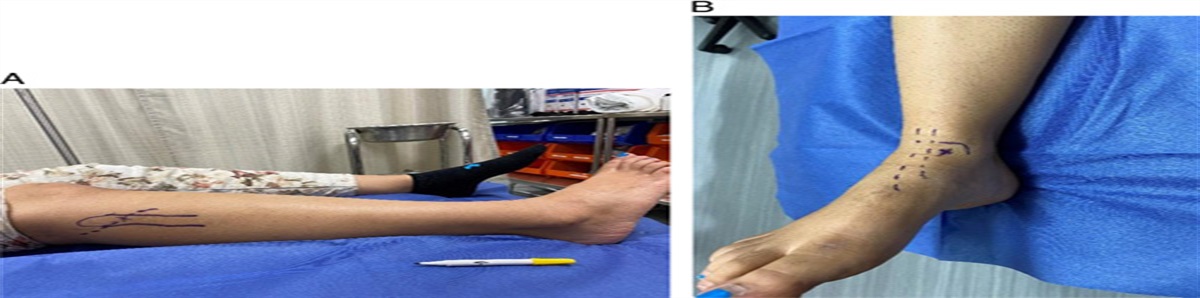
FIGURE 5: A, Patient underwent revision ORIF of the right ankle. Anterior incision just lateral to the tibialis anterior tendon was utilized. After arthrotomy, the malunion was exposed. Using an osteotome and an oscillating saw, this anterior fragment was taken down and made mobile under fluoroscopic guidance. B, Anatomic reduction was achieved by correction of the shortening and varus malalignment. C, Provisional fixation was obtained with a K wire and confirmed with fluoroscopy.
RESULTSA total of 7 patients who underwent revision ORIF surgery for an ankle fracture malunion between January 2017 and October 2020 were included in this study. Table 1 shows the demographic characteristics of the sample studied. The average age was 46.3±12.2 years old. Total 85.7% of the patients were female, 14.3% were male. The average body mass index was 28.6±6.1 kg/m2. The average amount of time between the patients’ revision ORIF procedure and collection of postoperative PROMIS scores was 19.3±5.9 months. Surgical technique varied between patients but retained the same goal of aligning the ankle joint in malunion fractures.
TABLE 1 - Demographic Characteristics n=7 Age (mean, SD) 46.3 (12.2) Sex (n) Male 1 Female 6 BMI (mean, SD) 28.6 (6.1) Race (n)* White 6 Ethnicity (n)† Not Hispanic or Latino 5 Months between revision ORIF and postoperative PROMIS (mean, SD) 19.3 (5.9)Age is presented as years with mean and SD. BMI is presented as kg/m2 with mean and SD. Categorical variables (sex, race, and ethnicity) are presented as frequency count. Months between revision ORIF and postoperative PROMIS survey is presented as months with median and SD.
*n=6.
†n=5 because of unavailable information for some participants.
BMI, body mass index; ORIF, open reduction internal fixation; PROMIS, Patient-reported Outcomes Measurement Information System.
Table 2 shows baseline and postrevision ORIF physical function PROMIS scores. For each of the participants, there was an increase in physical function PROMIS score seen after the revision ORIF procedure compared with the baseline, indicating an improvement in physical function in the malunited ankle postprocedure. The average preoperative physical function PROMIS score was 30.7; the average postoperative physical function PROMIS score was 48.9.
TABLE 2 - Baseline and Post-ORIF Physical Function PROMIS Scores (PF) Baseline PF PROMIS Postoperative PF PROMIS Time between baseline and postoperative (months) Participant 1 32.2 44.5 18.9 Participant 2 40.0 44.0 32.0 Participant 3 30.7 54.5 10.9 Participant 4 32.2 51.2 17.6 Participant 5 24.5 52.2 19.8 Participant 6 31.2 42.3 16.5 Participant 7 24.4 53.7 19.3 Average 30.7 48.9 —Baseline and post-ORIF physical function PROMIS scores are reported with a mean of 50.
Time between revision ORIF and postoperative PROMIS score is reported in months.
PF, physical functional; ORIF, open reduction internal fixation; PROMIS, Patient-reported Outcomes Measurement Information System.
Table 3 shows each of the 7 participants’ baseline and postrevision ORIF pain interference PROMIS scores. For each of the participants, there was a decrease in PROMIS pain interference score seen after the revision ORIF procedure compared with the baseline, indicating a decrease in pain after revision ORIF of the malunited ankle. The average preoperative pain interference PROMIS score was 64.8; the average postoperative pain interference PROMIS score was 55.6.
TABLE 3 - Baseline and Post-ORIF Pain Interference (PI) PROMIS Scores Baseline PI PROMIS Postoperative PI PROMIS Time between revision ORIF and postoperative (months) Participant 1 68.7 57.3 18.9 Participant 2 54.0 51.0 32.0 Participant 3 68.1 61.5 10.9 Participant 4 59.1 48.7 17.6 Participant 5 70.5 51.3 19.8 Participant 6 73.7 63.7 16.5 Participant 7 59.6 56.2 19.3 Average 64.8 55.7 —Baseline and post-ORIF pain interference PROMIS scores are reported with a mean of 50. Time between revision ORIF procedure and postoperative PROMIS score is reported in months.
PI, pain interference; ORIF, open reduction internal fixation; PROMIS, Patient-reported Outcomes Measurement Information System.
Of the 7 participants who underwent revision ORIF procedure for ankle fracture malunion, a majority of the participants did not experience any complications at least 1 year postprocedure. One participant (participant 1) subsequently underwent hardware removal for persistent pain. The same patient developed overlying cellulitis that was successfully treated with a 2-week course of oral clindamycin. Besides this participant, the other 6 individuals who underwent revision ORIF for ankle malunion did not experience any postoperative complications including infection, reoperation, or hardware removal.
DISCUSSIONIn this study, we found that a majority of participants—6 out of the 7 total participants—who underwent revision ORIF for ankle malunion did not experience postoperative complications (Fig. 6). In addition, we found that each patient exhibited an increase in physical function PROMIS score and decrease in pain interference PROMIS score after revision of ankle fracture malunion. These findings indicate that for each of these participants, the revision ORIF procedure for their ankle fracture malunion was beneficial in terms of restoring ankle function and decreasing pain, both of which contribute to their overall well-being and return to preinjury activities (Fig. 7). Despite aiming to restore functionality, the procedure holds certain risks. The risk of progressive arthritis still exists given the history of fracture, malunion, and surgery. Furthermore, risk for subsequent surgery is higher than if the ankle joint were fused.
 FIGURE 6:
FIGURE 6: Bone graft was placed in the small area anterolaterally, followed by plate fixation below. Final anterior posterior view (A), final oblique (B), and final lateral view (C).
 FIGURE 7:
FIGURE 7: Six months status post revision ORIF. Well-maintained ankle mortis without fixation loss or hardware failure. Patient back to baseline activities with minimal residual swelling around the ankle. Anterior posterior view (A), oblique view (B), and lateral view (C).
Literature on the outcomes of using revision ORIF to restore ankle function within an ankle fracture malunion is lacking. Our study is among the few to report on the outcomes of this strategy. A study by Bigsby et al8 that investigated 9 patients who underwent revision open reduction and internal fixation for malreduced ankles from January 2007 to January 2010 found that 3 (33%) developed a deep infection due to methicillin-resistant Staphylococcus aureus. In addition, 1 patient (11%) developed chronic regional pain syndrome, 1 patient (11%) experienced failure of plate fixation, and 1 patient (11%) experienced persistent pain requiring arthroscopy and debridement. The overall incidence of complications was 66.67% in this group, thus indicating that high incidence of complications should be taken into consideration before the operation. Our investigation only found complications in 1 participant (14.3%) including hardware removal and suspicion for cellulitis treated with antibiotics. Our study, along with the study from 2014, both indicate that postoperative complications such as infection are possible postrevision ORIF but are not common. As such, these possible complications should be taken into consideration preoperation for decision-making in a patient with a malunited ankle fracture.
Another study by Reidsma et al10 investigating 57 ankle fracture malunion that were treated with reconstructive osteotomy between 1975 and 1997 found that 85% of the patients had good or excellent results, with beneficial results lasting up to 27 years after the procedure. They also found that prolonged time to reconstruction is associated negatively with outcome. Reidsma et al10 found that 42 patients (88%) presented with good to excellent outcomes on radiographic analysis. This led them to recommend secondary reconstructive surgery over total ankle arthroplasty and arthrodesis in malunited ankle fractures. Similarly, we found that patients’ malunited ankles improved in both physical function and pain levels postrevision ORIF, based on the reported PROMIS scores. Our study provides further evidence that revision ORIF is an effective method in helping restore ankle function and anatomic alignment in patients with malunited ankle fractures.
Our study is unique, but is not without limitations. One limitation is that the sample size of the study is small with 7 participants. In addition, baseline physical function and pain interference PROMIS scores were obtained postoperatively for 3 out of the 7 participants, as these were not collected beforehand. This introduces the possibility of recall bias, as these participants were asked at a time point after the procedure to remember their preoperative ankle physical function and pain level, suggesting that some of the preoperative PROMIS scores may not accurately reflect preoperative characteristics. Future studies should consist of a larger sample size, collect baseline PROMIS scores for all participants at the same relative time point preoperatively, extend the timeline to collect PROMIS scores beyond 2 years postoperation and also investigate outcomes of individuals who undergo arthrodesis for malunited ankle fracture to compare to outcomes of individuals who undergo revision ORIF. Future studies aiming to study that a larger sample size may consider a multicenter study methodology. Despite these limitations, the results of this study contribute toward a better understanding of the outcomes and efficacy of revision open reduction and internal fixation in restoring ankle function in patients with malreduced ankle fractures.
CONCLUSIONSAnkle fractures commonly require surgical repair, though suboptimal repair and malunion may occur after both surgical and conservative management. This can be addressed through revision open reduction internal fixation or ankle arthrodesis depending on the extent of joint degeneration. Treatment of ankle fractures with suboptimal reduction with or without internal fixation or subsequent loss of adequate fixation can lead to traumatic degenerative arthritis of the joint. As such, it is paramount to consider revision open reduction internal fixation in ankle fracture malunion with maintained articular surface integrity. In this case series, our patients were able to improve physical function, decrease pain, and preserve their ankle motion after a revision ORIF procedure while experiencing low rates of complications. Reported complications in the literature include deep infection, persistent pain, and failure of plate fixation. Given the paucity of literature on revision surgery after ankle malunion, there is a need for further studies on efficacy and outcomes of the procedure using larger study populations.
CME QUESTIONS Which of the following is the most appropriate method of treating lateral malleolar fracture that has healed with shortening and valgus malunion with well-preserved joint space: Ankle arthrodesis Total ankle arthroplasty Physical therapy Fibular osteotomy, length restoration, and plate fixation A 33- year old man presents 3 months status post right ankle bimalleolar ankle fracture ORIF with persistent pain and decreased function. Initial assessment should include all of the following except: Weight-bearing x-rays History and physical exam Arizona brace Rule out presence of infection Which of the following postoperative radiographic finding may not accelerate post-traumatic arthritis of the ankle joint: Talar translation and tilt Fibular shortening Articular stepoff Medial clear space <5 mm Evaluation of weight-bearing ankle alignment, fracture healing, and articular congruence can be achieved more accurately using: Physical exam alone Weight-bearing CT scan Magnetic resonance imaging Gait analysis At a 10-week postoperative visit, you noticed displaced fracture of the anterior tibial plafond with slight anterior talar translation. Lateral and medial malleoli seem to be well healed. What is the next best step: Place a walking cast Plan for fragment excision CT scan to assess the extent of fracture fragment Transition to weight-bearing as tolerated in regular shoe REFERENCES
1. Daly PJ, Fitzgerald RH Jr, Melton LJ, et al. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand. 1987;58:539–544.
2. Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37:691–697.
3. Court-Brown CM, Aitken S, Hamilton TW, et al. Nonoperative fracture treatment in the modern era. J Trauma. 2010;69:699–707.
4. Jensen SL, Andresen BK, Mencke S, et al. Epidemiology of ankle fractures. A prospective population-based study of 212 cases in Aalborg, Denmark. Acta Orthop Scand. 1998;69:48–50.
5. Leyes M, Torres R, Guillen P. Complications of open reduction and internal fixation of ankle fractures. Foot Ankle Clin. 2003;8:131–147.
6. Clare MP, Berkowitz MJ. Revision open reduction and internal fixation of ankle and syndesmosis malunions. Instr Course Lect. 2019;68:265–274.
7. Weber D, Borisch N, Weber M. Treatment of malunion in ankle fractures. Eur J Trauma Emerg Surg. 2010;36:521–524.
8. Bigsby E, Cowie S, Middleton RG, et al. Complications after revision surgery of malreduced ankle fractures. J Foot Ankle Surg. 2014;53:426–428.
9. Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976;58:356–357.
10. Reidsma II, Nolte PA, Marti RK, et al. Treatment of malunited fractures of the ankle: a long-term follow-up of reconstructive surgery. J Bone Joint Surg Br. 2010;92:66–70.
11. Walsh AS, Sinclair V, Watmough P, et al. Ankle fractures: getting it right first time. Foot (Edinb). 2018;34:48–52.
12. SooHoo NF, Krenek L, Eagan MJ, et al. Complication rates following open reduction and internal fixation of ankle fractures. J Bone Joint Surg Am. 2009;91:1042–1049.
REFERENCES
1. Daly PJ, Fitzgerald RH Jr, Melton LJ, et al. Epidemiology of ankle fractures in Rochester, Minnesota. Acta Orthop Scand. 1987;58:539–544.
2. Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37:691–697.
3. Court-Brown CM, Aitken S, Hamilton TW, et al. Nonoperative fracture treatment in the modern era. J Trauma. 2010;69:699–707.
4. Jensen SL, Andresen BK, Mencke S, et al. Epidemiology of ankle fractures. A prospective population-based study of 212 cases in Aalborg, Denmark. Acta Orthop Scand. 1998;69:48–50.
5. Leyes M, Torres R, Guillen P. Complications of open reduction and internal fixation of ankle fractures. Foot Ankle Clin. 2003;8:131–147.
6. Clare MP, Berkowitz MJ. Revision open reduction and internal fixation of ankle and syndesmosis malunions. Instr Course Lect. 2019;68:265–274.
7. Weber D, Borisch N, Weber M. Treatment of malunion in ankle fractures. Eur J Trauma Emerg Surg. 2010;36:521–524.
8. Bigsby E, Cowie S, Middleton RG, et al. Complications after revision surgery of malreduced ankle fractures. J Foot Ankle Surg. 2014;53:426–428.
9. Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg Am. 1976;58:356–357.
10. Reidsma II, Nolte PA, Marti RK, et al. Treatment of malunited fractures of the ankle: a long-term follow-up of reconstructive surgery. J Bone Joint Surg Br. 2010;92:66–70.
11. Walsh AS, Sinclair V, Watmough P, et al. Ankle fractures: getting it right first time. Foot (Edinb). 2018;34:48–52.
12. SooHoo NF, Krenek L, Eagan MJ, et al. Complication rates following open reduction and internal fixation of ankle fractures. J Bone Joint Surg Am. 2009;91:1042–1049.
留言 (0)