
記住我




The participants were classified into the following three categories based on SE refractive error (defined as spherical power plus one-half of the cylindrical power): emmetropes (+ 0.5 to − 0.25 D, n = 23), mild and moderate myopes (–0.5 to − 6.00 D, n = 32), and high myopes ( ≤ − 6.25 D, n = 38). This was to investigate the relationship between the increasing degree of myopia and AST. As shown in Table 1, these groups did not differ significantly in age or sex (Table 1).
Table 1 Basic information of the three groupsThis study was approved by the Medical Ethics Committee of Nanchang University, Jiangxi, China and adhered to the principles of the Declaration of Helsinki. The nature of the study was explained to all participants, and appropriate consent, both written and verbal, was obtained.
The inclusion criteria were as follows: 1) AL ≥ 22.5 mm or SE ≤ + 0.5 D. (2) Aged between 20 and 50 years. (3) If both eyes of a participant met all the inclusion and exclusion criteria, only the right eye was chosen for the study. None of the participants wore rigid contact lenses, and those who wore soft contact lenses abstained from wearing them for 1 week before their participation in the study.
The exclusion criteria were as follows: (1) Presence of ophthalmopathy except for myopia (e.g., high myopia choroidal neovascularization, pterygium, retinal vein occlusion, glaucoma, uveitis, history of ocular trauma, rheumatoid arthritis and other auto-inflammatory); (2) Using systemic or topical medication; (3) Wearing or discontinuation of keratoplasty lenses within 1 week; (4) Anisometropia of ≥ 1.5 D and Km < 46.0 D; (5) History of ocular surgery (e.g., retinal laser photocoagulation, vitreous injection, and cataract surgery); (6) Presence of ocular hypertension; (7) Non-cooperating patients or those who could not complete the ophthalmic examination; (8) Presence of chronic diseases, such as systemic hypertension and diabetes mellitus; (9) Poor-quality AS-OCT scan results.
All the participants underwent an initial comprehensive eye examination; this included slit-lamp biomicroscopy and a dilated fundus examination, a refractive error assessment (KR-8900 autorefractor, Topcon, Japan), measurements of best-corrected visual acuity and intraocular pressure (Full Auto Tonometer TX-F, Topcon, Japan). Scleral thickness was assessed (CIRRUS HD-OCT5000, Carl Zeiss Meditec, U.S.A.), AL and mean meridian keratometry were measured (IOL Master 5.5, Carl Zeiss Meditec AG, Germany), central refraction was determined (ARK-510 autorefractor, Nidek, Japan), and wide-field fundus images were captured (Scanning Laser Ophthalmoscope, Daytona P200T, Optos, U.K.).
An average of five consecutive measurements were obtained for the AL, an average of three consecutive measurements were obtained for the Km, and an average of three measurements were obtained for the central refraction. All measurements were obtained by the same examiner. Subjective refraction was performed on all participants by a trained optometrist. The SE was calculated as the sphere plus half a cylinder. An Scanning Laser Ophthalmoscope test was used to further exclude fundus diseases other than myopia.
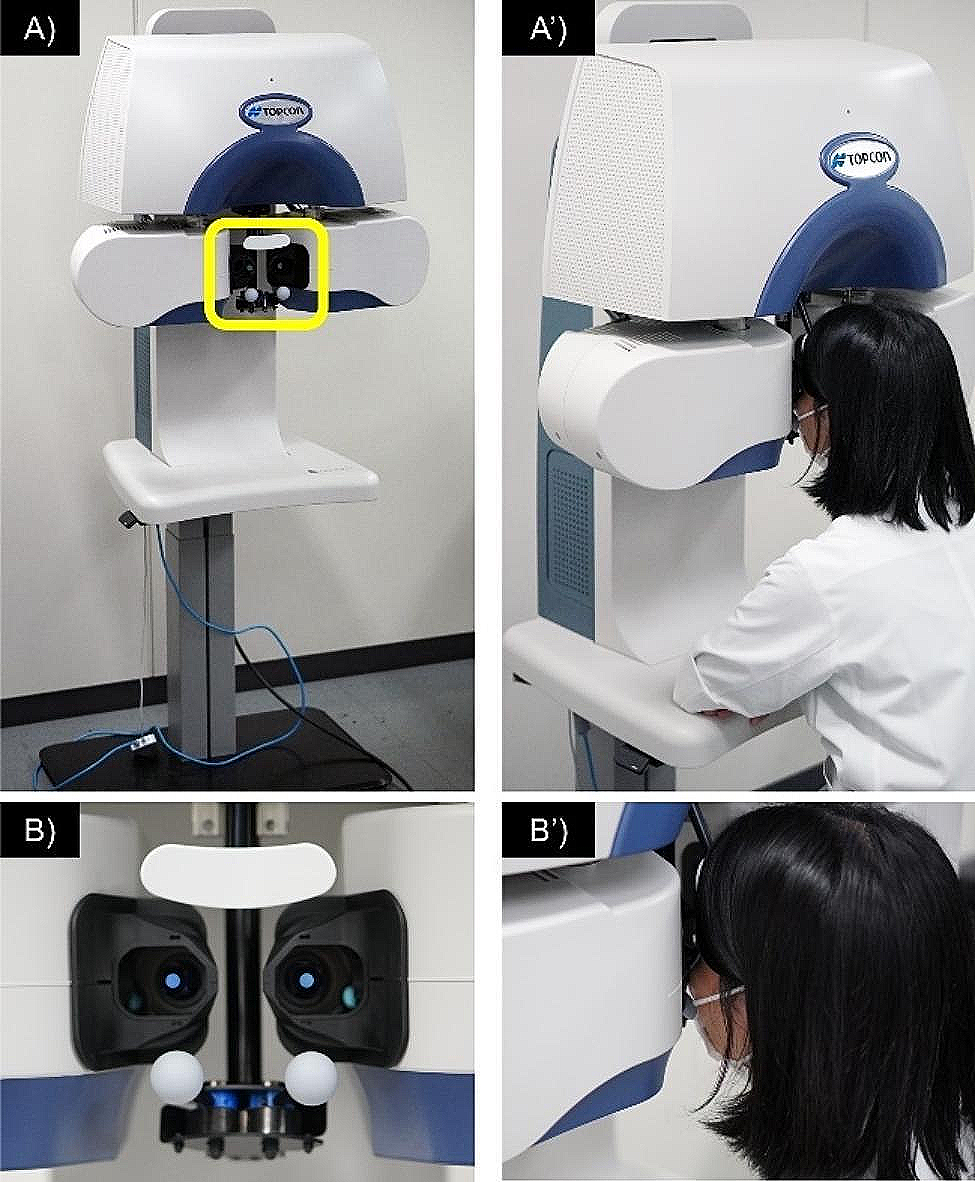
Measurement of anterior scleral thicknessAn anterior segment module was attached in front of the objective lens of the HD-OCT instrument. A 9-mm single-line scan protocol (length: 9 mm, depth: 2.6 mm) was used to acquire raw B-scan OCT images along each of the four meridians (superior, inferior, temporal, and nasal) while the participant fixated an appropriately located target; an image of the sclera was acquired within this target. During imaging, the scan line was positioned such that it passed above the scleral reflex in each gaze position to ensure that the AST results were obtained consistently in the same region of interest in all the participants (Fig. 1).
Fig. 1
A Single-line scan passing through the temporal scleral reflex. B Cropped raw B-scan image of the anterior sclera (dimension of the exported image: length: 9 mm, depth: 2.6 mm). The yellow arrowheads indicate the anterior scleral boundary and posterior scleral boundary, and the red arrowhead indicates the location of the scleral spur (reference point). Segmented optical coherence tomography image obtained after analysis with custom-designed software. The solid blue lines denote the 1-mm intervals at which the scleral thickness was measured
Scleral thickness was determined by manual measurement using caliper software included in the instrument. Only the images of the right eyes were used to analyze AST. We acquired raw B-scan OCT images along each of the four meridians (superior, inferior, temporal, and nasal) and marked the scleral spur as a reference point to enable the computation of the AST at intervals of 1 mm. All the images were analyzed by manual measurement to determine the AST, which was estimated from the scleral spur to a distance of 6 mm (n = 93) along the four meridians.
On the B-scan images of the anterior sclera, the outer boundary was identified as a thin hyporeflective region on the anterior part of the sclera, which is an actual presentation of episcleral blood vessels that separates the episclera and conjunctiva from the scleral tissue [11]. The inner boundary is a demarcated line between the hyper-reflective scleral tissue and the hyporeflective ciliary body tissue. Scleral thickness was measured as the distance between the outer and inner boundaries at the point of interest (Fig. 1).
The examiner marked the scleral spur (a slightly depressed region in the limbal area, facing the anterior chamber) as a reference point to enable the computation of scleral thickness at 1-mm intervals, extending peripherally from the scleral spur. Specifically, the thickness values were obtained along the direction normal to the tangents passing through the interval points located on the outer boundary for enhanced accuracy [10].The AST values were obtained up to 6 mm away from the scleral spur.
Data analysis and statisticsThis study used IBM SPSS 25.0.0 (SPSS, Inc., Chicago, IL, U.S.A.) software for all the statistical tests, and the inbuilt features of GraphPad Prism 8.0 (GraphPad Software, San Diego, United States) were used for plotting the graphs. Since the AST data were not found to depart significantly from a normal distribution (Shapiro–Wilk test: all P > 0.1 for the scleral thickness at all locations), parametric statistics were used throughout. Qualitative data were expressed as their frequency distributions. To examine the scleral thickness data in this population, a repeated-measures analysis of variance was used, with the measurement meridian (i.e., superior, inferior, nasal, and temporal) and measurement location respective to the scleral spur (i.e., 0, 1, 2, 3, 4, 5, or 6 mm). and refractive group (emmetropes, mild–moderate myopes, and high myopes), Bonferroni-corrected pairwise comparisons were performed for any significant main effects and interactions, including the continuous variables of age and SE refractive error as covariates. Additionally, we used a multiple linear regression analysis to examine age, AL, and scleral thickness measurements (i.e., the average thickness across all locations and meridians). A Student’s t-test was used to test differences in ocular biometry between male and female. The reliability of the AST measurements was assessed by estimating intraclass correlation coefficients (ICCs). A value of P < 0.05 was considered statistically significant.
留言 (0)