It was a retrospective comparative clinical study conducted on the patients with confirmed diagnosis of advanced keratoconus. We reviewed medical charts of 98 patients who underwent DALK (big bubble and Melles technique) from January 2011 to December 2017. Patients with advanced keratoconus, without history of corneal hydrops corneal scar, enrolled in the study.
Advanced keratoconus defined as patients who were intolerant of contact lens and corrected distance visual (CDVA) acuity was less than 20/80.
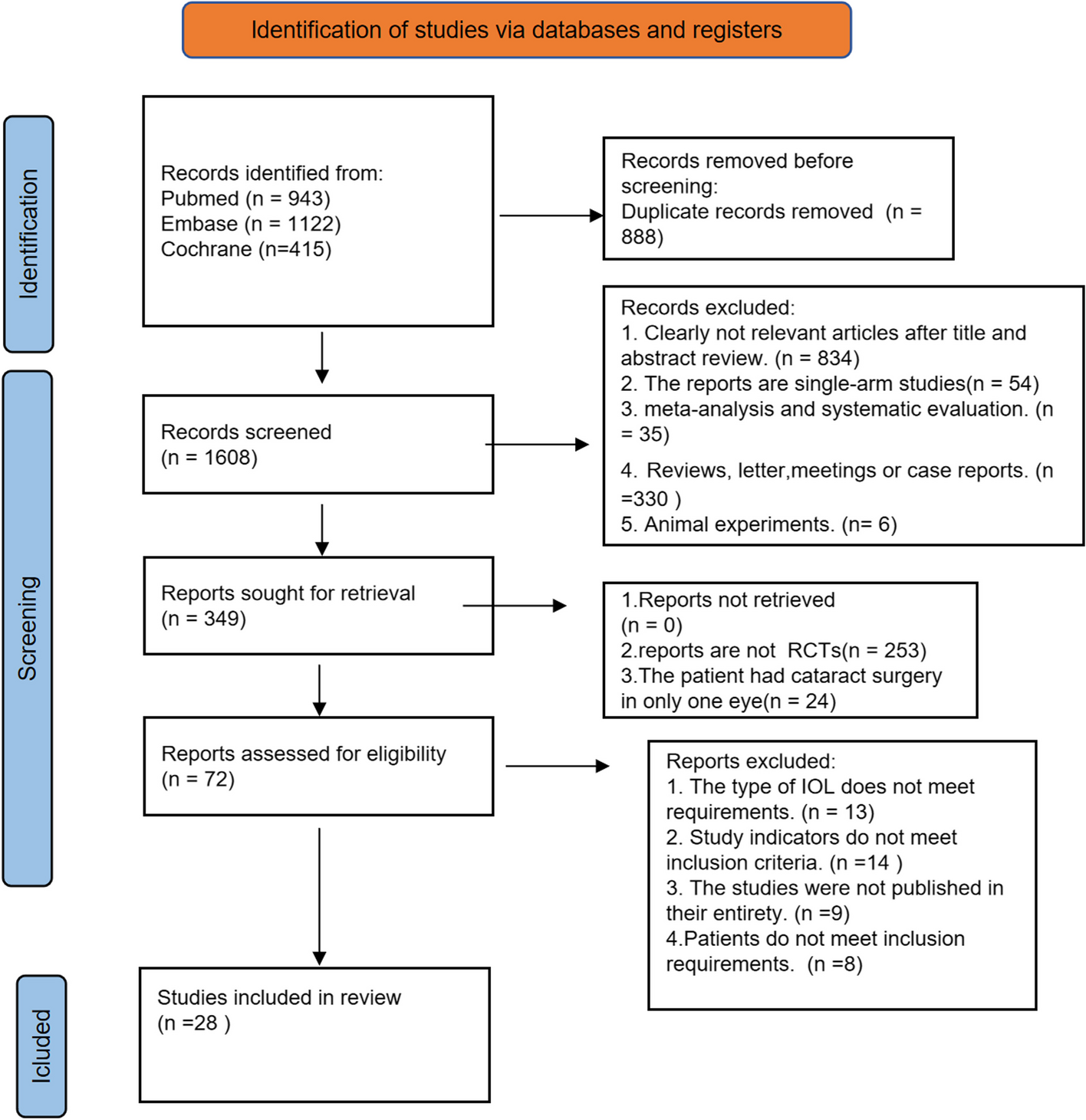
The study included a total of 72 eligible subjects. Following suture removal, all patients included had at least a 6-month follow-up. Patients are summoned for complimentary ophthalmic exams once informed consent is obtained. A comprehensive ocular examination, including uncorrected visual acuity (UCVA), snellen best spectacle-corrected visual acuity (BSCVA), tonometry, slit-lamp biomicroscopy, dilated fundus examination and manifest refraction using an autorefractometer (confirmed by manual refraction) done after 6 months from suture removal.
Keratometry, pachymetry using Pentacam (Oculus, Wetzlar,
Germany), corneal endothelial cell profile using specular microscopy (Confoscan 3.4; Nidek Technology, Padova, Italy), and corneal biomechanics properties using Corvis-ST( Oculus Optikgeräte GmbH, Wechsler, Germany) was performed 6 months after the removal of the sutures for all patients and the results recorded in the patients files. These data used to assess which technique provides better visual and structural results.
For determining the visual quality, optical aberration measured with iTRACE (TRACY SYSTEM) device. MTF and PSF measurements generated from root mean square results are used to quantify contrast sensitivity. Using wave front aberrometry and corneal topography data based on placido discs, this aberrometry provides information regarding corneal and internal aberration. HOA data analyzed quantitatively in the central 4-mm diameter up to the fifth order.
To assess the integrity of corneal tissue, biomechanical properties measured by Corvis-ST device. This dynamic Scheimpflug analyzer record the corneal biomechanics response to certain air pulse pressure, which induces inward deformation in cornea to maximum depth and then rebound to gain its original shape. Intraocular pressure, central corneal thickness, Corvis Biomechanical Index (CBI), Applanation Deflection Length1and 2 (respectively inward and outward movement), greatest concavity Deformation Amplitude, highest concavity Peak Distance, and applanation velocity1and 2 were measured. According to prior investigations, these criteria are regarded credible.
Exclusion criteria were the history of previous ocular surgery, amblyopia, and history of glaucoma or ocular hypertension previous history of Descemet membrane rupture, cataract, pregnancy and any type of retinal or optic nerve diseases. The patients with history of postoperative complications (epithelial and stromal graft rejection or corneal ulceration) excluded.
Surgical technique
Under general anesthesia, one skilled anterior segment specialist surgeon performs all surgical procedures. The vertical corneal length measured for determining Trephine diameter. The trephine’s diameter was approximately 3 mm smaller than the cornea’s vertical diameter. Mean size of donor graft was 8 mm (7.75-8.25 mm).
Donor tissue trephined 0.25 mm to 0.50-mm larger than the recipient bed in all.
cases based on the vitreous length. DM and endothelium of the donor tissue removed after using trypan blue dye for better visualization. Interrupted sutures with nylon 10 − 0 used to place the graft. Suture removal done regarding postoperative amounts of astigmatism revealed by topographic and Pentacam patterns of the cornea.
Melles technique
The recipient cornea marked into four quadrants to perform dissection with approximate depth of 70% easily. To produce an optical air–endothelium interface, an incision is created at the limbus and the anterior chamber is filled with air. Creating a sclerocorneal tunnel at a depth of 350 m (with a diamond knife) and dissecting the stroma under the guidance of spatula’s mirror reflex. Anterior chamber air bubble removed and balanced salt solution replaced. Exposed DM protected with the ophthalmic viscoelastic device (OVD). After the removal of dissected stromal layer and irrigation of OVD, prepared donor cornea placed and sutured with nylon 10.0.
The big bubble technique
This technique referred as the most used and faster technique with high rate of DM exposure. The first step in this technique is the suction trephination at depth of 70%. Through the trephination groove a 30-gauge needle bent 65 degree attached to air-filled syringe inserted with bevel facing down toward DM. A plane for dissection with a crescent knife was formed by the big bubble that separated the corneal stroma from the DM. With a 15-degree knife, the bubble burst, and OVD filled the void. Stromal layer dissected in four quadrants removed with microscissors and the rest of the procedure done as mention in Melles technique.
Suture removal performed at last 18 months after surgery and all the parameters were checked at least 6 months after suture removal. The mean follow up of cases was 24 months.
Statistical analysis
IBM SPSS Statistics software, V.24 (SPSS) used to analyze the data. Results reported as mean ± standard deviation (SD) for the continuous variables. The normality of continuous variables assessed using Kolmogorov-Smirnov test and Shapiro-Wilk test. Based on the results of normality in the data, paired t-test and Mann-Whitney test used to compare the two groups. Significance level of statistical tests was considered 0.05 (P = 0.05).





留言 (0)