
記住我

Unlike previous studies, this meta-analysis focused on comparing ovarian endocrine function between the hysterectomy and control groups with comprehensive indicators. In addition, subgroup analysis was used to identify potential source of heterogeneity and factors related to decreased ovarian function in these women.
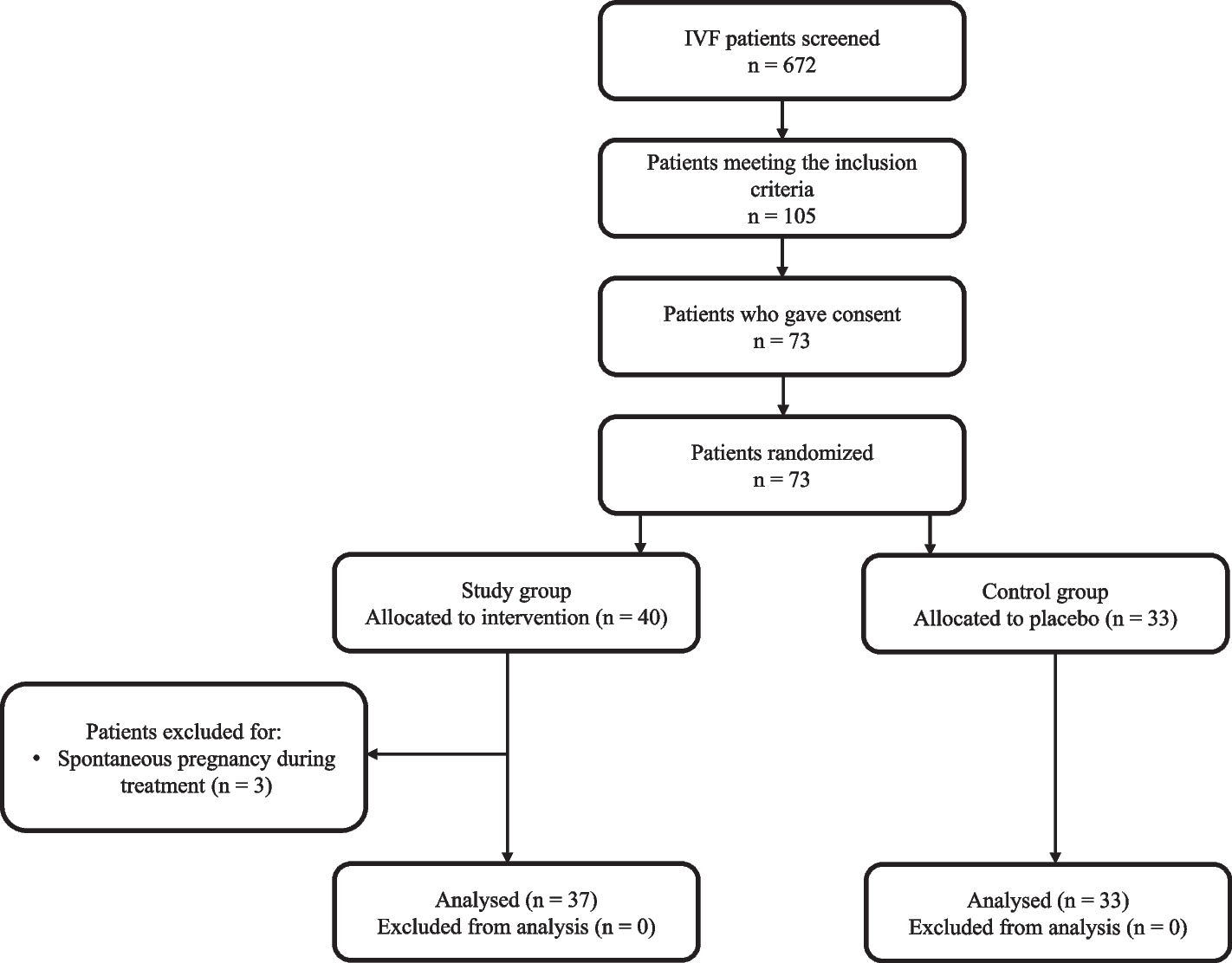
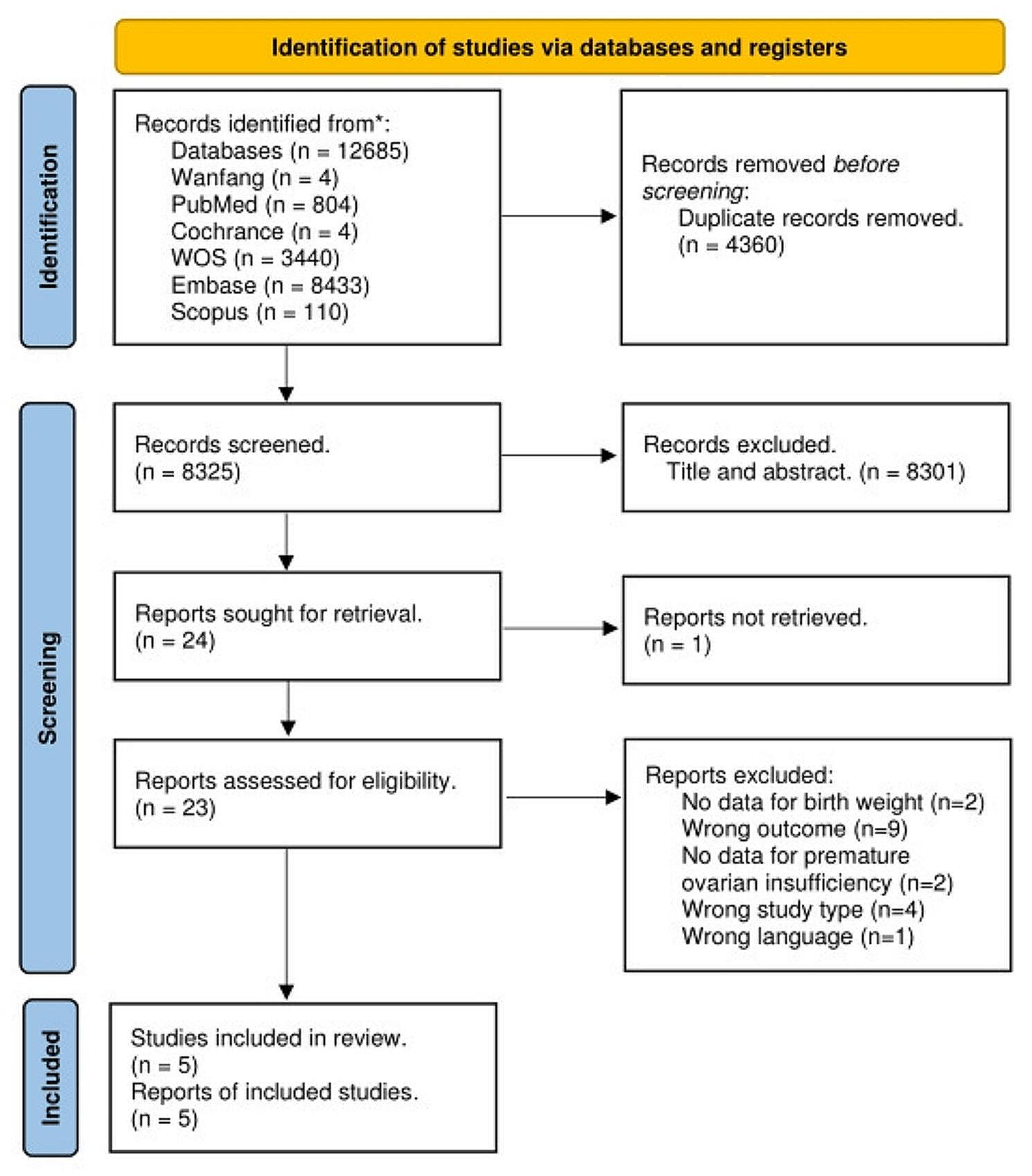
Study selectionThe selection process flow chart is presented in Fig. 1. Initially, 11,911 potential citations were retrieved from the electronic databases, and 42 additional studies were identified by manually searching the reference lists of the included studies. Ultimately, 14 articles were included in the final analysis, including 5 studies examining AMH [20,21,22,23,24], 10 studies examining FSH [11, 22, 24,25,26,27,28,29,30,31], 4 studies examining inhibin B [22, 29, 30, 32], 5 studies examining E2 [22, 28,29,30,31] and 5 studies examining LH [24, 28,29,30,31].
Fig. 1
PRISMA flowchart of 14 selected studies
Study characteristics and risk of biasThe 14 included studies were conducted between 1989 and 2021, involving a total of 1,457 premenopausal women with 760 and 697 in the hysterectomy and control groups, respectively. Among them, 2 studies were RCTs, 10 studies were cohort studies with a pre-post design (9 prospective cohort studies and 1 retrospective cohort study), and 2 studies were cross-sectional. The sample size ranged from 22 to 320 women. Other detailed information on study characteristics is presented in Table 1 and Table S1.
Table 1 Summarized characteristics of 14 selected studiesThe RoB 2 tool was used to evaluate the quality of the 2 included RCTs. Due to the surgical nature, it was difficult to blind study participants and to eliminate deviations from the intended intervention. Thus, all the included trials were deemed to have a high risk of bias for domain of intended interventions (Fig. S1). The quality of the 12 observational studies was assessed by using the NOS checklist. Based on the quality score, all 12 studies scored no less than 5, and no study was excluded (Table S2). The risk of bias summary is presented in Table 1.
Evaluation of ovarian function in premenopausal women who underwent hysterectomySerum anti-Müllerian hormoneThe meta-analysis included 5 studies that evaluated the association between hysterectomy and serum AMH levels via a fixed effect model. The serum AMH levels in the hysterectomy group were lower than those in the control group (WMD = -0.56, 95% CI: -0.72 to -0.39, P = 0.000). In the studies by “Wang (2013)” and “Cho (2021)”, although the baseline AMH levels in the hysterectomy group were lower than those in the control group (Table S3), hysterectomy made this difference more obvious (Fig. S2.a). In addition, there was moderate heterogeneity among the included studies (I2 = 41.3%, P = 0.103) (Table 2, Fig. S2.a). Publication bias, checked by using a funnel plot, Begg’s (z = 1.36, p-value = 0.174) and Egger’s (t = -2.13, p-value = 0.077) tests (Table 3, Fig. S2.b), indicated the low probability of publication bias in overestimating the association between hysterectomy and serum AMH levels. Additionally, the sensitivity analysis generated stable summary estimates without detecting influential publications (Fig. S2.c).
Table 2 Summary of meta-analysis resultsTable 3 Publication bias of the studiesSerum follicle stimulating hormoneA total of 10 studies were included in the analysis of FSH levels via a random effect model, and the weighted mean FSH values from the hysterectomy group were higher than those from the control group (WMD = 2.96, 95% CI = 1.47 to 4.44, P = 0.000). In the study by “Halmesmäki (2004)”, the baseline FSH levels in the hysterectomy group were lower than those in the control group (Table S3), hysterectomy surprisingly caused the higher postoperative FSH levels in hysterectomy group. Heterogeneity among these studies was high (I2 = 91.1%, P = 0.000) (Table 2, Fig. S3.a). Therefore, subgroup analysis was used to identify the potential sources of heterogeneity (Table S4). The results of the subgroup analysis showed that the possible sources of heterogeneity were the patient’s mean age and disease. A mean age ≤ 40 years had less heterogeneity than a mean age > 40 years (I2 = 79.4% vs. I2 = 89.7%, interaction p-value = 0.017). In addition, women with menorrhagia had lower I2 levels than those with uterine leiomyoma (28.1% vs. 91.1%, interaction p-value = 0.000). Furthermore, no significant publication bias (Begg’s test: z = 1.11, p-value = 0.267; Egger’s test: t = -0.77, p-value = 0.450) or influential publications were detected among the pooled results (Table 3, Fig. S3.bc).
Serum inhibin BA total of 4 studies evaluating the impact of hysterectomy on inhibin B values were included. As shown in Table 2, the hysterectomy group was found to be associated with significantly lower inhibin B level (WMD = -14.34, 95% CI = -24.69 to -3.99, P = 0.000). Significant heterogeneity was detected for these studies (I2 = 77.0%, P = 0.000) (Table 2, Fig. S4.a). The results of subgroup analysis showed that world bank countries classification, disease, hysterectomy type, control group are the possible sources of heterogeneity. However, there was only one study in most of these subgroups (Table S5). In addition, no significant publication bias (Begg’s test: z = 1.61, p-value = 0.108; Egger’s test: t = -2.30, p-value = 0.061) and influential publications were discerned across studies (Table 3, Fig. S4.bc).
Serum estradiolAs shown in Table 2, there were no significant differences in E2 levels between the hysterectomy group and control group (WMD = -17.13, 95% CI = -35.10 to 0.85, P = 0.631). In addition, there was high heterogeneity among the 5 included studies (I2 = 92.8%, P = 0.000) (Table 2, Fig. S5.a). The potential sources of heterogeneity were determined by subgroup analysis, which were mean age, BMI, disease and hysterectomy type. Notably, women with a mean age ≤ 40 years had less heterogeneity than those with a mean age > 40 years (I2 = 59.0% vs. I2 = 94.7%, interaction p-value = 0.001) (Table S5). Significant publication bias (Begg’s test: z = 2.14, p-value = 0.033; Egger’s test: t = -2.30, p-value = 0.420) was detected among the included studies (Table 3, Fig. S5.b). Furthermore, the trim-and-fill analyses revealed that publication bias could change the pooled effect size. However, the conclusion (WMD = 2.83, 95% CI = -17.37 to 23.02) remained unchanged after adjusting for publication bias (Table 3). In addition, sensitivity analysis indicated that no individual study had a significant effect on the results (Figure S5.c).
Serum luteinizing hormoneThe meta-analysis included 5 studies that evaluated the association between hysterectomy and serum LH levels via a random effect model. The weighted mean LH values in the hysterectomy group were higher than those in the control group (WMD = 4.07, 95% CI = 1.78 to 6.37, P = 0.000). In the study by “Xiangying (2006)”, the baseline LH levels in the hysterectomy group were higher than those in the control group (Table S3), but hysterectomy also made the difference more obvious (Fig. S6.a). Significant heterogeneity was detected among these studies (I2 = 95.5%, P = 0.000) (Table 2, Fig. S6.a). Sensitivity analysis showed that the potential sources of heterogeneity were mean age, BMI, disease and hysterectomy type. However, there was only one study in most of these subgroups. Similarly, women with a mean age ≤ 40 years had less heterogeneity than those with a mean age > 40 years (I2 = 19.0% vs. I2 = 93.2%, interaction p-value = 0.009) (Table S7). In addition, there was no significant publication bias (Begg’s test: z = 0.18, p-value = 0.855; Egger’s test: t = -0.09, p-value = 0.926), and sensitivity analysis indicated that no individual study had a significant effect on the results (Table 3, Fig. S6.bc).
留言 (0)