Mediastinal schwannomas usually occur in the posterior mediastinum arising from intercostal nerve, sympathetic chain or posterior root of spinal nerve, while those originating from intrathoracic vagus nerve are rare [4]. When these tumors compress the adjacent structures, they will cause symptoms such as chest pain, hoarseness, dyspnea, or dysphagia [5, 6]. Other rare symptoms caused by mediastinal schwannomas include inappropriate secretion of antidiuretic hormone syndrome (IADH syndrome) [7], Horner syndrome [8], intrathoracic bleeding [9], and pleural effusion [10].
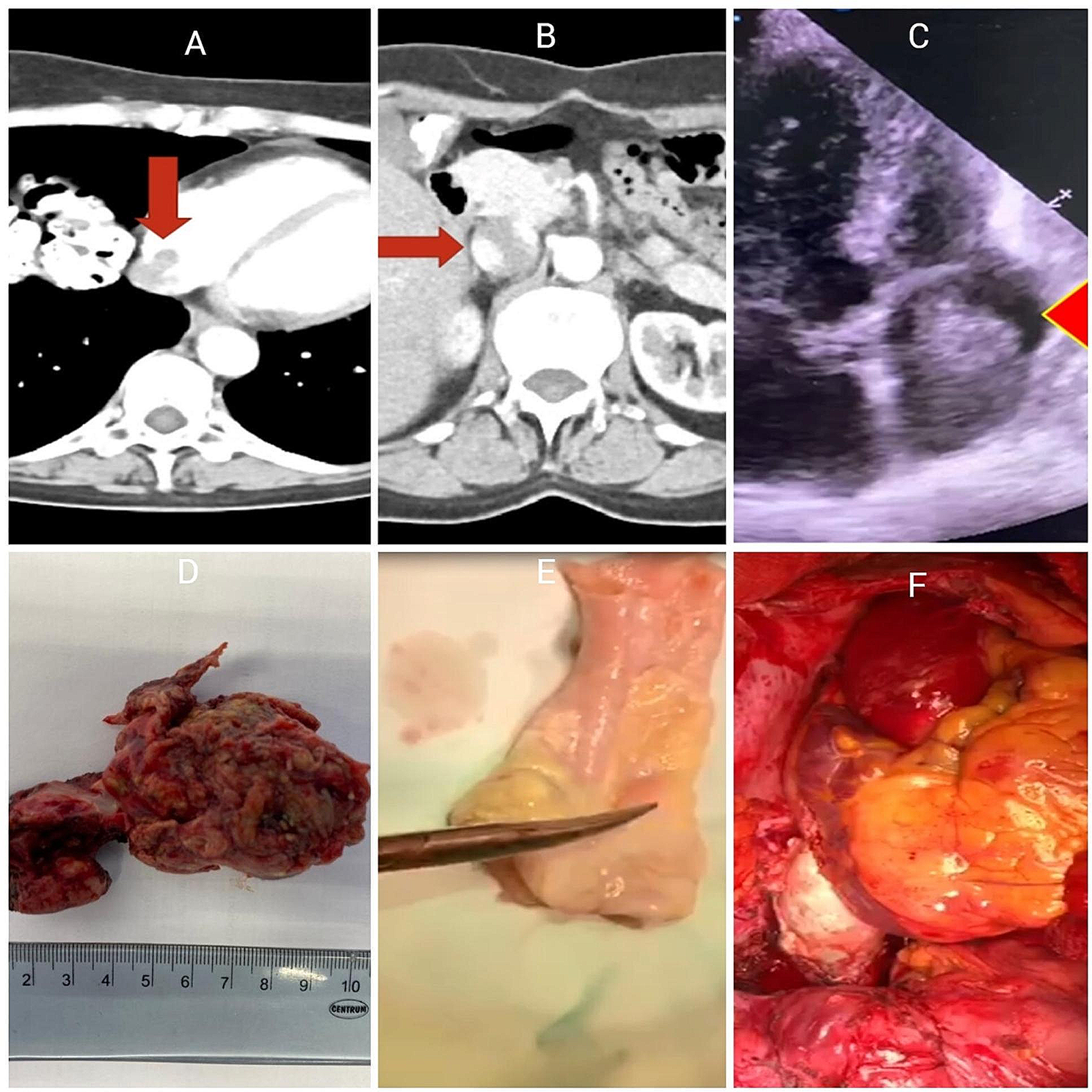
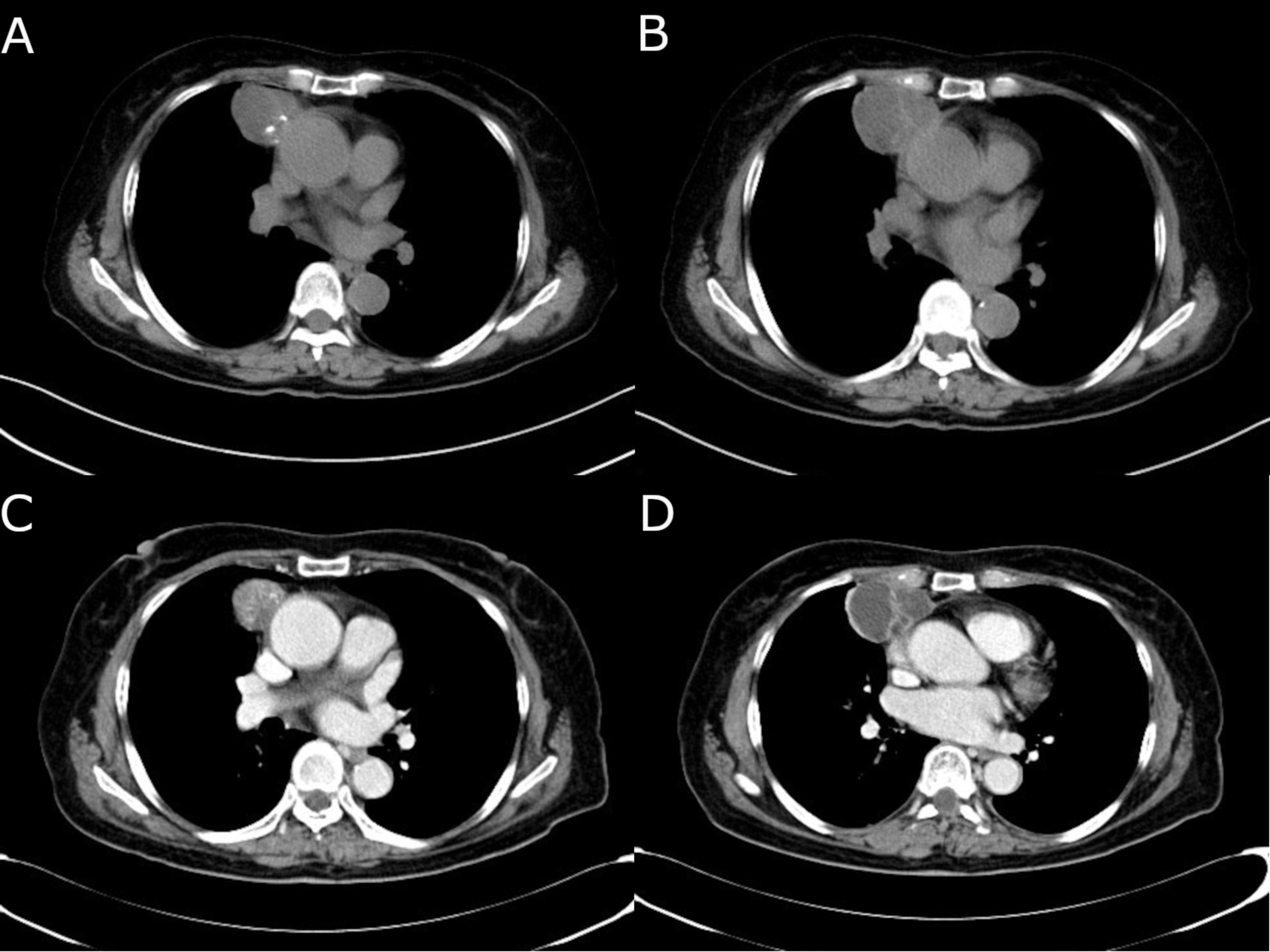
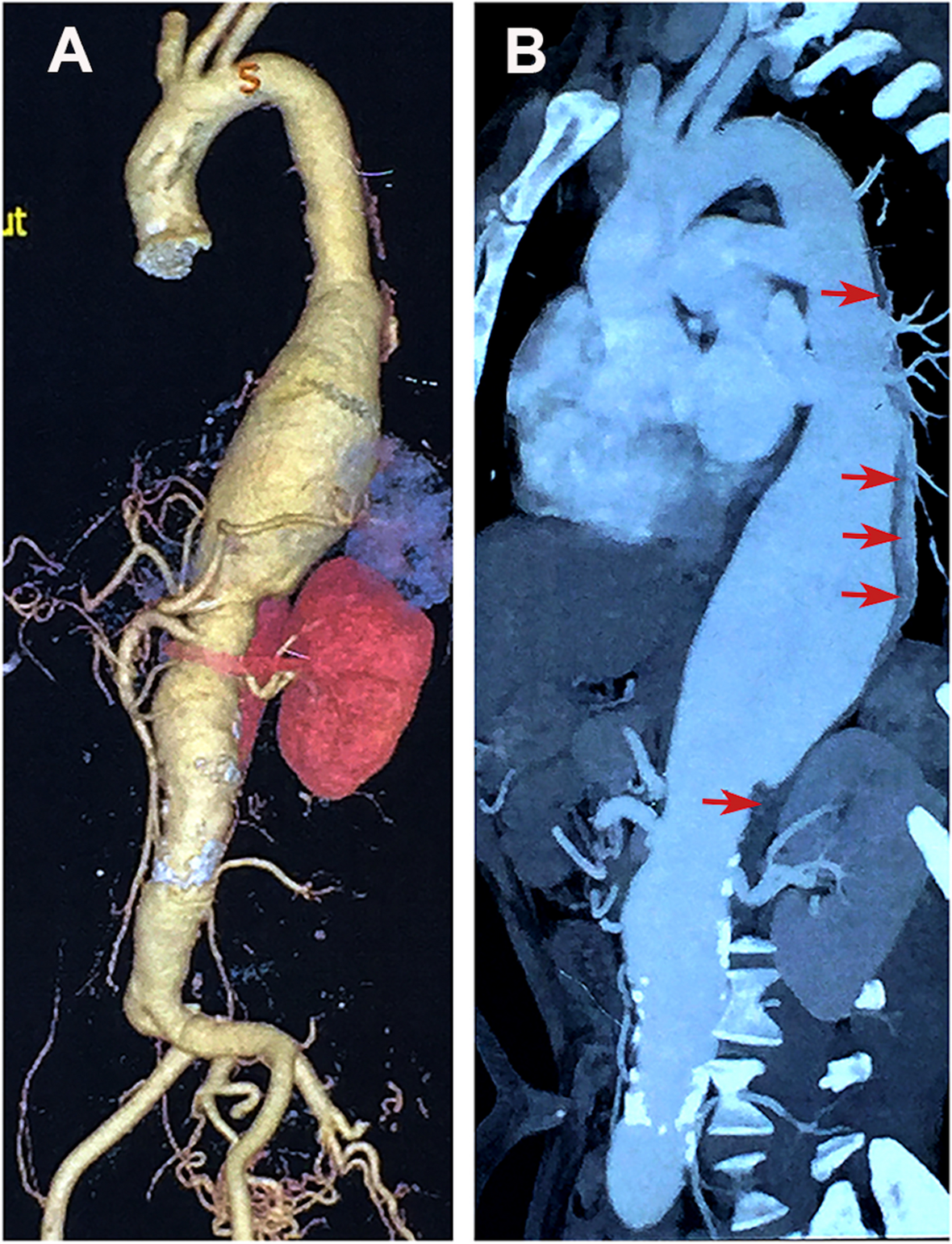
Mediastinal schwannomas present grossly as solitary and well-encapsulated tumors, which have a sharp border with the adjacent soft tissue. Nerve of origin usually present at the periphery of the tumor, instead of penetrating the tumor. CT scan can be used to determine the location of mediastinal schwannoma and its relationship with adjacent tissue. MRI can help better determine the relationship of a mediastinal schwannoma with adjacent vascular structures [11]. Under microscopic examination, mediastinal schwannomas are composed of two histological components: Antoni A areas and Antoni B areas. The Antoni A area is formed by densely arranged spindle cells, and the Antoni B area is formed by loose myxoid tissue, which often develops mucoid degeneration, cystic change or hemorrhage. Immunohistochemical staining of the spindle cells in schwannomas is positive for S-100 protein in cytoplasm, and positive for SOX-10 in nuclear [6].
There are several special variants of schwannoma that have been described in the mediastinum. Ancient schwannomas have a high frequency of regressive changes, such as fatty degeneration, cystic formation, hemorrhage, and calcification, which may grow to unusually large size. This variant of schwannoma still maintains its strong diffuse S-100 positivity by Immunohistochemistry, which helps distinguish it from malignant schwannomas [9]. Melanotic schwannomas are made up of Schwann cells, with capacity for melanogenesis. This variant of schwannoma contains melanosomes in different stage of maturation [12]. Malignant transformation of schwannomas usually occurs to malignant peripheral nerve sheath tumor (MPNST), angiosarcoma or epithelioid malignant change. Malignant schwannoma can exhibit other cellular components such as epithelial cells or mesenchymal features [11].
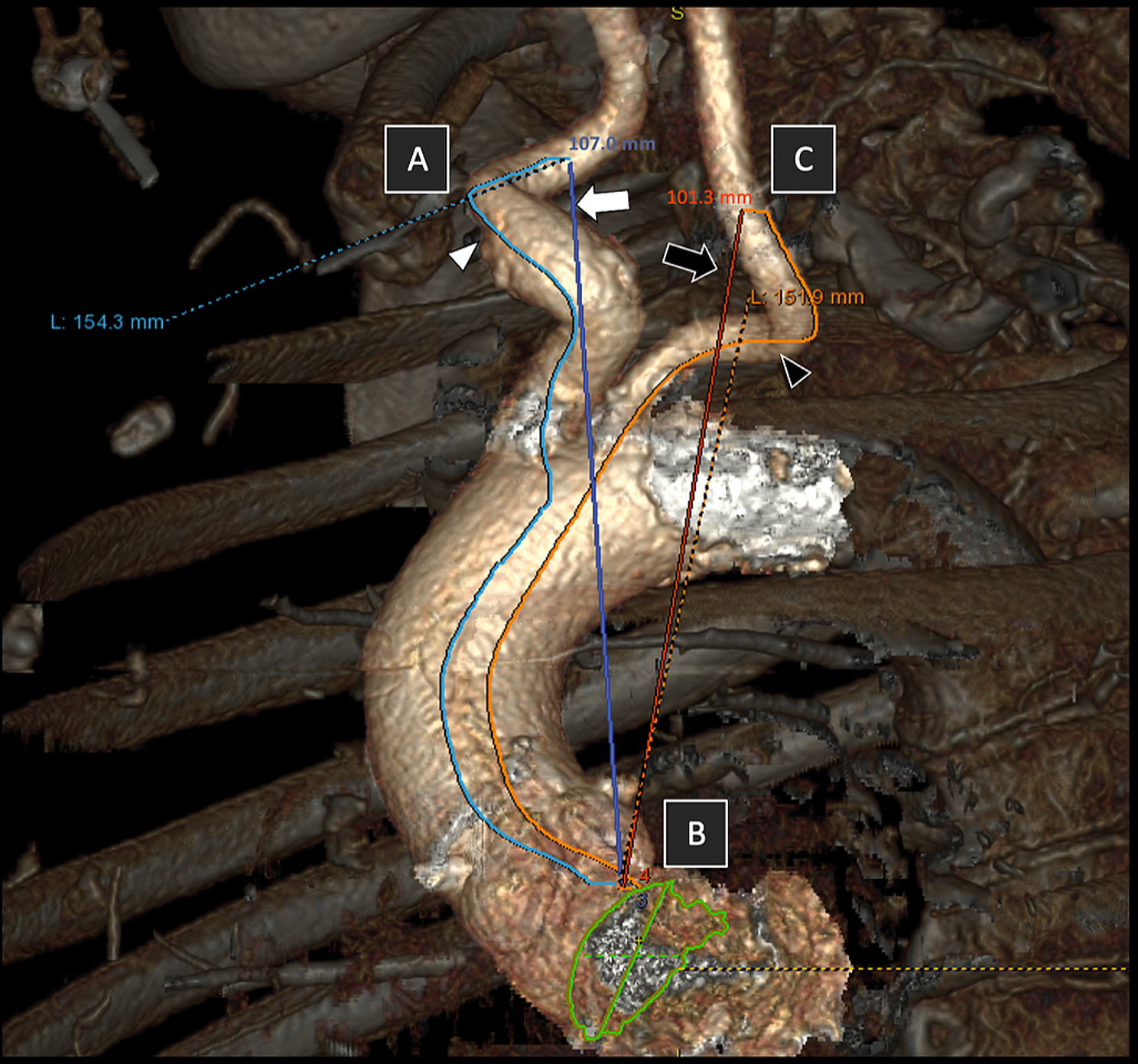
Complete surgical resection is the first-line treatment option for mediastinal schwannomas. Video-assisted thoracoscopy (VATS) technique has been gradually accepted as a safe and reliable access for resection of mediastinal schwannomas, which can reduce surgical trauma, accelerate postoperative recovery, while permit good exposure of the mediastinum. However, for tumors with more than 6 cm in size, or located at the costophrenic angle or thoracic apex, open approaches such as thoracotomy, sternotomy, supraclavicular excision or posterolateral thoracotomy are more appropriate [13]. It has been reported that preoperative angiography embolization could reduce tumor vascularity and operative blood loss, which facilitated the resection of large mediastinal schwannomas [14]. Intraoperative neurostimulation and neuromonitoring approach were recommended to reduce the risk of nerve injury [15].
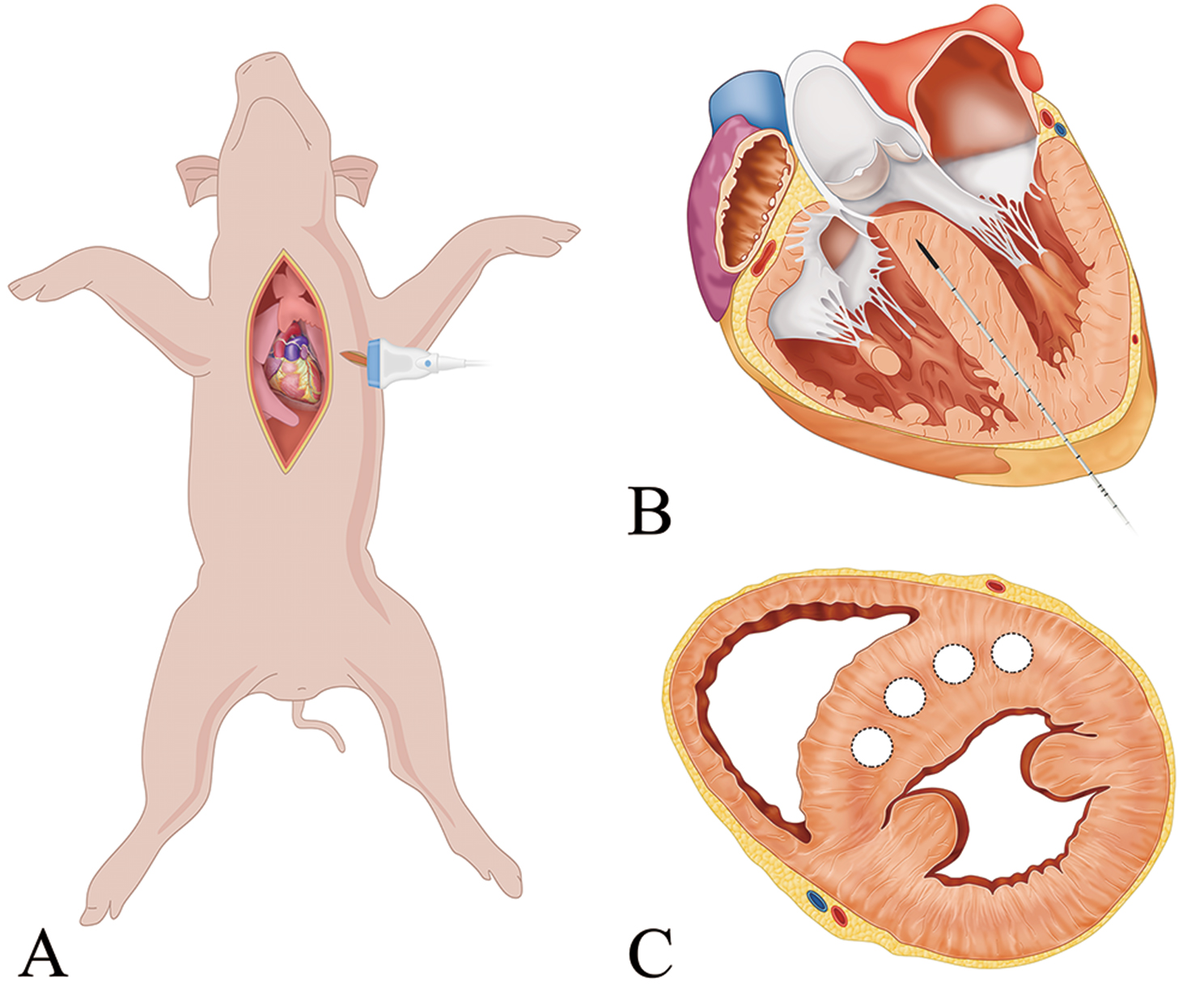
In this case, the essential of the operation was to expose the tumor clearly and to resect it completely, without injuring the vagus nerve. In order to achieve those purposes, we chose a 3 cm uniport through the 4th intercostal at midaxillary line to perform the video-assisted thoracoscopic thoracotomy. Electrocantery and aspirator were used to separate the capsule of the tumor and expose the vagus nerve clearly. After the pedicle of the tumor was adequately exposed, ultrasonic scalpel was used to divide the pedicle and complete the resection.




留言 (0)