We found that during inpatient treatment, moderate to vigorous physical activity levels increased, leading to a greater number of patients engaged in physical activity and, therefore, more patients complying with the 150 min recommendation given by the WHO. The activity levels of patients with a neurotic, anxiety, stress-related, and somatoform disorder diagnosis and of patients with a mood (affective) disorder diagnosis increased the most. In contrast, the activity level of patients with other psychiatric diagnoses changed less or not at all. Furthermore, patients engaged in different amounts of physical activity depending on the kind of ward they resided on. We also found further factors that may influence the level of physical activity.
Documentation of physical activity
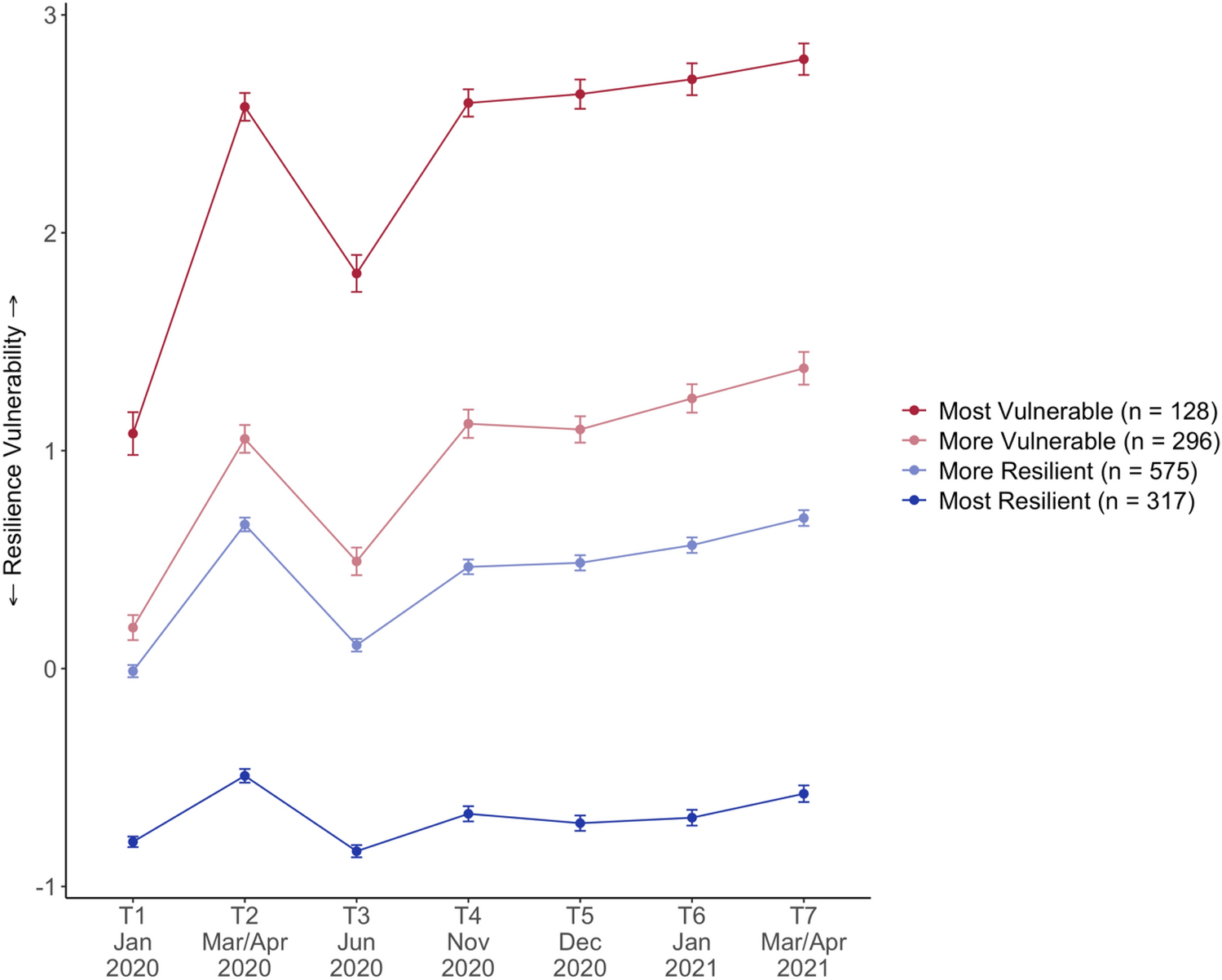
As shown in Fig. 1, the documentation rate increased until around July 2020. However, after July 2020, a decrease in the documentation rate was observed. One reason for this might have been the ongoing COVID-19 pandemic, as some psychiatric wards reduced their capacity, and less attention was granted to the documentation of physical activity. Whether the COVID-19 pandemic influenced physical activity is challenging to analyse in this study. Lower documentation rates and patient numbers do not allow a direct comparison of physical activity pre- and post-pandemic. Due to these circumstances, this limitation may heavily influence the comparison of 2019, 2020 and 2021.
Physical activity levels
We found that during inpatient treatment, the average (moderate to vigorous) physical activity per week increased significantly by 19.04 min. Upon admission, 39.7 min increased to 58.7 min upon discharge. Previous studies found higher physical activity in inpatients and outpatients. For example, in a meta-analysis by Vancampfort et al. a mean physical activity of 90.1 min per day was found in psychiatric inpatients [35]. However, the analysis includes studies with a broad spectrum of mental disorders and physical activity levels, of which some display similar physical activity levels to our study. Furthermore, a considerable variation of programs implemented to promote physical activity in featured clinics can be seen [36]. This feature would lead to a larger dispersion in physical activity levels recorded.
Petzold et al. found an average of 288 min per week of self-reported physical activity in psychiatric outpatients [22]. Chapman et al. found similar results, with 270 min per week of self-reported physical activity in psychiatric outpatients [37]. Compared to our study, the higher physical activity seen in these studies may result from different factors. One, physical activity levels differ between outpatient and inpatients. Studies have shown higher physical activity among outpatients [38], whereas other studies have shown higher physical activity among inpatients [35]. Two, in the studies by Petzold et al. [39] and Chapman et al. [37], the patients were recruited by flyers and doctors, resulting perhaps in higher rates of physical activity due to self-motivation and potentially excluding patients with no interest in physical activity. In our analysis, all patients admitted to the wards were included, showing a more realistic view by decreasing selection bias.
Another outpatient study by Helgadóttir et al. [40] found an even higher physical activity level, with an average of 41.6 min of moderate to intense physical activity per day. This study included patients with anxiety disorder and mood (affective) diagnoses. Our study showed that these patient groups had the highest physical activity levels.
Compared to the abovementioned studies, other studies found lower physical activity levels when measured by an accelerometer [41,42,43]. However, these studies still measured higher levels of physical activity than our study. In one of these studies—using an accelerometer—Jerome et al. took a closer look at the duration of each bout of moderate to vigorous physical activity performed by patients. They distinguished between bouts of 10 min or higher and bouts of any duration (including less than 10 min). When counting bouts of any duration, they found an average of 120 min per week of moderate to vigorous physical activity. However, when only counting bouts of activity with a duration of 10 min or higher, they found an average of 24.9 min per week of moderate to vigorous physical activity performed by patients [41]. This is important when considering the results of this study. When asking patients to recall their physical activity, they are most likely to remember only moderate to vigorous activities that exceed 10 min at a time. This phenomenon may explain the lower physical activity levels found in our study.
Another factor to consider when assessing the results of this study is the individual rather than the overall increase in physical activity. An increase of 19.04 min of moderate to vigorous physical activity per week may seem rather small, however, it is important to consider that only about one-third of the patients engaged in any physical activity upon discharge. This means that these patients engaging in any physical activity actually increased their physical activity levels by roughly 60 min per week. In general, however, clinicians should be aware that the WHO has stated that even small increases in moderate to vigorous physical activity are beneficial to patient health. Therefore, every increase in physical activity is a win [31].
Only 9.5% of patients in our study complied with the WHO recommendation upon admission and 14.6% upon discharge. These numbers are meagre, considering the positive effects physical activity can provide. Moreover, even though the number of patients being physically inactive decreased from 76.2 to 61.9%, showing potential improvement through inpatient treatment, almost two-thirds of patients remain physically inactive. Thus, more systematic interventions are needed to increase physical activity throughout inpatient treatment.
Coleman et al. analysed the exercise as a vital sign (EVS) data of patients in primary care. They found that 36% of patients were inactive, 33% were insufficiently active, and 31% were sufficiently physically active [27]. These findings show a higher percentage of patients engaging insufficiently and sufficiently in physical activity compared to our findings. This difference can be explained by Kruisdijk et al. They showed that healthy individuals, as found in the primary care setting, show higher physical activity compared to patients with mental disorders- the cohort of patients in our study [20].
Psychiatric diagnoses
Patients with neurotic, anxiety, stress-related, somatoform disorder or mood (affective) disorder diagnoses showed a higher physical activity level than patients with other mental disorders. Our finding of low physical activity in patients with schizophrenic, schizotypal, or delusional disorders supports the findings by Vancampfort et al. that patients with schizophrenia show lower physical activity compared to patients with other psychiatric diagnoses [35].
Furthermore, throughout inpatient treatment, patients with a schizophrenic, schizotypal, or delusional disorder diagnosis continued to show a low physical activity level. In contrast, patients with neurotic, anxiety, stress-related, or somatoform disorder diagnoses or a mood (affective) disorder diagnosis further increased the number of minutes spent performing moderate to vigorous physical activity per week. One possible explanation could be that patients with schizophrenia participate in sports therapy significantly less [36] compared to patients with other mental disorders. This might explain the little to no increase in physical activity during inpatient treatment. Another explanation may be an inadequate offer of physical activity interventions for patients with schizophrenic disorders offered during inpatient treatment. The needs of patients with schizophrenic disorders may differ from others and should therefore be explicitly catered to this patient group. Further reasons might be limitations due to higher disease severity and comorbidities associated with schizophrenia or side effects of antipsychotic medication. These factors reinforce the importance of implementing a more specific approach to increase the physical activity of patients with schizophrenia.
Wards
The open ward showed the highest physical activity upon admission, followed by the day-clinic ward. The optionally closed wards showed the lowest physical activity. During inpatient treatment, patients on the day-clinic ward showed a significantly higher increase in physical activity compared to the open and optionally closed wards. On one optionally closed ward, we saw only a slight increase in physical activity. On the other optionally closed ward, we saw a slight decrease in physical activity. Patients in the open ward further increased their physical activity.
A reason for patients’ higher physical activity levels on the open and day-clinic ward may be the lower severity of their mental illness, as patients with severe mental illness tend to be less active. Another explanation for the increased physical activity among patients on the day-clinic ward may be the daily journey to the clinic and back, as some patients might have used bicycles. The free time outside the clinic could have also allowed patients to participate in further physical activities.
To explain the difference between the two optionally closed wards, a closer look at the patient distribution is essential. Optionally closed ward 1 (OCW1) is primarily for patients with mood (affective) disorders, whereas optionally closed ward 2 (OCW2) is primarily for patients with schizophrenic, schizotypal, and delusional disorders. As we showed that patients with schizophrenic, schizotypal, and delusional disorders show lower physical activity than patients with mood (affective) disorders, the difference between these two wards can be explained.
The higher physical activity among patients on the open and day-clinic wards still raises the question of how to increase physical activity on optionally closed wards. Further studies on specific differences between wards and these patients would be needed to address this.
Exploratory analysis
We found that education, housing situation, employment status, legal guardianship status, residence status, month of admission, year of admission, alcohol intake, nicotine use, drug use, depression severity and duration of treatment were associated with the level of physical activity. Age, gender, BMI and comorbidities showed no significant association with the level of physical activity.
The exploratory analysis indicates that many factors might influence physical activity in patients with mental disorders. The benefit gained by identifying and verifying these factors could be enormous. Upon admission, patients with different needs to increase physical activity could be identified and selected for specific interventions such as individual or group training.
Many factors we identified might seem obvious (such as education and status of employment). Other factors, like the month of admission, seem less obvious. This, however, may indicate the need for new approaches in specific months of the year—especially in the winter. A larger cohort would be needed to verify the factors that we found in this study. This need reinforces the importance of implementing physical activity as a vital sign because only through data can we create an evidence-based approach to meeting the needs of all patients with psychiatric disorders.
Implementing physical activity as a vital sign
Implementing physical activity as a vital sign in everyday clinical practice is an ongoing procedure. Constant meetings with clinicians are needed to explain the importance of implementing physical activity as a vital sign to ensure ongoing documentation. One reason for the difficulty of implementing this tool might be rooted in the lack of education regarding physical activity in medical schools [44, 45]. Physicians need to be aware of the importance of physical activity and engage in more physical activity themselves. There is a strong positive correlation between the physical activity habits and good lifestyle choices of medical students and doctors and their attitude towards physical activity counselling [46, 47]. Patients are also more likely to participate in preventive practices when physicians do so [47]. As we showed in the results section, documentation of physical activity has not been achieved for every patient, and the documentation rate fluctuated in all wards. Hence, optimising the documentation of physical activity is crucial. As Electronic Health Records and reminder systems led to more frequent energy balance counselling in primary care [48], implementing these should be considered to obtain a higher rate of documenting physical activity levels.
Strengths and limitations
One strength of this paper is the selection of patients. As we included all patients on all psychiatric wards, the study cohort is a heterogeneous group. In addition, patients were not actively recruited, thereby minimising selection bias.
However, it is possible that a slight selection bias occurred. Some severely ill patients were in no state to answer questions concerning physical activity and were, therefore, not included in this analysis. Documenting the diagnosis of patients with missing physical activity data could help address this aspect in future studies. Important to note is that during the implementation phase of documenting physical activity levels (during which this study took place), physician adherence to the documentation of physical activity levels could influence data.
One limitation of this analysis is the small number of patients, with only 328 patients meeting all of our inclusion criteria. Therefore, results concerning subgroups with smaller patient numbers should be evaluated carefully. In addition, the factors we identified that might influence the level of physical activity should be considered with caution as more patients are needed to verify these factors. In general, due to its design and the limited statistical analyses, our study only provides explorative information which nevertheless lays an important basis for future studies.
Using a self-report physical activity tool might be another limitation, as patients might state higher or lower physical activity levels than performed. Indeed, previous studies showed that physical activity levels measured with an accelerometer are lower than using a self-report questionnaire [17, 49]. However, according to one study by Tucker et al., this is not true when using exercise as a vital sign (EVS) or physical activity as a vital sign (PAVS) [49]. Physical activity measured with the EVS is even lower than when measured with an accelerometer [50]. Even though the EVS does not fully correlate with the accelerometer-measured physical activity, it showed a high specificity (74–89%) [28] and an accurate negative predictive value [50], making it a fitting tool to identify patients who are not meeting the physical activity guidelines.
Unfortunately, the translation of the EVS into the German language has not yet been validated. This would be an important aspect to investigate in future studies.
Important for future studies on this topic might be to document the clinic’s sports program throughout the year for each ward. This information could help to understand changes in physical activity levels associated with the clinic’s sports program, thereby showing ways of proactively increasing physical activity levels and enabling comparison between clinics.

留言 (0)