
記住我



Brain metastasis is a rare refractory event in patients with urothelial carcinoma (UC). Currently, treatment of brain metastasis has no fixed therapeutic approach. Treatment strategies include neurosurgical resection, stereotactic radiosurgery, and whole brain radiotherapy [1]. Unfortunately, recurrence is often faced after surgery and radiotherapy. Immunotherapy represented by immune checkpoint inhibitors (ICIs) has achieved great success in recent years [2]. Platinum-based chemotherapy is the recommended first-line standard therapy for all metastasis urothelial carcinoma patients eligible for cisplatin or carboplatin [3]. Patients ineligible for platinum may receive immunotherapy, which provides a new treatment option [4,5]. Systemic therapies may achieve intracranial responses, however, high-level evidence is lacking, as patients with BM have routinely been excluded from phase III trials of new systemic treatment strategies [6,7]. Meanwhile, the efficacy of ICIs monotherapy is limited by primary and acquired drug resistance [4,5,8]. Immunotherapy combined with antiangiogenesis therapy has emerged as a new regimen in recent years. We herein evaluated the safety and efficacy of combined immunotherapy and antivascular therapy in an elderly patient with urothelial carcinoma brain metastasis, and summarize the currently available evidence.
Case reportA 78-year-old woman was admitted with impaired limb movement on the right side in October 2021. About 2 years ago, a computed tomography examination was performed for gross hematuria: luminal lesions in the left renal pelvis and upper ureter. Urethral cystoscopy, left ureteroscopy and biopsy were performed on July 4 2019, and the biopsy pathology was considered urothelial carcinoma. She underwent a left nephrectomy and left ureterectomy and recovered well postoperatively. The postoperative pathologic findings were consistent with urothelial carcinoma. She did not search for further treatment except for traditional Chinese medicine after the operation.
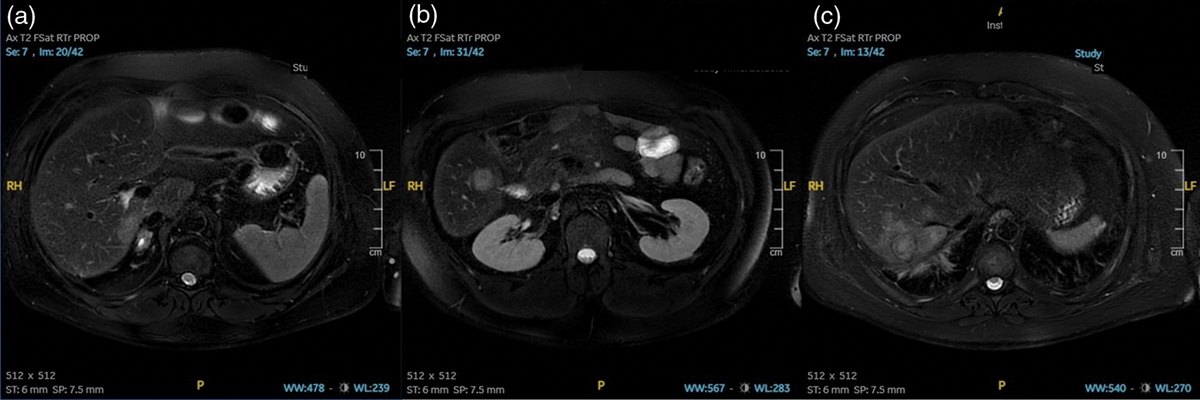
In September 2021, the patient had a sudden onset of right limb inactivity, accompanied by slow response and aphasia. CT was performed on 15 September 2021 (The Second Affiliated Hospital of Dalian Medical University): left frontal lobe occupation. Thereafter, the patient turned to our institute for further treatment on 8 October 2021. On admission, the patient was unresponsive, had aphasia, and impaired right limb movement, with a performance score of about 2. Further brain MRI showed a left frontal lobe mass, surrounded by a large area of cerebral edema, which was diagnosed as a brain metastatic tumor by radiologists in the hospital (Fig. 1a,b). A baseline chest computed tomography scan revealed multiple masses in the upper lobe of both lungs, with large nodules in the upper lobe of the left lung with a maximum diameter of 2.1 cm (Fig. 2a–c). Abdomen computed tomography showed no active findings. The patient was then diagnosed with left frontal lobe metastasis and multiple lung metastases after taking together all the information. The patient has no history of diabetes, hypertension or cardiovascular disease. Thus, one course of radiotherapy for brain metastasis was administered immediately, and local lesion-targeted radiation therapy (total dose of 50 Gy/25F for left frontal lesions) was administered from October 2021 to November 2021. Administration of mannitol and dexamethasone relieved symptoms and improved his status at the same time. All the symptoms were relieved after treatment and the tumor size in the head was reduced through MRI scan (Fig. 1c,d).
 Fig. 1:
Fig. 1: The brain MRI of different times showed a left frontal lobe mass. (a,d) (9 October 2021): A baseline brain MRI scan. (c,d) (10 January 2022) Radiotherapy for brain metastasis was completed more than 1 month. (e,f) (10 February 2022) Radiotherapy for brain metastasis was completed more than 2 months.
 Fig. 2:
Fig. 2: The pulmonary computed tomography (CT) of different times showed multiple metastases in both lungs. (a–c) (12 October 2021) A baseline chest computed tomography (CT) scan. (d–f) (5 January 2022) Radiotherapy for brain metastasis was completed more than 1 month.
Due to the enlargement of intrapulmonary metastases (Fig. 2d–f), an interventional radiology-guided core biopsy of the lesion in the upper lobe of the left lung was performed on 7 January 2022, which demonstrated a poorly-differentiated carcinoma and hematoxylin and eosin staining of the lung lesion revealed that epithelioid tumor cells (Fig. 3a). Furthermore, immunohistochemistry (IHC) revealed CK7(+), CK20(+), GATA3(+), CK(+), HER2(−), P40 (+), TTF-1(focal +) (Fig. 3b–h), which considered metastatic urothelial carcinoma combined with the history and histological findings. A gene analysis of the new puncture sample showed a high tumor mutation burden (12.67 Muts/Mb). Immunohistochemistry indicated negative programmed death ligand-1 expression. Based on these results, this patient may be an ideal candidate for ICIs treatment. The patient did not receive immunotherapy at the time because of her age.
 Fig. 3:
Fig. 3: Histopathologic stains from the upper lobe of the left lung puncture biopsy. (a) Hematoxylin and eosin stain. Magnification: ×100; (b–h) Immunohistochemical stain: B, CK7(+); C,CK20(+); D,GATA3(+); E,CK(+); F, HER2(−); G,P40 (+); H,TTF-1(focal +);(200×).
Unfortunately, the neurological symptoms worsened again after local radiotherapy and which performance for unresponsive, aphasia, and impaired movement of the right limb again. MRI on 10 February 2022 showed that the metastases in the left frontal lobe were larger than before (Fig. 1e,f).Subsequently, lacking standard treatment and with request to try immunotherapy by the patient, toripalimab (a PD-1 mAb) (day 1, 240 mg) plus bevacizumab (day 1, 400 mg) were administered from 18 February 2022.The treatment is given every three weeks. Surprisingly, she quickly achieved response after treatment of toripalimab plus bevacizumab. The clinical discomfort symptoms were quickly relieved a week later; Speech and action almost returned to normal three weeks later, with the retardation disappeared. Response to the therapy was also observed through MRI/CT scan, which showed that the tumor size in the head and both lungs were all reduced after three courses in 30 March 2022 (Fig. 4,5). After six courses on 1 July 2022, the imaging results showed that the patient exhibited continuous partial response (Fig. 4,5).In addition, the toxicities the patient experienced were mainly hypertension, which was well managed.
 Fig. 4:
Fig. 4: The brain MRI of different times showed a left frontal lobe mass. (a,c) (10 February 2022) Before ‘toripalimab plus bevacizumab’ treatment. (b,d) (30 March 2022) After ‘toripalimab plus bevacizumab’ treatment was administered for three cycles. (e,f) (1 July 2022) After ‘toripalimab plus bevacizumab’ treatment was administered for six cycles.
 Fig. 5:
Fig. 5: The pulmonary computed tomography of different times showed multiple metastases in both lungs. (a–c) (5 January 2022) Before ‘toripalimab plus bevacizumab’ treatment. (d–f) (30 March 2022) After ‘toripalimab plus bevacizumab’ treatment was administered for 3 cycles. (g–i) (1 July 2022) After ‘toripalimab plus bevacizumab’ treatment was administered for six cycles.
Although the patient regrettably developed brain metastases and was resistant to radiation therapy, Fortunately, she has a continuous survival benefit from treatment of toripalimab plus bevacizumab, with over 6 months of PFS benefit and over 10 months of OS benefit at the time of this article submission.
In this case report, informed consent was obtained before each treatment. The patients’ responses to all drugs were according to the Response Evaluation Criteria in Solid Tumors (RECIST) criteria, and adverse events were as per the Common Terminology Criteria for Adverse Events criteria.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee(s) and with the Helsinki Declaration (as revised in 2013).The patient signed informed consent forms, which allowed for the publication of the relevant clinical and imaging data from her case.
DiscussionUpper urinary tract urothelial carcinoma (UTUC) represents a rare and aggressive malignancy arising from the renal pelvis or ureter. Platinum-based chemotherapy is the recommended first-line standard therapy for all metastasis urothelial carcinoma patients eligible for cisplatin or carboplatin [3]. The elderly are often complicated with renal insufficiency and cannot tolerate cisplatin chemotherapy. In recent years, Immunotherapy represented by immune checkpoint inhibitors (ICIs) has been a great success and PD-1/PD-L1 checkpoint blockade immunotherapy has been rapidly undergoing a transition from clinical trials to routine clinical practice in multiple tumor types [2,9]. According to the results of IMvigor210, KEYNOTE 052, the United States of America (US) Food and Drug Administration (FDA) and European Association Of Urology (EAU) have approved Atezolizumab and Pembrolizumab for alternative immunotherapy in patients intolerant to platinum chemotherapy [4,5]. Immunotherapy targeting immune checkpoints has become a new therapeutic option for patients with metastatic urothelial carcinoma.
Brain metastasis is a rare refractory event in patients with urothelial carcinoma (UC). Incidence of BM differs between tumors, with the majority of brain metastases occurring in those with lung, breast and colorectal cancers, melanoma or renal cell carcinoma [10]. However, some cases of tumor types such gastro-oesophageal cancers, genitourinary cancers, head and neck cancers and sarcomas are rarely lead to BM. In 2700 cases from the Memorial Sloan-Kettering Cancer Center in New York, Victor et al. reported that the distribution of primary cancers was as follows: 48% lung, 15% breast, 9% melanoma, 1% lymphoma, 3% gastrointestinal, 11% genitourinary, 10% osteosarcoma, 5% neuroblastoma and 6% head and neck cancer [11]. The prognosis of patients with brain metastases is generally poor, and survival is about 4 weeks, if untreated [12]. Development of brain metastases remains a substantial contributor to overall cancer mortality in patients with advanced-stage cancer [13]. Usually, metastatic brain tumors are diagnosed using imaging studies such as computed tomography and MRI [14]. Clinical symptoms or presentation of a patient with brain metastases have been described by Posner et al. In their series study, headache, vomiting and neurological symptoms were predominant clinical presentations in patients [15].
Brain metastases are thought to occur via the seeding of circulating tumor cells into the brain microvasculature; within this unique microenvironment, tumor growth is promoted and the penetration of systemic medical therapies is limited. Currently, treatment of brain metastasis has no fixed therapeutic approach. All of the factors that follow should be taken into consideration: the patient’s general condition, the site and the pathological type of primary disease, the number, size and localization of brain metastases. Treatment strategies include neurosurgical resection, stereotactic radiosurgery and whole brain radiotherapy[1]. WBRT has always been considered as the standard treatment of brain metastases [16].
Systemic therapies may achieve intracranial responses, however, high-level evidence is lacking, as patients with BM have routinely been excluded from phase III trials of new systemic treatment strategies [6,7]. The role of chemotherapy in the treatment of brain metastases is controversial because of the blood-brain barrier. Most authors maintain that most chemotherapeutic drugs cannot pass through the blood-brain barrier hence the chemotherapy efficacy in brain metastatic disease is low or absent [17]. Increased molecular understanding of brain metastases has driven continued development of novel immunotherapies and targeted therapies that have higher bioavailability beyond the blood–tumor barrier. Recently, some studies have shown clinically meaningful activity of systemic agents such as novel immunotherapies and tyrosine-kinase inhibitors in BM patient populations of melanoma, breast cancer and lung cancer, thus providing proof of concept for the efficacy of such approaches [18–21]. Immune checkpoint inhibitors work by activating the human immune system and have become an important method for treating brain metastases [22].
However, the efficacy of ICIs monotherapy is limited by primary and acquired drug resistance. Only 11% to 39% of UTUC patients respond to PD-1/PD-L1 inhibitors according to the current study results [4,5,8]. Immunotherapy combined with antiangiogenesis therapy has emerged as a new regimen in recent years. In terms of the mechanism [23], anti-angiogenic agents can not only reverse the immunosuppressive effects stimulated by vascular endothelial growth factor (VEGF) but also induce the normalization of tumor vascular system and promote the transition of T cells and other immune effector molecules. On the other hand, ICIs can activate effector T cells and increase the infiltration and cytotoxicity of effector T cells to normalize tumor vasculature. A series of clinical trials have also demonstrated that this combination strategy impressively improved the therapeutic efficacy of advanced renal carcinoma, hepatocellular carcinoma, non-small-cell lung carcinoma and other malignant tumors.
In addition, 90% of the patients with brain metastases had peritumoral brain edema (PTBE), which resulted in increased intracranial pressure and even secondary cerebral hernia in severe cases. It was an acute and critical disease of the tumor and a key factor affecting the life quality and duration of the patient [24]. Currently, the conventional treatment for PTBE is glucocorticoid and osmotic dehydrating agent, and the main drugs used in clinical practice are dexamethasone and mannitol [25]. Previous studies [26] have confirmed that PTBE belongs to vasogenic edema, which is mainly caused by increased expression of vascular endothelial growth factor(VEGF), which is similar to the generation mechanism of brain edema associated with radioactive brain necrosis. In recent years, studies have found that the anti-VEGF drug bevacizumab has a significant effect on severe brain edema associated with radioactive brain necrosis [27,28]. Studies have reported that bevacizumab can also treat PTBE. Compared with conventional dehydration, clinical symptoms such as dizziness, headache, nausea and vomiting caused by PTBE can also be alleviated in a shorter time after using bevacizumab, and imaging results show that the range of PTBE is smaller than before [29,30].
Toripalimab (JS001) is a humanized immunoglobulin G4 mAb targeting programmed cell death-1 (PD-1) independently developed by China. Toripalimab received its first global conditional approval in China on 17 December 2018, for the treatment of unresectable or metastatic melanoma after the failure of previous systemic therapy [31]. It has a high binding affinity, which enables it to bind its specific antigen PD-1 receptor more firmly and compete better with PD-L1 and PD-L2 binding on tumor cells. After binding, it can induce strong endocytosis of PD-1 receptor, thus reducing the expression of PD-1 on the cell membrane surface. A study revealed the different binding orientation of toripalimab compared with other PD-1 blockades, which binds PD-1 mainly on a loop that contributes to multiple interactions with PDL1 [32]. Recently, increasing studies about various malignancies have proven the potential superiority of toripalimab, especially good tolerability, which may provide an opportunity to use concurrently with other anti-tumor drugs [33]. The results of the POLARIS-03 study showed that the median OS of patients with advanced urothelial carcinoma treated with toripalimab was 14.6 months, and the ORR was 27.2% [8].
The patient was an elderly woman with urothelial carcinoma diagnosed in gross hematuria 2 years ago and she underwent a left nephrectomy and left ureterectomy. Unfortunately, she recurred 2 years later, presenting as brain and lung metastasis, and worsened again soon after brain radiotherapy. The neurological symptoms performance as unresponsive, aphasia, and impaired movement of the right limb. Based on the above study results, we selected toripalimab immunotherapy combined with bevacizumab after thorough communication with patients. The neurological symptoms were quickly relieved after treatment and the evaluation 3 cycles later showed partial response according to RECIST. In addition, the toxicities the patient experienced were mainly hypertension, which was well managed.
In this case, we found that the TMB was high through genetic testing before treatment. Previous studies have shown that TMB can be used to predict the efficacy of immunotherapy, although it is not a perfect biomarker [34,35]. TMB has been reported to be highly correlated with the efficacy of PD-1/PD-L1 inhibitors in recent years, and high TMB, which represents genomic instability, is considered to have the potential to induce antigen production and further enhance immunogenicity [36]. Current studies have confirmed that TMB can be used as a clinical screening biomarker for the use of ICIs in melanoma, lung cancer and urothelial carcinoma [4,37,38]. However, the majority of patients are nonresponsive to PD-1/PD-L1 monotherapy in unselected populations. The optimization of combined treatment strategies and the search for effective biomarkers that predict the response to immunotherapy remains one of the major drawbacks in cancer management.
There are many kinds of antivascular targeted therapies and ICIs in clinical practice, and the choice of immune combination therapy in the treatment of urothelial carcinoma BM will indeed bring confusion to clinicians. CIs and antiangiogenic drugs have their own side effects, and the toxicity spectrum is more complex than if either therapy were used alone when they are combined. We applied toripalimab combined with bevacizumab in this patient, and achieved satisfactory results; however, when the patient is administered immunotherapy and antivascular targeted therapies, it should be noted that attention must be paid to common adverse reactions such as hypertension, rash, diarrhea and liver function injury; vigilance should also be raised for rare serious adverse reactions such as immune-associated pneumonia, immune-associated myocarditis and myasthenia gravis.
Although the patient regrettably developed brain metastases and was resistant to radiation therapy, Fortunately, she has a continuous survival benefit from treatment of toripalimab plus bevacizumab, with over 6 months of PFS benefit and over 10 months of OS benefit at the time of this article submission, which exceeds the average survival time of previously reported cases.
In conclusion, immunotherapy plus antivascular therapy may be a reasonable option for patients with metastatic urothelial carcinoma, including brain metastases, which is of great significance to prolong the survival period and improve the quality of life of patients.
Because only one patient with metastatic urothelial carcinoma was observed in this report, the clinical data are very limited and further observation and accumulation of more experience are needed, and further clinical studies will be conducted on the efficacy and safety of this combination regimen. We hope to encourage researchers to pay attention to patients with metastatic urothelial carcinoma, including brain metastases. Well-designed trials for better evidence are required to verify the findings in our report in the future.
AcknowledgementsThis study was approved by the institutional review board of Dalian Third People’s Hospital. Written informed consent was obtained from all the patients. No funding was received for this study. Q.F., Y.X. and Y.W. were responsible for collecting data, sorting out data and writing the article; Y.W. was responsible for guiding the writing and participating in the revision of the article, and all authors read and approved the final manuscript.
Conflicts of interestThe authors declare that there are no conflicts of interest.
References 1. Patchell RA, Tibbs PA, Regine WF, Dempsey RJ, Mohiuddin M, Kryscio RJ, et al. Postoperative radiotherapy in the treatment of single metastases to the brain: a randomized trial. JAMA 1998; 280:1485–1489. 2. Ghahremanloo A, Soltani A, Modaresi SMS, et al. Recent advances in the clinical development of immune checkpoint blockade therapy [J]. Cell Oncol 2019; 42:609–626. 3. Roupret M, Babjuk M, Burger M, et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2017 update [J]. Eur Urol 2018; 73:111–122. 4. Balar AV, Galsky MD, Rosenberg JE, et al. Atezoliz umab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial[J]. Lancet 2017; 389:67–76. 5. Ren S, Squires H, Hock E, et al. Pembrolizumab for locally advanced or metastatic urothelial cancer where cisplatin is unsuitable: an evidence review group perspective of a NICE single technology appraisal[J]. Pharmacoeconomics 2019; 37:1073–1080. 6. Eichler AF, Chung E, Kodack DP, Loeffler JS, Fukumura D, Jain RK. The biology of brain metastases-translation to new therapies. Nat Rev Clin Oncol 2011; 8:344–356. 7. Jenkinson MD, Haylock B, Shenoy A, Husband D, Javadpour M. Management of cerebral metastasis: evidence-based approach for surgery, stereotactic radiosurgery and radiotherapy. Eur J Cancer 2011; 47:649–655. 8. Sheng X, Chen H, Hu B, et al. Safety, efficacy, and biomarker analysis of toripalimab in patients with previously treated advanced urothelial carcinoma: results from a multicenter phase II trial POLARIS-03[J]. Clin Cancer Res 2022; 28:489–497. 9. Gedye C, van der Westhuizen A, John T. Checkpoint immunotherapy for cancer: superior survival, unaccustomed toxicities. Intern Med J 2015; 45:696–701. 10. Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol 2004; 22:2865–2872. 11. Yilmazer G, Nart M, Izmirli M, Yavuz A, Can A. Whole brain radiotherapy results of patients with brain metastases and investigation of their prognostic factors. Türk Onkoloji Dergisi 2014; 29:39–45. 12. Sundström JT, Minn H, Lertola KK, Nordman E. Prognosis of patients treated for intracranial metastases with whole-brain irradiation. Ann Med 1998; 30:296–299. 13. Gavrilovic IT, Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol 2005; 75:5–14. 14. Akhavan A, Binesh F, Heidari S. Survival of brain metastatic patients in Yazd, Iran. Asian Pac J Cancer Prev 2014; 15:3571–3574. 15. Posner JB. Brain metastases: 1995. A brief review. J Neurooncol 1996; 27:287–293. 16. Duan L, Zeng R, Yang KH, Tian JH, Wu XL, Dai Q, et al. Whole brain radiotherapy combined with stereotactic radiotherapy versus stereotactic radiotherapy alone for brain metastases: a meta-analysis. Asian Pac J Cancer Prev 2014; 15:911–915. 17. Fabi A, Felici A, Metro G, Mirri A, Bria E, Telera S, et al. Brain metastases from solid tumors: disease outcome according to type of treatment and therapeutic resources of the treating center. J Exp Clin Cancer Res 2011; 30:10. 18. Margolin K, Ernstoff MS, Hamid O, Lawrence D, McDermott D, Puzanov I, et al. Ipilimumab in patients with melanoma and brain metastases: an open-label, phase 2 trial. Lancet Oncol 2012; 13:459–465. 19. Long GV, Trefzer U, Davies MA, Kefford RF, Ascierto PA, Chapman PB, et al. Dabrafenib in patients with Val600Glu or Val600Lys BRAF-mutant melanoma metastatic to the brain (BREAK-MB): a multicentre, open-label, phase 2 trial. Lancet Oncol 2012; 13:1087–1095. 20. Bachelot T, Romieu G, Campone M, et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): a single-group phase 2 study. Lancet Oncol 2013; 14:64–71. 21. Fekrazad MH, Ravindranathan M, Jones DV Jr. Response of intracranial metastases to erlotinib therapy. J Clin Oncol 2007; 25:5024–5026. 22. El Rassy E, Botticella A, Kattan J, Le Péchoux C, Besse B, Hendriks L. Non-small cell lung cancer brain metastases and the immune system: from brain metastases development to treatment. Cancer Treat Rev 2018; 68:69–79. 23. Kazerounian S, Lawler J. Integration of pro-and antiangiogenic signals by endothelial cells. J Cell Commun Signal 2018; 12:171–179. 24. Tsao MN, Khuntia D, Mehta MP. Brain metastases: what’s new with an old problem?. Curr Opin Support Palliat Care 2012; 6:85–90. 25. Moroz MA, Huang R, Kochetkov T, et al. Comparison of corticotropin- releasing factor, dexamethasone, and temozolomide: treatment efficacy and toxicity in U87 and C6 intracranial gliomas. Clin Cancer Res 2011; 17:3282–3292. 26. Gerstner ER, Duda DG, di TE, et al. VEGF inhibitors in the treatment of cerebral edema in patients with brain cancer. Nat Rev Clin Oncol 2009; 6:229–236. 27. Zhuang H, Yuan X, Zheng Y, et al. A study on the evaluation method and recent clinical efficacy of bevacizumab on the treatment of radiation cerebral necrosis. Sci Rep 2016; 6:24364. 28. Wang Y, Wang E, Pan L, et al. A new strategy of CyberKnife treatment system based radiosurgery followed by early use of adjuvant bevacizumab treatment for brain metastasis with extensive cerebral edema. J Neurooncol 2014; 119:369–376. 29. Boothe D, Young R, Yamada Y, et al. Bevacizumab as a treatment for radiation necrosis of brain metastases post stereotactic radiosurgery. Neuro Oncol 2013; 15:1257–1263. 30. Levin VA, Bidaut L, Hou P, et al. Randomized doubleblind placebo- controlled trial of bevacizumab therapy for radiation necrosis of the central nervous system. Int J Radiat Oncol Biol Phys 2011; 79:1487–1495. 31. Keam SJ. Toripalimab: first global approval. Drugs 2019; 79:573–578. 32. Liu H, Guo L, Zhang J, Zhou Y, Zhou J, Yao J. Glycosylationindependent binding of monoclonal antibody toripalimab to FG loop of PD-1 for tumor immune checkpoint therapy. MAbs 2019; 11:681–690. 33. Sheng X, Yan X, Chi Z, Si L, Cui C, Tang B, et al. Axitinib in combination with toripalimab, a humanized immunoglobulin G4 monoclonal antibody against programmed cell death-1, in patients with metastatic mucosal melanoma: an open-label phase IB trial. J Clin Oncol 2019; 37:2987–2999. 34. Chan TA, Yarchoan M, Jaffee E, Swanton C, Quezada SA, Stenzinger A, Peters S. Development of tumor mutation burden as an immunotherapy biomarker: utility for the oncology clinic. Ann Oncol 2019; 30:44–56. 35. Topalian SL, Taube JM, Anders RA, Pardoll DM. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat Rev Cancer 2016; 16:275–287. 36. Wang Z, Duan J, Cai S, Han M, Dong H, Zhao J, et al. Assessment of blood tumor mutational burden as a potential biomarker for immunotherapy in patients with non-small cell lung cancer with use of a next-generation sequencing cancer gene panel. JAMA Oncol 2019; 5:696–702. 37. Van Allen EM, Miao D, Schilling B, Shukla SA, Blank C, Zimmer L, et al. Genomic correlates of response to CTLA-4 blockade in metastatic melanoma. Science 2015; 350:207–211. 38. Rizvi NA, Hellmann MD, Snyder A, Kvistborg P, Makarov V, Havel JJ, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015; 348:124–128.
留言 (0)