
記住我
Substantial evidence has confirmed the efficacy of antipsychotic drugs for treatment of acute bipolar mania. A recent meta-analysis reported that several antipsychotic drugs were associated with greater efficacy in acute bipolar mania, including haloperidol, aripiprazole, asenapine, cariprazine, olanzapine, paliperidone, quetiapine, risperidone and ziprasidone, than placebo.1 The meta-analytic evidence also suggests that some antipsychotics showed greater efficacy than mood stabilisers, such as haloperidol versus lithium (reported standardised mean difference (SMD): −0.26, 95% CI −0.44 to –0.07) and risperidone versus valproate (SMD: −0.38, 95% CI −0.60 to –0.16).1 Several guidelines have recommended atypical antipsychotics as the first-line therapeutic option for acute mania. The Canadian Network for Mood and Anxiety Treatments guideline recommends that quetiapine, asenapine, aripiprazole, paliperidone, risperidone and cariprazine can be used as first-line treatment for patients with acute mania.2 The National Institute for Health and Care Excellence guideline and the Royal Australian and New Zealand College of Psychiatrists clinical practice guideline recommend antipsychotic monotherapy as the first-line treatment for acute mania, and its combination with lithium or valproate as the next step if insufficient efficacy ensues.3 4
The dose equivalence of antipsychotics is important for both clinical and research purposes. When switching antipsychotic drugs or comparing/combining different antipsychotic drugs in clinical trials or meta-analyses, knowledge of dose equivalence for comparable efficacy is needed.5 6 Davis7 used data from double-blind, flexible-dose, randomised controlled trials (RCTs) on schizophrenia and estimated the antipsychotic dose equivalents to chlorpromazine 100 mg/day. This method assumed that physicians would adjust the dosages of the experimental drug to obtain the maximum clinical response in these flexible-dose RCTs. Therefore, the reported mean doses could be applied to estimate the clinical equivalent doses between antipsychotics. The equivalence dose reference reported by Davis has been widely applied for decades.8 Leucht et al6 employed the same method and extended the dose equivalence to atypical antipsychotics and shifted the comparator to olanzapine 1 mg/day. Importantly, the antipsychotic drugs have been considered as first-line treatment for bipolar mania2–4; however, there are so far no specific antipsychotic dose equivalents for treatment of bipolar mania. It is unknown that simply borrowing the dose equivalence from RCTs conducted among participants with schizophrenia could be directly translated to patients with acute bipolar mania.9–11 According to the results of network meta-analysis (NMA) studies, the efficacy of antipsychotics may differ between schizophrenia and acute mania.1 12 For example, risperidone was associated with better efficacy than quetiapine in the treatment of schizophrenia (SMD: −0.13, 95% CI −0.23 to −0.04)12; however, risperidone was not associated with better efficacy compared with quetiapine in alleviating acute mania (SMD: 0.22, 95% CI −0.01 to 0.46).12 Therefore, we hypothesised that the equivalent dose of antipsychotics may differ between schizophrenia and bipolar mania.
ObjectiveWe systematically reviewed the RCTs on oral antipsychotic drugs for treatment of acute mania. We first conducted an NMA to compare the efficacy of the included antipsychotics for acute mania and then calculated dose equivalence using the classic mean dose method by Leucht et al.6 Finally, we compared the antipsychotic dose equivalents between acute bipolar mania and schizophrenia.
MethodsSearch strategy and inclusion criteriaWe followed the classic mean dose method by Leucht et al6 to calculate the antipsychotic dose equivalence. The NMA was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guideline for NMA (online supplemental eappendix 1).13 The study protocol was registered on the Open Science Framework (doi: 10.17605/OSF.IO/CYPV6). Two authors reviewed the literature search, data transfer accuracy and statistical analyses, and discrepancies were resolved by discussing with a third author.
The MEDLINE, Cochrane Central Register of Controlled Trials, EMBASE, PsycINFO, ClinicalTrials.gov and WHO ICTRP databases were systematically searched without language restrictions from database inception to 17 September 2022 (online supplemental eappendix 2). We included blinded, flexible-dose RCTs (placebo-controlled, head-to-head or multiple arms) that had used an oral antipsychotic drug for treatment of patients with bipolar I disorder who experienced an acute manic or mixed episode. We also included RCTs that used fixed-dose design initially but allowed investigators to titrate the dose according to patients’ clinical conditions. The following were the PICO (population, intervention, comparison, outcome) settings of the current study: (1) P: adult patients with bipolar I disorder experiencing an acute manic episode; (2) I: monotherapy with an antipsychotic drug; (3) C: a placebo or another antimanic drugs; and (4) O: changes in manic symptoms. We excluded (1) RCTs that used the dose lower than the recommended target range14; (2) studies that enrolled participants with schizoaffective disorder or bipolar II disorder; (3) relapse prevention studies; (4) open-label studies; (5) studies in special populations such as children, adolescents, elderly or patients with treatment resistance; and (6) RCTs with augmentation or combined treatment but without any antipsychotic monotherapy (eg, quetiapine+lithium vs lithium). Therefore, we also included RCTs of antipsychotic monotherapy compared with augmentation or combined antimanic treatment (eg, quetiapine vs quetiapine+lithium) because such RCTs also provided useful information in the arm of antipsychotic monotherapy. Screening and selection of studies were performed independently by four of the authors, with each study assessed by a minimum of two authors. Disagreements were resolved by consulting with the corresponding author.
Outcome measures and target populationWe extracted the bibliographic and background information. We collected data on the changes in manic symptoms at week 3, measured with the Young Mania Rating Scale (YMRS), the Mania Rating Scale from the Schedule for Affective Disorders and Schizophrenia (MRS), or the Manic State Rating Scale. For studies without data on week 3, we used data at the points closest to 3 weeks (2 weeks to 6 weeks). If there were two measures meeting the criteria, we will extract the measure with the lower p value. Intention-to-treat data sets were used when available. We collected the mean daily dose and their SD after 3 weeks of antimanic treatment. If data were only presented in graphs or plots, these data were obtained using WebPlotDigitizer.15 If possible, we estimated the means and SDs from other statistics (eg, sample size, median, range or IQR).16 For missing values, we imputed the data using summary statistics level based on observed SD values from other trials in the meta-analysis.17 18 At least two authors double-checked the data transfer accuracy and calculations.
The primary outcome was weighted mean dose equivalence, and the secondary outcomes were direct ratios and direct and indirect ratio dose equivalences. The Cochrane Risk of Bias Assessment Tool was used to rate the quality of the included studies by two independent authors.19 The included studies were classified as having high, low or unclear risk of bias (ROB) according to the following domains: selection biases (randomisation and allocation concealment), detection bias, performance bias, attrition bias, reporting bias and other bias. In case of discrepancies, another author was consulted to obtain a consensus.
Data analysisWe performed NMA under a frequentist framework using a multivariate random-effects NMA model with the statistical package netmeta in R statistical software V.4.0.2 (R Project for Statistical Computing). We estimated the antimanic outcomes using SMD with 95% CI. The restricted maximum likelihood estimation method was used to estimate the heterogeneity, assuming a common estimate for heterogeneity variance among different comparisons. The transitivity assumption was supported by evaluating the distribution of potential effect modifiers (publication year, sample size, baseline severity, mean age and female percentage). Heterogeneity among the included studies was evaluated by τ statistic. Inconsistency between direct and indirect comparisons was examined using the design-by-treatment and the node-splitting methods. Publication bias was investigated using Egger’s tests and comparison-adjusted funnel plots. The certainty of evidence for the results of NMA was evaluated using the CINeMA (Confidence in Network Meta-Analysis).
The classic mean dose method included three analyses: (1) weighted mean, (2) direct ratios, and (3) direct and indirect ratios.6 The dose equivalent to olanzapine was calculated from the sample size weighted mean dose of each antipsychotic drug divided by the weighted mean dose of olanzapine. The direct ratio analysis was calculated from the mean dose ratio of each antipsychotic drug to olanzapine in RCTs with head-to-head comparisons (vs olanzapine). The calculated direct ratios were then weighted by sample size, producing average weighted direct ratios. The direct and indirect ratio analyses used all ratios in head-to-head comparisons (any comparisons) and then obtained indirect ratio of any antipsychotic to olanzapine. For example, we had a ratio of olanzapine to haloperidol and a direct ratio of aripiprazole to haloperidol; we obtained an indirect ratio of aripiprazole to olanzapine by dividing aripiprazole/haloperidol by olanzapine/haloperidol. We compared the dose equivalents of acute mania with those of schizophrenia obtained from the study by Leucht et al6 using the independent samples t-test. If the efficacy of an antipsychotic drug significantly differed from that of olanzapine, we provided efficacy-adjusted dose equivalents to olanzapine to those antipsychotic drugs by using the formula shown in online supplemental eappendix 3. A two-sided p<0.05 was considered statistically significant. We used GRADE (Grading of Recommendations, Assessment, Development and Evaluation)20 assessment to evaluate the certainty of evidence of antipsychotic dose equivalents to olanzapine. The GRADE assessment was rated by two independent authors. The certainty of evidence was then reported as very low, low, moderate and high.
FindingsThe selection process and the number of included RCTs are shown in online supplemental efigure 1. The current study included 41 studies (42 RCTs) with 11 396 participants experiencing an acute manic episode (online supplemental etable 1). The sample size of the 42 RCTs ranged from 12 to 521, with a mean of 117.61 (59.35). The mean age was 39.32 (13.10) years, 48.77% of whom were female. Among the 42 RCTs, 35 (83.3%) provided data at week 3 (week 3: 35; week 4: 5; week 6: 3). The antimanic drugs investigated included haloperidol (k=9), risperidone (k=6), paliperidone (k=1), ziprasidone (k=3), quetiapine (k=7), olanzapine (k=14), asenapine (k=2), cariprazine (k=3), aripiprazole (k=8) and brexpiprazole (k=2) (online supplemental etable 1). Among the 42 RCTs, only one study had a high ROB (online supplemental efigures 2 and 3).
The network plot is highly connected (online supplemental efigure 4). The size of the nodes corresponds to the number of participants assigned to each treatment, and the width of the lines corresponds to the number of trials evaluating the comparisons. Figure 1 shows the comparative efficacy of the included antipsychotic drugs. The NMA results indicate that risperidone is superior to olanzapine (reported SMD: −0.22, 95% CI −0.41 to –0.02), while brexpiprazole was inferior to olanzapine (SMD: 0.36, 95% CI 0.08 to 0.64). The comparisons of olanzapine with other antipsychotic drugs did not reach statistical significance. The heterogeneity was low to moderate (tau-squared=0.02; online supplemental etable2). The global inconsistency (assessed by design-by-treatment) was statistically significant (Q-value=49.92, p=0.002; online supplemental etable3). However, the local inconsistency showed that there was statistical agreement between direct and indirect estimates (online supplemental etable 4 and efigure 5), except for ziprasidone relative to haloperidol or placebo. The funnel plot and the Egger’s test (p=0.26) did not show publication bias (online supplemental efigure 6). According to the results of CINeMA (online supplemental etable 5), 8 of 78 (10.3%) comparisons for the antimanic efficacy were rated as moderate confidence of evidence, 1 of 78 (1.3%) as low and 69 of 78 as very low (88.5%).
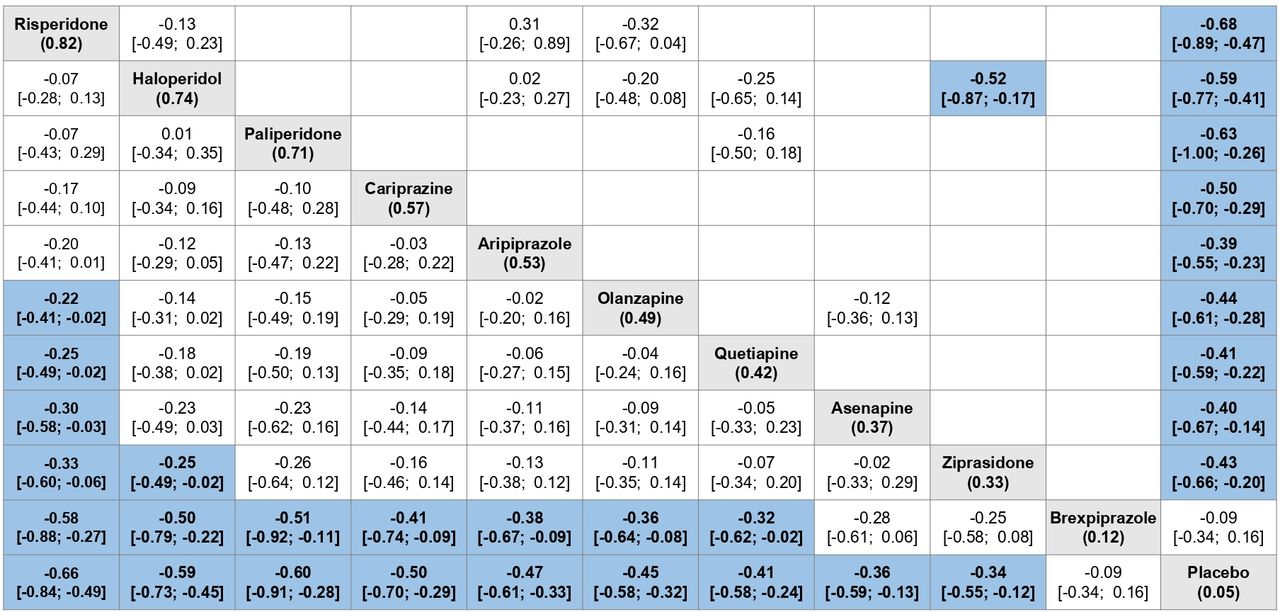 Figure 1
Figure 1 Comparative efficacy (standardised mean difference) in antimanic outcome of the included antipsychotic drugs. Antipsychotics are shown in grey and reported in order of surface under the curve cumulative ranking (given in parentheses). The results of the pairwise meta-analyses are presented in the upper right half and the results of the network meta-analyses in the left lower half. Comparisons between treatments should be read from left to right and the estimate is in the cell in common between the column-defining treatment and the row-defining treatment. In the left lower half, standard mean differences lower than 0 favour the column-defining treatment, and in the upper right half those lower than 0 favour the row-defining treatment. Cells in blue and bold print indicate significant results. Bold type indicates statistical significance.
Table 1 presents the antipsychotic dose equivalents to olanzapine (1 mg/day) for acute mania using weighted mean analyses. For patients with acute mania, the dose equivalents to olanzapine (1 mg/day) were 0.68 for haloperidol, 0.32 for risperidone, 0.61 for paliperidone, 8.00 for ziprasidone, 41.46 for quetiapine, 1.65 for aripiprazole, 1.23 for asenapine, 0.53 for cariprazine and 0.22 for brexpiprazole. The comparisons between acute mania and schizophrenia were significant for haloperidol, risperidone, quetiapine and aripiprazole (all p<0.001). The percentage change in olanzapine equivalent dose from schizophrenia to acute mania ranged from −15.8% to 38.2%. The olanzapine equivalent dose for bipolar mania decreased 15.8% in risperidone and 8.1% in haloperidol, and increased 1.0% in ziprasidone, 17.0% in aripiprazole, 28.5% in quetiapine and 38.20% in asenapine. The efficacy-adjusted dose equivalents to olanzapine (1 mg/day) were 0.19 for risperidone and 0.50 for brexpiprazole. Using weighted mean analyses, all of the certainty of evidence for antipsychotic dose equivalence were moderate, except for haloperidol (low) and brexpiprazole (low).
Table 1Weighted mean analyses for dose equivalents to olanzapine 1 mg
Table 2 presents the antipsychotic dose equivalents to olanzapine 1 mg/day using the direct and indirect ratio analyses. For patients with acute mania, the dose equivalents to olanzapine (1 mg/day) were 0.47 for haloperidol, 0.25 for risperidone, 3.41 for ziprasidone, 1.10 for aripiprazole and 1.15 for asenapine. The comparisons between acute mania and schizophrenia were significant for haloperidol, risperidone, ziprasidone and aripiprazole (all p<0.001). The percentage change ranged from −48.9% to 16.2% for acute mania relative to those for schizophrenia. The olanzapine equivalent dose for acute mania decreased 48.88% in ziprasidone, 38.2% in haloperidol, 12.7% in aripiprazole and 7.4% in risperidone, and increased 16.2% in asenapine. Using direct and indirect ratio analyses, all of the certainty of evidence for antipsychotic dose equivalence were low, except for haloperidol (very low). The results of direct ratio analyses are shown in online supplemental etable 6. The details of GRADE assessment for antipsychotic dose equivalence are shown in online supplemental etables 7–15.
Table 2Direct and indirect ratio analyses for dose equivalents to olanzapine 1 mg
DiscussionTo date, there has been no evidence-based approach to examine the dose equivalents of antipsychotic drugs for acute bipolar mania. Clinicians and researchers still borrowed the dose equivalence derived from schizophrenia for acute bipolar mania. In the current study, we used the approach by Leucht et al,6 estimating the antipsychotic dose equivalents to olanzapine 1 mg/day for acute mania. We also found that the differences in dose equivalence between acute mania and schizophrenia were statistically significant. Substantial evidence has confirmed the efficacy of antipsychotic drugs for patients with acute bipolar mania, and antipsychotic drugs are recommended in several treatment guidelines as first-line treatment for acute bipolar mania.3 4 Therefore, our study findings may provide rational and useful antipsychotic dose equivalents for acute bipolar mania in clinical and research settings.
The classic mean method by Davis and Leucht et al6 7 assumes that physicians would adjust the dosages of the experimental drug to obtain the maximum clinical response in the flexible-dose RCTs, and this assumption was translated to therapeutic equivalence among all antipsychotic drugs for schizophrenia. However, the assumed therapeutic equivalence in the classic mean dose method was not subject to statistical analyses.5 6 In the current study, we conducted NMA to examine comparable efficacy in reducing manic symptoms among all antipsychotic drugs. The NMA results supported therapeutic equivalence among the investigated antipsychotic drugs, except for risperidone and brexpiprazole relative to olanzapine. Global inconsistency was statistically significant, while local inconsistency was only observed in ziprasidone relative to haloperidol and placebo. Notably, we included three RCTs of ziprasidone21–23 and these three RCTs used the MRS as their measurement for the antimanic outcome. However, most of the included studies used the YMRS as their measurement. The inconsistency of ziprasidone relative to haloperidol and placebo might be related to the use of a different rating scale for manic symptoms.
For acute bipolar mania, we found that the results of olanzapine equivalent dose may differ between the weighted mean analyses and the direct and indirect ratio analyses. For example, 1.00 mg of olanzapine was equal to 8.00 mg of ziprasidone in the weighted mean method, while it was equal to 3.41 mg of ziprasidone in the direct and indirect ratio methods. One of the explanations is that olanzapine has been directly compared with only haloperidol, risperidone and asenapine. The accuracy of the direct/indirect ratio analyses depends on the number of head-to-head RCTs; however, among the 42 included RCTs, only 12 head-to-head RCTs contributed to direct or indirect ratios. The limited sample size may explain why we could not calculate the dose equivalent to olanzapine for paliperidone, quetiapine and cariprazine in the direct and indirect ratio analyses.
In the current study, the estimated antipsychotic dose equivalents to olanzapine 1 mg/day were different between acute bipolar mania and schizophrenia, ranging from −15.8% to 38.2% in the weighted mean analyses and from −48.9% to 16.2% in the direct and indirect ratio analyses. These findings might indirectly imply that the effective dose ranges for these two disorders are different. Taking the weighted mean method as an example, the quetiapine dose equivalent to olanzapine 1 mg/day was 41.46 mg/day for acute bipolar mania and 32.37 mg/day for schizophrenia, suggesting that the required dose was higher in acute bipolar mania relative to schizophrenia. However, so far, there has been no expert consensus on the antipsychotic dose ranges for acute bipolar mania, and the target dose range might depend on the recommendations of the manufacturers, which need further investigation.
There are some limitations to other dose equivalence methods for acute bipolar mania. For example, the minimum effective dose, which is the lowest dose that is significantly superior to placebo, was limited to the small sample sizes of fixed-dose, placebo-controlled trials (only eight trials for acute bipolar mania in adults).24 25 The expert consensus method and the daily defined dose method are limited to the relative low evidence-based method.14 25–27 However, as we mentioned above, so far there has been no expert consensus on the target dose ranges for antipsychotic drugs for acute bipolar mania. The latest method by Leucht et al28 overcame the above problems by giving the near-maximum effective doses method. However, based on the estimated dose–response curve, some dose equivalents estimated by this method are far from clinical practice or estimation by other methods. For example, it is reported that 1.84 mg/day aripiprazole is equivalent to 1 mg/day risperidone for schizophrenia.28 Moreover, the near-maximum effective doses method requires (1) antipsychotic dose equivalence to convert all antipsychotic drugs and (2) an adequate number of multiple fixed-dose RCTs for dose–response curve on low doses. These two requirements are still lacking in acute bipolar mania.
LimitationsThere were some limitations to the current study. First, the dose–response curve was not a linear model, but a sigmoid model, and it can differ from drug to drug.28 The weighted mean dose of olanzapine was 14.90 mg/day, and thereby antipsychotic conversion around olanzapine 14.90 mg/day may be more applicable than those far from 14.90 mg/day. Second, the number of patients and head-to-head RCTs was relatively small for some antipsychotic drugs such as paliperidone, limiting the statistical power of these drugs. Third, we focused on the acute antimanic outcomes (week 3); therefore, our findings cannot be generalised to other time scale far from acute manic phase. Fourth, we also calculated efficacy-adjusted dose equivalence for risperidone and brexpiprazole; however, such adjustment was based on the assumption that the mean dose in the included RCT provided the maximum clinical response. Therefore, the dose equivalence for brexpiprazole is limited. Fifth, the certainty of evidence was low to very low for direct and indirect ratio methods. Sixth, we only took antipsychotic monotherapy into account; however, augmentation treatments with mood stabilisers play an important role in clinical scenarios. Our study findings cannot be applied to antipsychotic dose equivalence when using augmentation treatment. Finally, our results were derived from population-level data. When applying the dose equivalents, physicians need to consider patient characteristics such as age, body mass index or stage of illness (eg, treatment resistance).
Clinical implicationsTo our knowledge, this is the first study to assess the antipsychotic dose equivalence for treatment of acute bipolar mania. We found that the antipsychotic dose equivalence for acute bipolar mania is different from schizophrenia. We believe acute bipolar mania warrants its own antipsychotic dose equivalence, and our findings are useful for both clinical practice and future research.
留言 (0)