The limitations of NBI technology have been widely discussed. First, the method requires clear visualization of the mucosa. Thus, if the mucosa is obscured by saliva, blood, or a layer of mucus, the examination is not useful [8]. In addition, a thick layer of hyperkeratosis may be found on some lesions. This phenomenon is called the umbrella effect and may occur in some lesions, particularly in leukoplakia or verrucous carcinoma [8]. This hyperkeratotic layer covers the IPCLs, and the pattern of the vasculature can no longer be seen [8]. Although the interpretation of such findings is very difficult, according to Stanikova et al., the vasculature surrounding the lesion can be used as an excellent diagnostic predictor of the type of lesion [9]. The second limitation is submucosal tumor growth, since NBI can identify only mucosal lesions. When a tumor grows submucosally, the shape of the IPCLs may look normal and the examination might have a false-negative result. The third major limitation mentioned by many authors is the influence of radiotherapy on IPCLs [3,4,5]. If the patient was treated by primary radiotherapy or by the combination of surgery followed by adjuvant radiotherapy, the interpretation of mucosal findings is difficult. The difficulties arise mainly from the fact that radiotherapy alters the characteristics of the laryngeal mucosa and induces inflammatory changes that affect the pattern of IPCLs [10]. Due to the influence of chronic inflammation on the vascular system, detection of possible tumor recurrence can be difficult and may not be diagnosed until an advanced stage, worsening the patient's prognosis [11].
In our study, pathologic changes in the vocal cord mucosa that were present before radiotherapy disappeared after radiotherapy. In the first 3 months after radiotherapy, the mucosal changes regressed and no changes previously observed and interpreted as pathological (perpendicular vessels, leukoplakia) were seen. The first discrete proliferation of new IPCLs was observed 3 months after radiotherapy. The new vessels were always longitudinal. Between 3 and 9 months, the IPCLs underwent significant changes. During this period, the IPCLs became much more visible and an increased number of vessels was observed. The microarchitecture of the vessels also changed during this period. The most common change was ectasia of the vessels. All changes during this period were longitudinal; no changes that could be interpreted as pathology were observed. After 9 months, the vascular changes became stable. Progression of mucosal changes between 9 and 12 months was minimal to nonexistent.
Accordingly, we propose three stages of IPCL changes after radiotherapy: the regression stage, the proliferation stage, and the stagnation stage.
The regression stage starts at the end of radiotherapy and lasts up to 3 months. The proliferation stage describes the main changes and mucosal vessels from 3 to 9 months. The stagnation stage describes the stagnation and de-escalation of changes in the IPCLs seen at 9 months after radiotherapy.
The reason for the appearance of longitudinal vessels after radiotherapy is probably that radiation tends to cause chronic inflammation in tissues [10]. Many classification systems (such as the Ni, ELS, or the Puxxedu classification system) tend to interpret longitudinal vascular changes as benign, and some of the classifications even state that certain types of vascular changes (Ni type II–III, Puxxedu type I) are specific to inflammation [7, 12]. This is also supported by the fact that inflammatory lesions of the vocal cords (such as Reinke edema or chronic laryngitis) tend to have very similar longitudinal vascular changes, although the microarchitecture tends to be different. The caliber of the vasculature in inflammatory lesions tends to be homogeneous, without arborization, whereas the caliber of vessels that change after radiation therapy is usually not homogeneous, and arborization may be present.
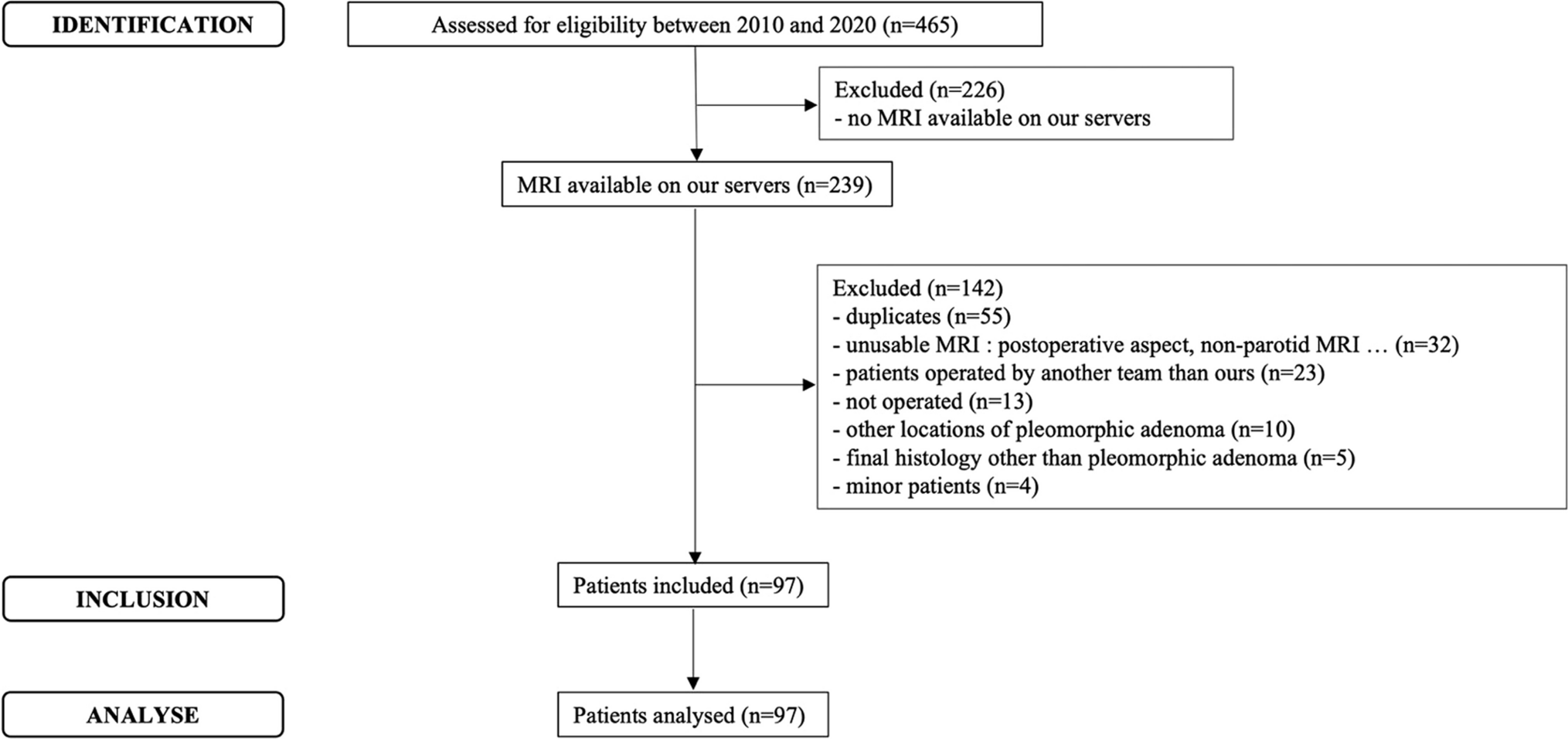
It must be said that the study was limited to a small sample of patients. The number of patients was limited, mainly because the preferred treatment modality for T1 vocal cord carcinoma is cordectomy. This treatment provides good patient outcomes and was the main reason patients were excluded from the study [13]. Although a statistically small sample was used, the consistency of the vascular changes observed was very high and the changes were very similar in all patients in the study.
After the radiotherapy, no perpendicular vasculature was recorded. Therefore, we propose that no special follow-up procedures are required and that patients should be followed in accordance with standard protocols proposed by the European Laryngological Society for patients after treatment for laryngeal cancer [14]. If the patient was treated with curative radiotherapy for glottic carcinoma and the radiation dose was 55 Gy, the longitudinal vessels should be interpreted as radiation-induced inflammatory changes. On the other hand, if perpendicular vasculature is present, the situation should be managed with caution due to probable tumor recurrence, and a sample should be taken for histological examination.



留言 (0)