
記住我





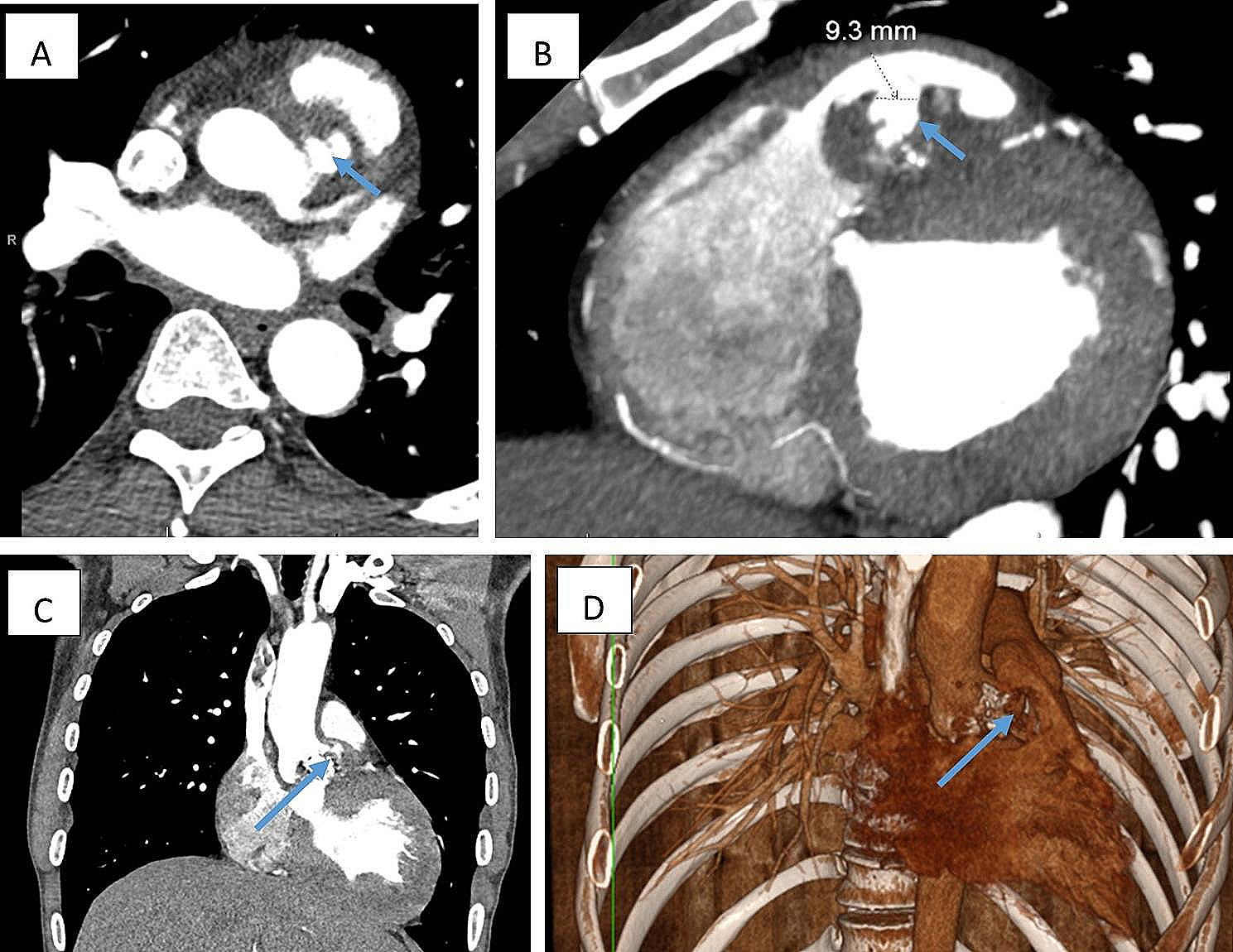
An 81-year-old man, with a 3-day history of loss of appetite and abdominal pain, presented to the emergency department of our hospital with fever and tachypnoea. His hemodynamic status was stable; however, chills, shivering, and mild tenderness in the upper abdomen were observed at presentation. The patient had a history of hypertension, hyperlipidaemia, insulin usage for type 2 diabetes mellitus, percutaneous coronary intervention for unstable angina pectoris, and postoperative lobectomy for right lung cancer. The patient had also undergone pancreaticoduodenectomy for a duodenal papillary carcinoma and had experienced recurrent cholangitis since then. Blood tests revealed a white blood cell count and C-reactive protein level of 12,100/µL and 10.87 mg/dL, respectively. While chest radiography revealed no abnormalities, contrast-enhanced computed tomography (CT) revealed a pseudoaneurysm in the descending thoracic aorta (at the level of Th10) surrounded by fluid accumulation (Fig. 1A, B). Based on the fever, inflammatory response, and the aneurysm shape, we diagnosed the patient with ITAA.
Fig. 1
Computed tomography (CT) before the first thoracic endovascular aortic repair (TEVAR) reveals a ruptured pseudoaneurysm in the descending thoracic aorta (at the level of Th10) surrounded by fluid accumulation (A: 3D CT; B: contrast-enhanced CT)
The patient presented with a pseudoaneurysm and a localised rupture. It was feared that this would progress to a free rupture during the period of intravenous antibiotics and we decided that urgent surgical treatment was necessary. Due to his advanced age and medical history (especially insulin usage for type 2 diabetes mellitus), we determined that he would have a low tolerance for prosthetic graft replacement and performed TEVAR as an emergency procedure. Meropenem and vancomycin were administered intravenously before the TEVAR procedure. If a stent graft was placed extensively on the proximal side, there would be an increased risk of paraplegia. Therefore, a 28 × 100 mm GORE TAG device (W. L. Gore and Associates, Flagstaff, Ariz) was implanted during the procedure to cover the aortic aneurysm protrusion (6 cm proximally from the protrusion and 4 cm distally from the protrusion). One week after TEVAR, a blood culture taken before TEVAR yielded Escherichia coli, so the antibiotic therapy was switched to cefotaxime. The inflammatory response decreased, and the patient remained afebrile; however, CT performed 17 days after TEVAR revealed that the abscess cavity had extended beyond the proximal edge (3.5 cm from the implanted stent graft), i.e., in the area uncovered by the graft (Fig. 2A, B). The aortic wall had become fragile due to infection in this uncovered area and was at risk of rupture. Considering the need for a sufficient landing zone, we implanted a 31 × 150 mm GORE TAG device (W. L. Gore and Associates, Flagstaff, Ariz) on the proximal side with a 3 cm overlap to the previous stent graft. Furthermore, considering the possibility that the patient was refractory to cefotaxime, the antibiotic therapy was switched to meropenem. However, the abscess cavity continued to enlarge (Fig. 3A, B), and we decided to perform a surgical intervention. The patient was re-evaluated for his eligibility for a prosthetic graft replacement; however, the procedure was deemed too invasive due to the initial preoperative risk as well as the patient's worsening frailty. Instead, abscess debridement and pedicled tissue flap were performed for further infection control. The use of the omentum for the pedicled tissue flap was deemed difficult owing to the patient’s history of pancreatoduodenectomy; thus, LDM flaps were selected instead. Preoperative CT showed that on the proximal side, the upper edge of the stent graft was 6.5 cm from the upper edge of the abscess (17.5 cm from the aortic aneurysm protrusion), and on the distal side, the lower edge of the stent graft was 3.5 cm from the lower edge of the abscess (4.5 cm from the aortic aneurysm protrusion). We also confirmed from the preoperative CT that there was no endoleak in the aortic aneurysm and no blood flow from the branch arteries into the aortic aneurysm. Based on the above, because there was sufficient landing zone and no blood flow into the aortic aneurysm, we judged that the risk of bleeding was low. Eighteen days after the second TEVAR, a thoracoscopic abscess debridement was performed to prevent damage to the LDMs intended for use in the pedicled tissue flap. This operation was performed through a small incision made 10 cm away from the left fifth intercostal space. The abscess was located in a sub-adventitial space using ultrasound, and a 5 cm long-axis incision was made through the aortic adventitia. The abscess was debrided and its cavity was cleaned; following this, drains were placed. Similar to the blood culture, a pus culture also yielded Escherichia coli. Seven days after abscess debridement, stent graft wrapping was performed using LDM flaps constructed with the thoracodorsal artery as the feeding vessel. The surgery was performed through thoracotomy at the left fifth intercostal space. We widened the previously debrided aortic exenteration site in a cephalocaudal direction and completely unroofed the abscess cavity. The stent graft was partially exposed (Fig. 4A), and the abscess cavity was thoroughly flushed. The LDM flaps were guided into the thoracic cavity from the second intercostal space and wrapped around the stent graft (Fig. 4B). One week after the stent graft wrapping procedure, debridement of necrosis skin and wound closure were performed using a rectus abdominis musculocutaneous flap due to skin necrosis in the area where the LDM was harvested. Two weeks after the stent graft wrapping procedure, the antibiotic therapy was switched from meropenem to cefotiam based on the pus culture results; it was administered intravenously for 6 weeks after abscess debridement. The patient was then switched to oral levofloxacin, and a lifelong oral antibiotics policy was adopted.
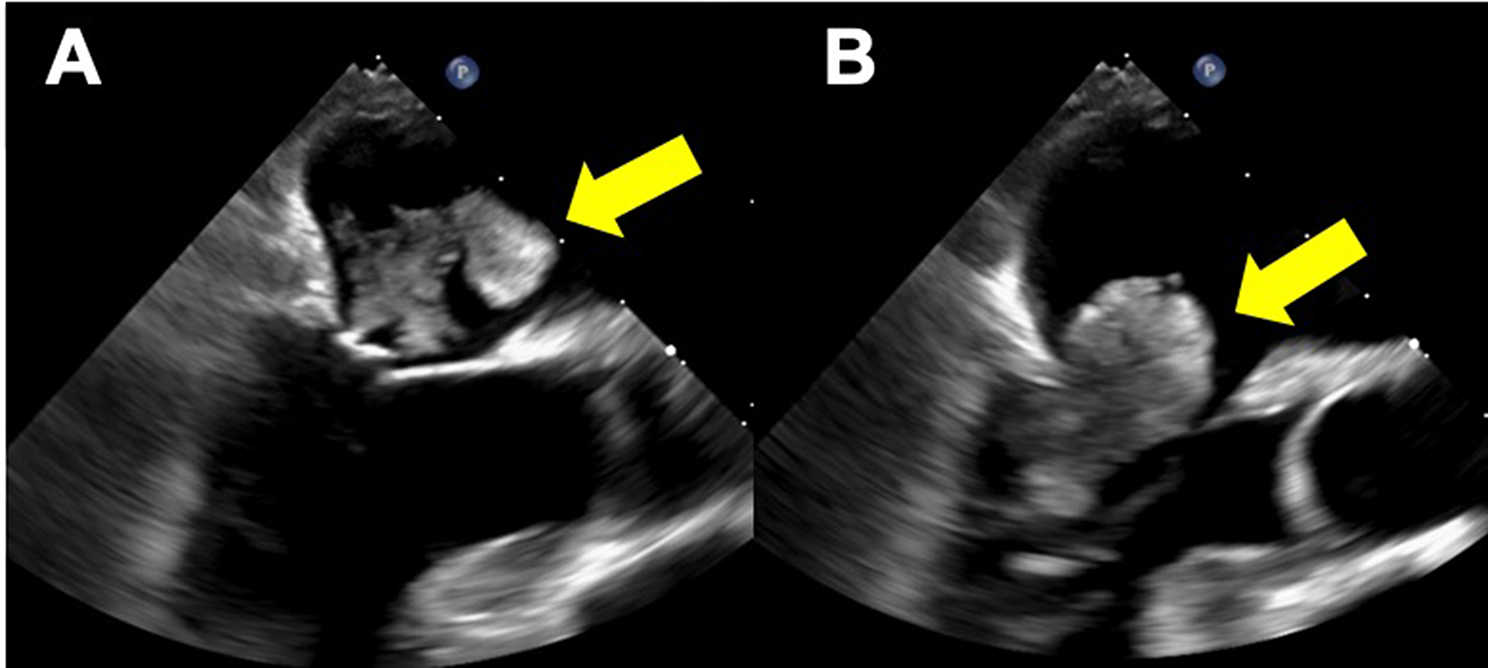
Fig. 2
CT performed 17 days after TEVAR revealed that the abscess cavity had extended beyond the proximal edge from the implanted stent graft, i.e., in the area uncovered by the graft (A: three days after the initial TEVAR; B: 17 days after the initial TEVAR)
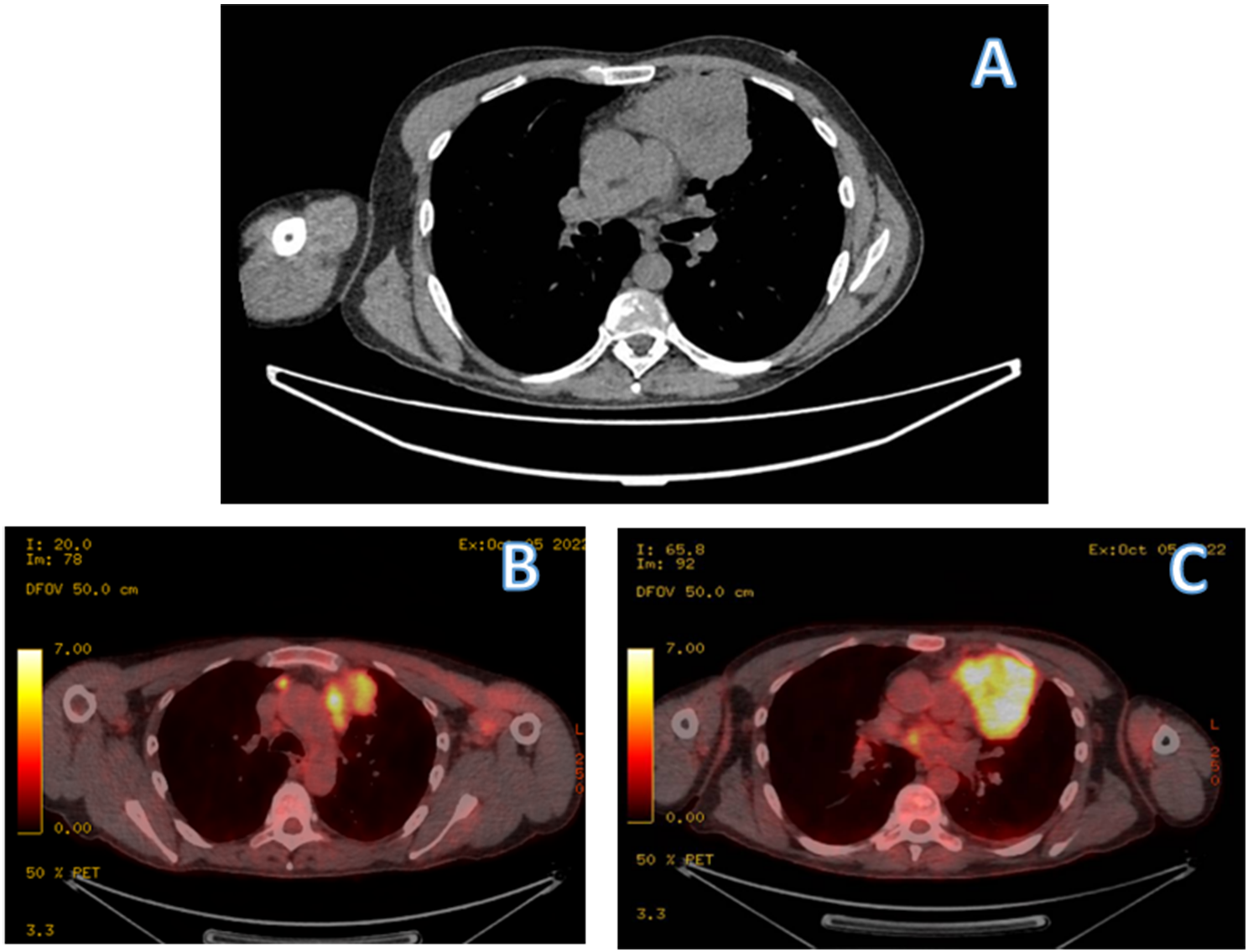
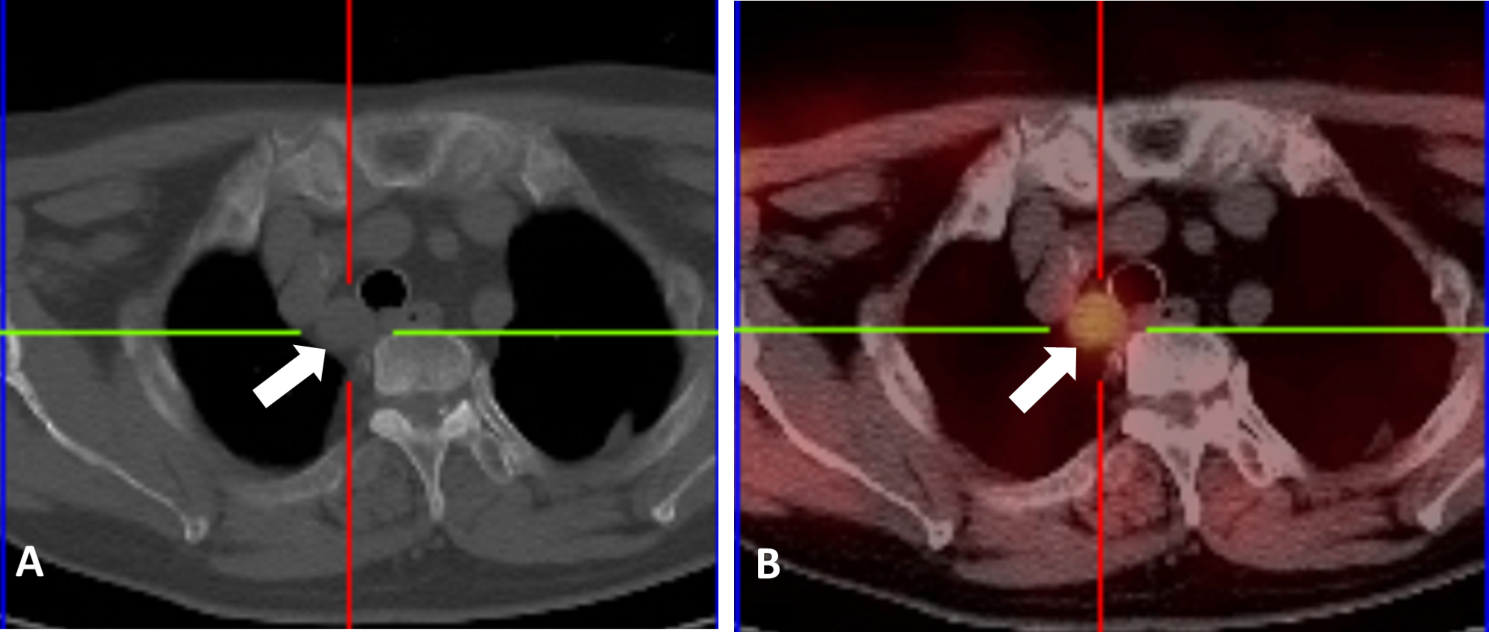
Fig. 3
Despite antibiotic treatment after TEVAR, contrast-enhanced CT suggests abscess expansion over time (A: three days after the initial TEVAR; B: 29 days after the initial TEVAR)
Fig. 4
Operative image of stent graft wrapping using latissimus dorsi muscle (LDM) Flaps. The stent graft is partially exposed when the abscess cavity is released (A). The LDM flaps are guided into the thoracic cavity from the second intercostal space and wrapped around the stent graft (B)
Postoperative CT confirmed that the LDM flaps were wrapped around the stent graft and that there was no bleeding or other complications (Fig. 5). The patient made an excellent recovery and was discharged home on day 77. No recurrent infection was observed at the 8-month outpatient follow-up.
Fig. 5
CT performed 7 days after stent graft wrapping confirmed that the LDM flaps were wrapped around the stent graft and that there was no bleeding or other complications
留言 (0)