
記住我

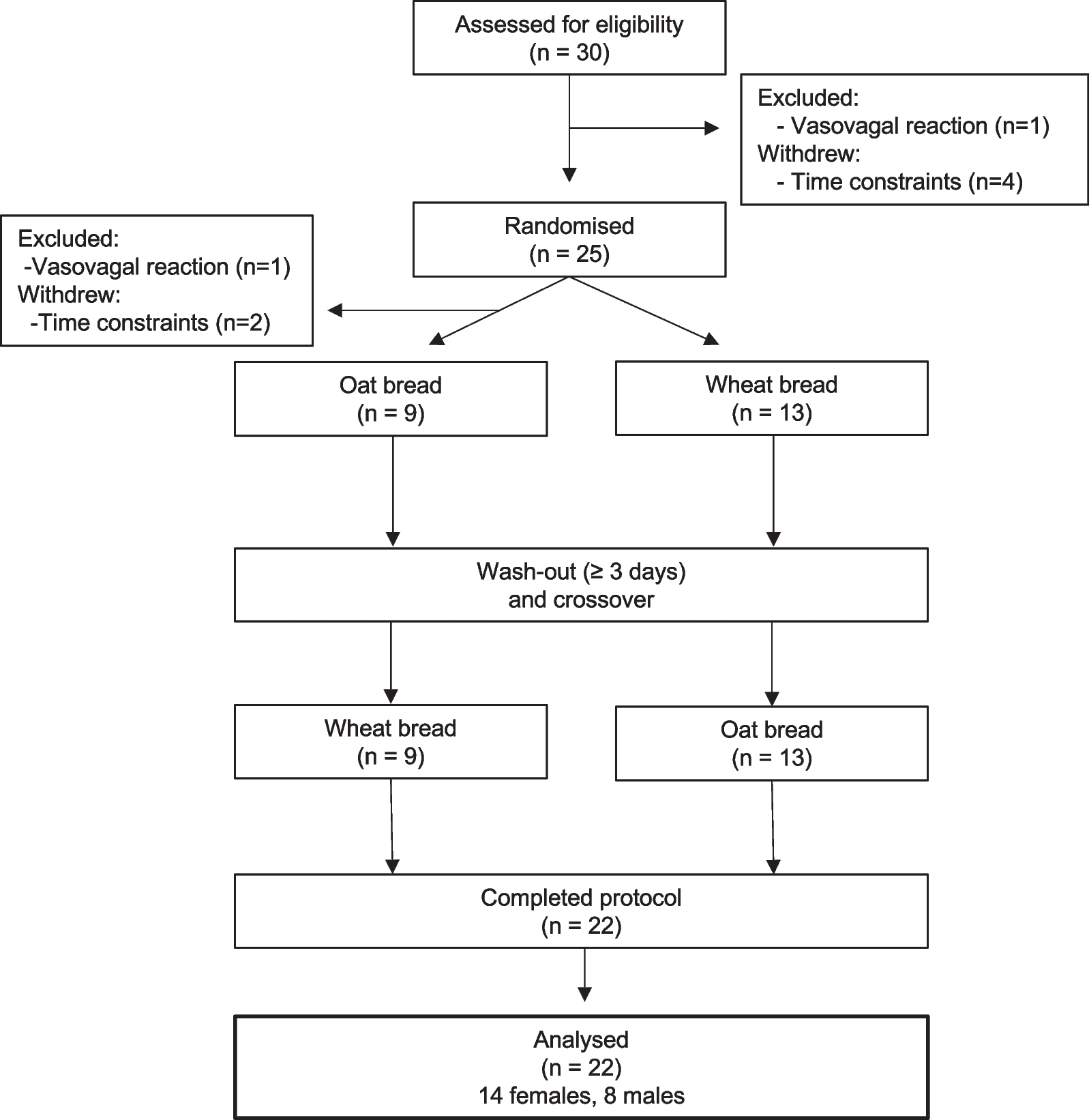

The participants in this prospective cohort study were recruited from Shanghai communities in 2013–2014. All participants underwent a physical examination, laboratory testing, and body composition measurements at baseline. Information on the history of current and past diseases, medication use, smoking habits, menopausal status, family history, and personal habits was collected using standardized questionnaires at baseline [11]. Those with a validated history of malignant tumors, thyroid dysfunction or hyperthyroidism or hypothyroidism, cardiovascular or cerebrovascular diseases, severe liver or kidney dysfunction, treatment with steroids or thyroxine, age < 50 years, or premenopausal women at enrollment were excluded. In 2015–2016, these participants were invited for a second examination which was similar to the previous. Afterward, participants were followed up during 2021–2022 via telephone or electronic medical records (Fig. 1). From the second examination to the last follow-up, the mean follow-up period was 5.5 ± 0.6 years.
Fig. 1
Flow diagram of study population
For this study, 1048 participants undergoing two examinations during 2013–2014 and 2015–2016, non-CVD at baseline and during health examination periods, with complete data, were finally included. When compared with non-respondents (including those with missing covariate data or lost to follow-up), respondents had similar BMI, blood pressure, glucose levels, and lifestyle habits. There were fewer men than women in the current study. All participants provided written informed consent. The study was approved by the Ethics Committee of the Shanghai Sixth People’s Hospital affiliated to Shanghai Jiao Tong University School of Medicine.
Anthropometric and laboratory measurementsHeight, weight, waist circumference, and blood pressure were measured using standardized methods. BMI was calculated as the weight in kilograms divided by the squared height in meters. The total FM, fat%, FFM, and FFM% were measured using an automatic bioelectrical impedance analyzer (BIA; TBF-418B; Tanita Corp., Tokyo, Japan). Changes in each body composition compartment (fat% and FFM%) between the first and second examinations were calculated as percentage change [(value2 – value1)/value1 × 100%]. According to previous literature, age-associated muscle loss begins at around 50 years, with mass loss at a rate of 0.5–1.2% per year [12]. Participants were then categorized into four groups:⊿FFM% < – 8%, – 8% ≤ ⊿FFM% < – 2%, – 2% ≤ ⊿FFM% < 2% (reference group: stable), and ⊿FFM% ≥ 2%. In addition, adults who maintain their weight, lose their FFM and gain a similar amount of fat% [13]. Thus, the same classification method was used for fat% change.
Venous blood samples for the measurement of blood routine, glucose, and lipid levels were drawn after a 10-h overnight fast. Participants without a validated history of diabetes underwent a 75-g oral glucose tolerance test, whereas those with diabetes performed a standard bread meal instead. Homeostasis model assessment of insulin resistance (HOMA-IR) was evaluated using the following formula: HOMA-IR = fasting insulin (FINS) (mU/L) × fasting plasma glucose (FPG) (mmol/L)/22.5 [14].
OutcomeThe primary endpoint was a composite of cardiovascular events, including nonfatal myocardial infarction, unstable angina pectoris, hospitalization for heart failure, coronary revascularization, ischemic stroke, and cardiovascular death [15]. The first occurrence of cardiovascular event was recorded via phone calls or electronic medical records in 2021–2022. Subsequently, two well-trained physicians evaluated the outcome data and used the International Classification of Diseases-Tenth Revision (ICD-10) to identify cardiovascular events (I00–I99).
Diagnostic criteriaCurrent smokers were defined as participants who smoked at least one cigarette per day for more than six months at baseline [16]. According to the International Physical Activity Questionnaire 2010, physical activity levels were classified as light, moderate, and high [17]. Participants were categorized into two groups: BMI < 25 kg/m2 and BMI ≥ 25 kg/m2, based on the World Health Organization 2000 criteria [18]. On the basis of the 2020 guidelines of the International Society of Hypertension [19], hypertension was defined as systolic blood pressure (SBP) ≥ 140 mmHg, diastolic blood pressure (DBP) ≥ 90 mmHg, and/or the use of antihypertensive drugs. Diabetes was diagnosed according to the following criteria: (1) FPG ≥ 7 mmol/L, (2) 2 h-plasma glucose (2hPG) ≥ 11.1 mmol/L, (3) glycated hemoglobin A1c (HbA1c) ≥ 6.5%, or (4) a previous diagnosis of diabetes, according to the guidelines of the 2021 American Diabetes Association [20]. Participants with total cholesterol (TC) ≥ 5.2 mmol/L (200 mg/dL), triglyceride (TG) ≥ 1.7 mmol/L (150 mg/dL), low-density lipoprotein cholesterol (LDL-C) ≥ 3.4 mmol/L (130 mg/dL), high-density lipoprotein cholesterol (HDL-C) < 1.0 mmol/L (40 mg/dL), or using lipid-lowering drugs were identified as having dyslipidemia [21].
Statistical analysisFor continuous variables, normally distributed variables were presented as means ± standard deviations, while skewed variables were described as median and interquartile range. Frequency (proportion) was used for categorical variables. One-way ANOVA, Kruskal–Wallis H test, and chi-square test were used to compare baseline characteristics between fat% change categories for normally distributed, skewed, and categorical variables, respectively. Cox proportional hazards regression analysis was performed to obtain hazard ratios (HRs) and 95% confidence intervals (CIs) of cardiovascular events based on fat% and FFM% changes. Three models were applied: model 1 was adjusted for age and sex; model 2 was further adjusted for lifestyle factors (baseline smoking status, education attainment, family history of CVD, and physical activity); model 3 was further adjusted for metabolic factors (hypertension, diabetes, dyslipidemia, C-reactive protein (CRP), fat%, FFM%, and BMI). The restricted cubic splines with four knots (5th, 35th, 65th, 95th knots) were used to graphically assess the dose–response association between body composition changes and cardiovascular events, because it could better balance both the smoothness of the curve and the accuracy of the model. Interactions of body composition changes with age group (< 65 vs. ≥ 65 years), sex (men vs. women), and overweight/obesity status (BMI < 25 vs. ≥ 25 kg/m2) were examined in the fully adjusted model, and HRs with 95% CIs were calculated for each subgroup. All analyses were conducted using R version 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria), and a two-tailed P < 0.05 was considered statistically significant.
留言 (0)