
記住我


The Ethics Committee of the First Affiliated Hospital of Soochow University approved this study. All the selected patients proved signed informed consent.
Patient selection criteriaInclusion criteria 1.Patients who underwent surgical treatment for acetabular fractures at the First Affiliated Hospital of Soochow University between June 2016 and December 2020.
2.Patients aged 18–82 years (regardless of gender), with acetabular fractures involving the quadrilateral surface according to the Letournel–Judet classification.
3.Acetabular fractures involving the quadrilateral surface, such as an anterior wall or anterior column with a posterior semi-transverse, T-shaped, double-column, or transverse fracture.
4.Patients with a previously exposed quadrilateral surface who had been treated via a lateral-rectus approach combined with an APWLP approach.
5.Patients with complete data who had been followed up for > 1 year.
Exclusion criteria 1.Open fractures of the pelvis or acetabulum.
2.Fractures not treated with an APWLP.
3.Patients with severe medical diseases, such as hepatic or renal insufficiency, hematopoietic diseases, and diseases of the circulatory and respiratory systems, and those who could not undergo surgery.
4.Patients with incomplete medical records or imaging data.
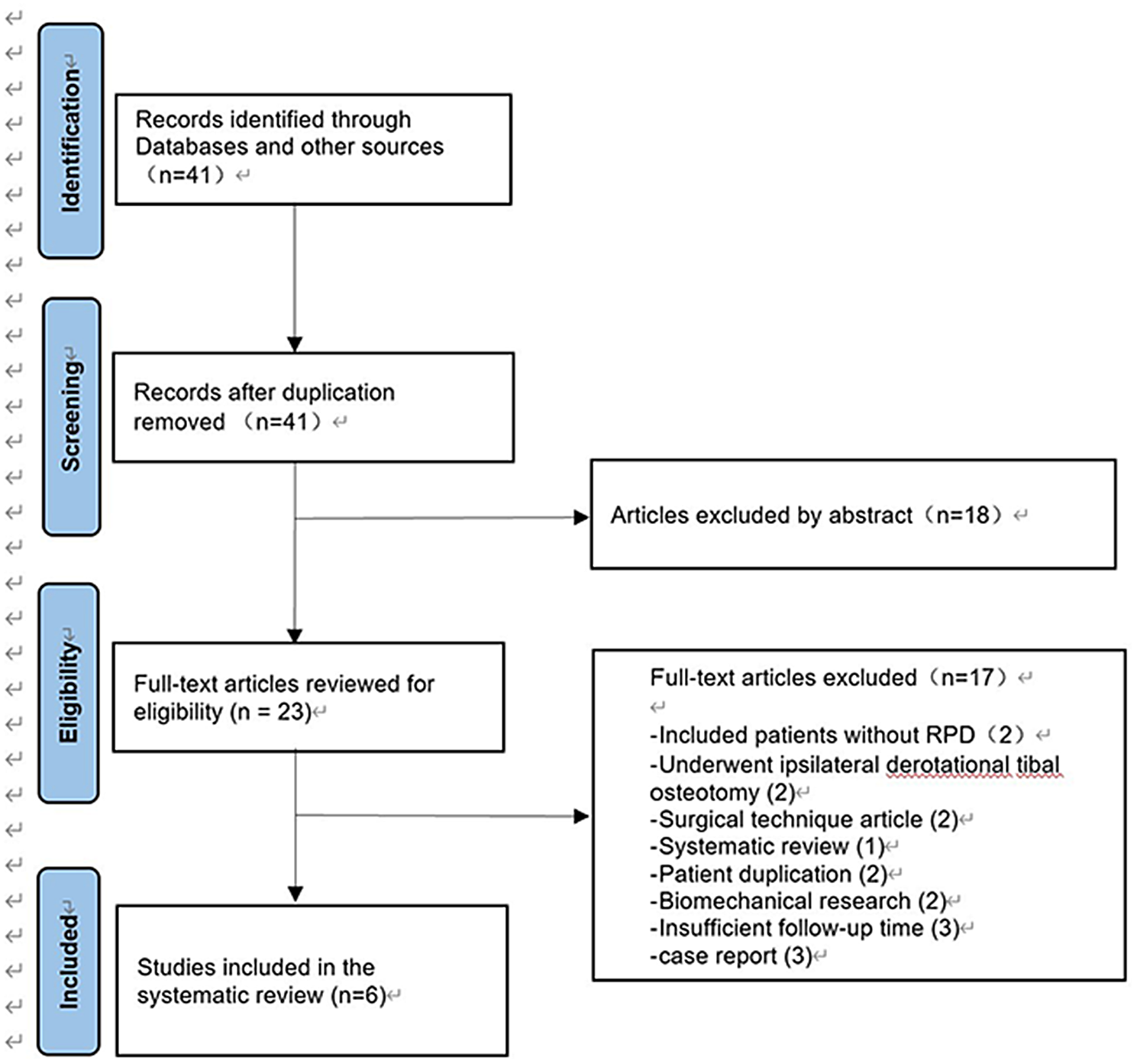
General informationFrom June 2016 to December 2020, 86 patients with acetabular fractures were treated in our hospital. Of the 86 patients, 39 were treated using an APWLP. Out of the 39 patients, one patient lacked complete medical records, and three patients who lacked imaging data were not included in the follow-up. The 35 patients including 25 males and 10 females (23–82 years old; average, 52.45 ± 15.87 years) who met the inclusion and exclusion criteria were available for evaluation (Fig. 3). Fracture classification was based on the Letournel–Judet classification. There were 13 cases of double-column fractures, seven cases of T-shaped fractures, seven cases of anterior wall with posterior semi-transverse fractures, and eight cases of transverse fractures. Among them, 29 cases involved extra-articular pelvic rim fractures. Thirteen cases were injuries from falls (10 from heights of > 2 m and 3 from trips or slip falls), and 22 cases were due to car accidents. The timing of surgery was 2–15 d (average, 5.22 ± 2.70 d).
Fig. 3
A flowchart of inclusions
Surgical techniqueAll operations were performed by a chief physician who had completed acetabular fracture surgery through the lateral-rectus approach for more than 200 patients at our hospital.
First, the patient was placed in the supine position on the operating table to ensure that the C-arm machine could see through the surgical site during the operation. The affected lower extremity was routinely disinfected to facilitate hip flexion surgery and traction to reduce acetabular fractures. Exposure of the belly button and pubic symphysis facilitated the determination of anatomical landmarks during surgery. The lateral-rectus approach was used to expose and fix the fractures. The details of the surgical procedure and operative techniques were previously described by Chen et al. [9]. All of the quadrilateral surface fractures were fixed with an APWLP, and the other fractures were fixed with AO reconstruction plates. The C-arm machine was used once again to assess for fracture reduction and check the position of the plate screw to ensure that the screw did not enter the joint cavity (Fig. 4). The operation time and amount of intraoperative blood loss were routinely recorded.
Fig. 4
A 44-year-old man presented with an anterior column and posterior hemitransverse fracture of the right acetabulum following a traffic accident. The case involved pelvic fractures Preoperative AP (a), iliac oblique position (b), obturator oblique position (c), and 3D CT reconstruction d, e of the pelvis confirmed the fracture pattern. On the 7th day after the injury, fixation was performed through the lateral-rectus approach using an APWLP combined with a reconstruction plate. Postoperative AP (f, i, l), iliac oblique position (g, j, m), obturator oblique position (h, k, n), and 3D CT reconstruction (q, r), showing excellent Matta’s X-ray evaluation scores. Modified Merle d’Aubigné evaluation scores were excellent and hip flexion function o, p was satisfied (f, g, and h are X-rays taken 3 days postoperatively; i, j, and k are X-rays taken 3 months postoperatively; l, m, n are X-rays taken 1 year postoperatively; and q and r are 3D CT reconstructions done 1 year postoperatively)
First-generation cephalosporins were routinely used to prevent postoperative infections within 48 h. Anti-thrombotic pressure bands were applied after surgery to prevent venous thrombosis of the lower extremities. Low-molecular-weight heparin was used for anticoagulation on the first day after surgery. Patients with drainage tubes had the tubes removed when the drainage volume was < 50 mL/d after surgery. The hip joint was actively and passively moved on the second day after surgery, and a walker was used to perform functional exercises within 6 weeks after surgery.
Radiographic and clinical evaluationAll patients underwent three standard plain radiographic examinations, namely for the anteroposterior pelvis and obturator and iliac oblique views, before surgery; 1, 3, 6, and 12 months after surgery; and at the last follow-up. All patients underwent three-dimensional (3D) pelvic computed tomography before surgery. Fractures were classified according to the Letournel–Judet classification.
The quality of fracture reduction was evaluated according to the Matta imaging standard. A fracture displacement of < 1 mm implied anatomical reduction, 1–3 mm implied satisfactory reduction, and > 3 mm implied unsatisfactory reduction.
Clinical outcomes were evaluated according to the modified Merle d’Aubigné-Postel scoring standard. The score evaluation involves three aspects: pain, walking, and range of joint motion. Scores of 18, 15–17, 12–14, and 3–11 points are considered excellent, good, fair, and poor, respectively.
Statistical methodsStatistical analyses were performed using the SPSS 23.0 (SPSS, USA) statistical software, and the data obtained are presented as \(\overline \pm s\). For normally distributed data, a paired sample t test was performed. The enumeration data were tested using Chi-squared or Fisher's exact test. P < 0.05 was considered to indicate statistical significance.
留言 (0)