
記住我
Approximately 8000 people are diagnosed with cholangiocarcinoma annually in the United States, and the incidence and mortality are increasing.1 Extrahepatic cholangiocarcinomas (EHCC) account for ~90% to 95% of all cholangiocarcinomas and are classified as perihilar (tumors located from the junction of the right and left hepatic ducts to the cystic duct) or distal (from the cystic duct to the Ampulla of Vater). Perihilar tumors can be further classified according to the Bismuth-Corlette classification based on the extent of ductal infiltration and resectability.2
Cure of EHCC is achieved through surgical resection, but few patients are candidates for resection up front, and there are high rates of both local and distant failure following resection. As a result, neoadjuvant and adjuvant treatment strategies involving chemotherapy and radiation (RT) have been developed to improve outcomes in patients with EHCC. Orthotopic liver transplant (OLT) following neoadjuvant therapy has also emerged as an effective treatment strategy for select patients. Treatment for unresectable patients involves chemotherapy, RT, or a combination in appropriately selected patients.
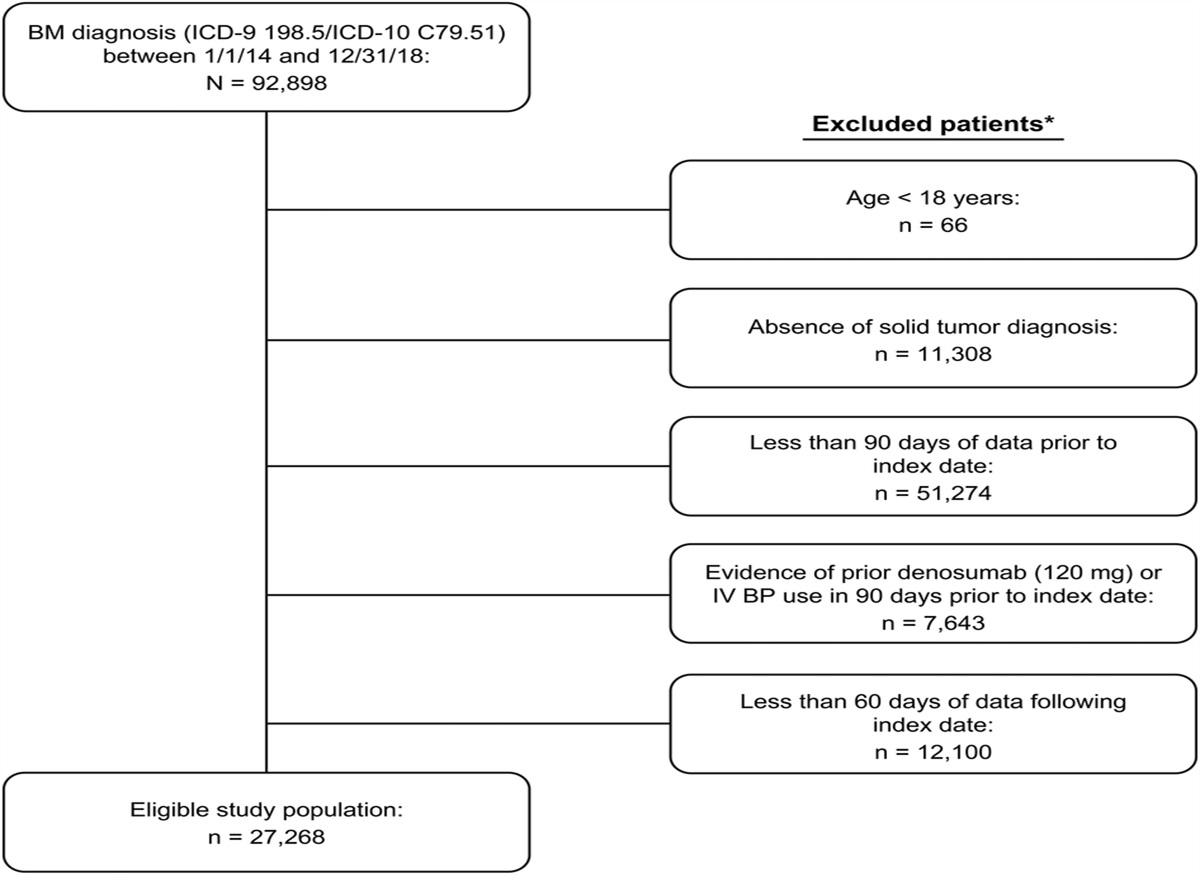
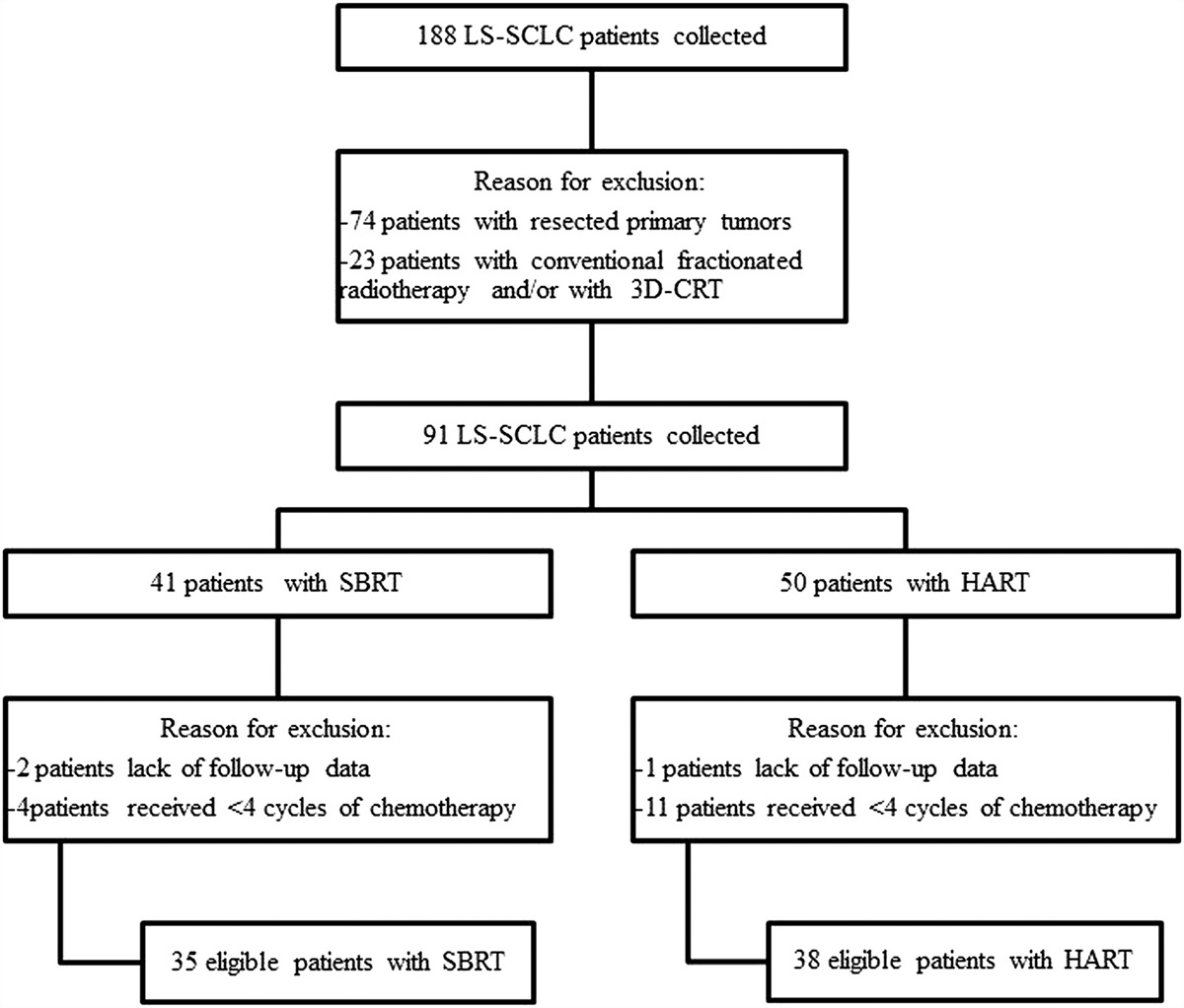
METHODOLOGYThe evidence regarding treatment outcomes was assessed using the Population, Intervention, Comparator, Outcome, and Study design (PICOS) framework. For patients diagnosed with Stage I-III EHCC, we sought to evaluate how surgery, with or without neoadjuvant and/or adjuvant treatments, compared with each other in terms of response, quality of life, or oncologic outcomes through the assessment of data from prospective Phase I-III trials, meta-analyses, and retrospective studies. The trial size required for inclusion was ≥20 patients. The database search strategy is noted in Supplemental File 1 (Supplemental Digital Content 1, https://links.lww.com/AJCO/A438). An extensive analysis of current medical literature covering January 1, 2012 to January 28,2022 from peer-reviewed journals indexed in the Ovid Medline database and using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines yielded a comprehensive set of relevant articles.3 Four authors independently screened the studies to determine those included in this review as detailed in the reference selection flow diagram (Supplemental Fig. 1, Supplemental Digital Content 2, https://links.lww.com/AJCO/A439). Discrepancies between the reviewers were resolved by consensus. A total of 104 articles were identified using the search strategy that met all inclusion criteria. Twenty-three additional studies were included through backward citation searching if they were published before January 1, 2012 and significantly contributed to the literature or if they provided supplemental background information found through PubMed. Study type and quality for these references were assessed through American Radium Society (ARS) Appropriate Use Criteria (AUC) methodology (Supplemental Table 1, Supplemental Digital Content 3, https://links.lww.com/AJCO/A440). The checklist for confirming the completion of essential elements for PRISMA 2020 systematic review may be found in Supplemental Table 2 (Supplemental Digital Content 4, https://links.lww.com/AJCO/A441).
Staging and Work-UpStaging of EHCC is based on the eighth edition of the American Joint Committee on Cancer (AJCC) staging system.4 Perihilar and distal EHCC are staged separately. The initial work-up should include liver function tests. Although optional, tumor markers, such as carcinoembryonic antigen, alpha-fetoprotein, and CA 19-9, may help differentiate EHCC from other primaries and/or for prognostication. Multiphasic computerized tomography (CT) or magnetic resonance imaging (MRI) with intravenous (IV) contrast of the abdomen and pelvis to characterize the primary tumor should be obtained and a CT of the chest to evaluate for metastases. Cholangiography should also be obtained to evaluate the biliary system. Early surgical consultation to assess for resectability and/or transplant is recommended. Biopsy should be obtained in patients who are not candidates for surgery up front.
Management of Malignant Biliary Obstruction (MBO)The goal of treatment for MBO is to relieve obstruction (Tables 1, 2). Preoperative obstructive jaundice is a risk factor for postoperative mortality in patients undergoing major hepatectomy. Endoscopic retrograde cholangiography (ERCP) during initial work-up often identifies a dominant stricture and may be useful as a first therapeutic step.
TABLE 1 - Variant 1: 60 year old female with clinical Stage IIIA, cT2bN2M0 by MRI, hilar cholangiocarcinoma presenting with jaundice, icterus, and hyperbilirubinemia (total bilirubin = 20). Evaluated by surgery and is a candidate for hepatic resection and regional lymphadenectomy. ECOG performance status 1-2. (Case for management of MBO and adjuvant therapy N2) Treatment Rating category Group median rating Disagree SQ SOE SOR Treatment Options Neoadjuvant biliary drainage for MBO A 8 1,3 S ↑ Upfront Surgery without biliary drainage U 3 3 M ↑ Neoadjuvant CT followed by surgery *M 5 X 3,3,2,2 S ↑ Neoadjuvant RT followed by surgery U 3 - EC ↑ Neoadjuvant CRT followed by surgery M 5.5 3,3,2 S ↑ Surgery followed by adjuvant CT alone *M 5 X M,M,2,1 S ↑ Surgery followed by adjuvant RT alone U 3 3,3,3,3 S ↑ Surgery followed by adjuvant CRT M 6 3,3,3,3,3,3,3,3,3,3,3,3 S ↑ If RT: Dose to Tumor/Tumor Bed assuming negative margins 40-45 Gy/20-25 fx M 5 3,3,3,3,3 S ↑ 46-54 Gy /23-30 fx A 8 3,3,2,3,3,3,3,3,3,2,3,3,3 S ↑ 55-60 / 25-33 fx U 3 3,2,3,3,3,3 S ↑ If RT: Dose to Elective nodes 40-45 Gy/20-25 fx A 8 3,2,3,3,3,3,2 S ↑ 46-50.4 Gy /23-28 fx M 5 - EC ↑ If RT: Volumes to be included in Clinical Target Volume Celiac A 8 3,2,3,3,3,3,3,3,2,3 S ↑ SMA A 8 3,2,3,3,3,3,3,3,2,3 S ↑ Porta hepatis (hepatoduodenal ligament and common hepatic) A 8.5 3,2,3,3,3,3,3,3,2,3 S ↑ Pancreaticoduodenal A 8 3,2,3,3,3,3,3,3,2,3 S ↑ Paraaortic A 7 3,2,3,3,3,3,3,3,2,3 S ↑ GTV (Neoadjuvant) or Tumor bed + margin (Adjuvant) A 9 3,2,3,3,3,3,3,3,2,3 S ↑Abbreviations: - indicates neutral; ↑, strong recommendation; ↓, weak recommendation; A, usually Appropriate; CRT, chemo-radiation; CT, chemotherapy; EC, expert consensus; EO, expert opinion; fx, fraction; L, limited; M, May be appropriate; M, meta-analysis; M, moderate; MBO, malignant biliary obstruction; NA, not applicable; RT, radiation therapy; S, strong; SMA, superior mesenteric artery; SOE, strength of evidence; SOR, strength of the recommendation; SQ, refers to the study quality (1, 2, 3, or 4) of the references listed; U, Usually not appropriate.
*Disagree: The variation of the individual ratings from the median rating indicates panel disagreement on the final recommendation.
Variant Discussion:
The optimal method of preoperative biliary decompression (endoscopic nasobiliary, endoscopic with stent placement or percutaneous transhepatic) in patients with ECC who present with obstructive jaundice is variable depending on institutional preference. Although the optimal preoperative bilirubin level is a matter of debate, the shortest possible duration of perioperative biliary drainage is recommended. For those patients who are recommended to undergo neoadjuvant therapy, perioperative biliary drainage is strongly recommended. In patients undergoing neoadjuvant therapy, additional measures to maintain biliary patency after drainage (ie stent placement) may be useful. Typically radioactive stent placement, intraluminal brachytherapy, PDT and RFA in addition to biliary drainage to maintain biliary patency are reserved for inoperable ECCs.
Dose to Tumor/Tumor bed may depend of final pathology. Preoperative radiation doses are typically 45 – 50 Gy, sometimes with doses as high as 60 Gy delivered to areas at risk for positive margin using intensity modulated radiation therapy with simultaneous integrated boost technique. Postoperative radiation doses are typically prescribed at 40 – 45 Gy with boost to 50 – 54 Gy for R0 resections and 55 – 59.4 Gy for R1 resections. Available data most strongly support elective node dose of 40 – 45 Gy but it is not unreasonable to consider doses up to 50.4 Gy to control microscopic disease as the panel feels 40 Gy is somewhat low (expert consensus).
Abbreviations: - indicates neutral; ↑, strong recommendation; ↓, weak recommendation; A, usually Appropriate; CRT, chemo-radiation; CT, chemotherapy; EC, expert consensus; EO, expert opinion; fx, fraction; L, limited; M, May be appropriate; M, meta-analysis; M, moderate; MBO, malignant biliary obstruction; NA, not applicable; RT, radiation therapy; S, strong; SMA, superior mesenteric artery; SOE, strength of evidence; SOR, strength of the recommendation; SQ, refers to the study quality (1, 2, 3, or 4) of the references listed; U, Usually not appropriate.
*Disagree: The variation of the individual ratings from the median rating indicates panel disagreement on the final recommendation.
Variant Discussion:
The optimal method of biliary decompression (endoscopic nasobiliary, endoscopic with stent placement, or percutaneous transhepatic) in patients with ECC who present with obstructive jaundice is variable depending on institutional preference. Additional measures to maintain biliary patency after drainage such as stent or radioactive stent placement, intraluminal brachytherapy, PDT and RFA in addition to biliary drainage are typically reserved for inoperable ECCs.
More aggressive therapy would likely be recommended in patients with good performance status but in patients with poor performance status best supportive care or palliative local therapy may be considered.
SBRT may not be a viable treatment option for lymph node positive ECC unless the lymph node is adjacent to the primary tumor and bowel doses are not limiting. In addition, SBRT total dose would be dependent on ability to meet normal tissue tolerances. Elective nodes would not be included in SBRT target volumes. Hypofractionated radiotherapy may be considered for node positive ECCs that are not candidates for SBRT.
Available data most strongly support elective node dose of 40 – 45 Gy but it is not unreasonable to consider doses up to 50.4 Gy to control microscopic disease as the panel feels 40 Gy is somewhat low (expert consensus).
Drainage can be achieved through a percutaneous or endoscopic nasobiliary approach, or through endoscopic biliary stent placement. Percutaneous biliary drainage is indicated for inoperable patients when endoscopic stent placement is not feasible, although a multi-institutional randomized phase II trial demonstrated increased mortality with this approach compared with endoscopic drainage.5 The optimal method remains unclear due to a lack of randomized data.6
Several types of stents are available. Covered stents can prevent tumor ingrowth and reduce stent failure rates but are thought to have a higher probability of migration.7 Uncovered self-expanding metal stents provide a palliative option. Prospective data demonstrate improved duration of stent patency and lower cholangitis rates when using metal versus plastic stents.8 Data suggest decreased stent occlusion and tumor ingrowth using covered stents compared with uncovered stents.9 The type of stent remains at the discretion of the interventionist.
Another method of preventing tumor overgrowth after stenting is with RT. Studies comparing biliary stents with or without implantation of 125I seeds demonstrate longer stent patency, decreased rates of restenosis, and longer survival times, without differences in complication rates.10–13 Radiation using 192Ir high dose rate (HDR) intraluminal brachytherapy (HDR ILBT) delivered after endoscopic placement of a catheter at the site of obstruction can also be used. Studies evaluating the efficacy of HDR ILBT demonstrate longer stent patency and improved overall survival (OS) compared with stent alone.14–17 External beam RT following stent placement can improve stent patency compared with stent alone,18 and retrospective data suggest that this approach results in improved local control and OS.19
Photodynamic therapy (PDT), using light activation during endoscopy, or intraluminal radiofrequency ablation (RFA), has also been used alone or in combination with other therapies to treat the tumor and increase stent patency duration. Patients receiving PDT have been shown to have improved biliary drainage, quality of life, performance scores, and possibly OS.20–25 Nonrandomized case-controlled26 and randomized27 studies demonstrate the efficacy of RFA in improving stent patency times.
Lastly, stent placement with hepatic arterial infusion (HAI) alone or combined with other therapies can be considered. Retrospective studies have shown improved OS when combining HAI with systemic chemotherapy or RT compared with either modality alone.28–31 A large multicenter retrospective study compared outcomes for stent placement with HAI and RFA versus stent alone and demonstrated longer median stent patency and survival times for the combination group versus the control group, without differences in adverse events between the 2 groups.32
In summary, treatment of MBO is typically performed using endoscopic or percutaneous drainage, usually with stent placement. Data suggests that additional therapies used in combination with stents may prolong stent patency time and survival. The decision of when or how to achieve biliary decompression depends on the location of the obstruction and the patient condition.
SurgeryDistal cholangiocarcinomas have higher rates of resectability as compared with perihilar cholangiocarcinomas. Surgical resection of distal cholangiocarcinoma usually entails a pancreaticoduodenectomy, and surgical principles are similar to the management of pancreatic head adenocarcinoma. In the absence of metastatic disease or vascular involvement, the majority of distal cholangiocarcinomas are resectable with pancreaticoduodenectomy. In general, neoadjuvant therapy should be considered in patients who may require portal vein resection with reconstruction.
Operative resection of perihilar cholangiocarcinoma is more challenging with higher rates of unresectability and usually requires formal hepatectomy or extended hepatectomy with biliary reconstruction. Classification systems are used to provide information about perihilar cholangiocarcinoma local resectability.33 The primary principle determining resectability is the need for biliary reconstruction and maintaining adequate hepatic parenchyma in the remnant liver. Patients with tumor extending into bilateral segmental ducts without a target for restoring biliary continuity are unresectable. Similarly, contralateral portal vein involvement and/or lobar atrophy of anticipated remnant liver is considered unresectable. Therefore, evaluation includes the patient’s functional status and the technical resectability of the tumor and the volume and function of the future liver remnant. A liver remnant volume of >25% is sufficient in a healthy liver; however, >30% to 40% is recommended in the setting of chronic cholestasis, steatosis, cirrhosis, or chemotherapy-induced liver toxicity.
Patients with a small future liver remnant volume should be considered for portal venous embolization before curative intent resection.34 Portal vein embolization occludes the portal vein to the side of the liver that is being resected and causes resultant hypertrophy of the future liver remnant. Contralateral lobar hypertrophy occurs over 2 to 3 weeks, and the kinetic growth rate of the future liver remnant is measured. A post-PVE kinetic growth rate of >2% per week has been shown to correlate with decreased rates of hepatic insufficiency and short-term liver-specific mortality.35
OLT has been employed for patients with perihilar cholangiocarcinoma. Compared with resection for patients with small node-negative tumors, OLT is associated with a 33% increase in 5-year OS rates.36 Typically, transplant candidates are surgically unresectable for reasons of either anatomic invasion or underlying patient disease (commonly primary sclerosing cholangitis). However, OLT is limited by an inadequate supply of liver allografts to satisfy the patient's need. Currently, access to deceased donor liver grafts is limited to patients who meet strict criteria defined by the United Network for Organ Sharing. Patients initially presenting outside of these criteria have significantly worse survival.37 Living donor liver transplantation can be performed more liberally and is determined by the institutional protocol.38 Patients with EHCC with nodal involvement or distant metastatic disease are not considered transplant candidates. To maintain transplant eligibility, patients must undergo neoadjuvant therapy. Survival rates differ among patients who develop cancers in the setting of primary sclerosing cholangitis (5-y OS 74%) and patients who develop de novo cholangiocarcinoma (5-y OS 58%).39 Likewise, patients with no evidence of active disease on post-transplant specimen evaluation have improved survival.
In summary, surgery is the mainstay of treatment for resectable EHCC. Resectability is primarily determined by the need for biliary reconstruction and maintaining an adequate remnant liver. Neoadjuvant therapies may be indicated. Patients with the anatomically unresectable disease should be considered for OLT following neoadjuvant therapy.
Neoadjuvant TherapyWhile surgical resection is the only cure for EHCC, most patients present with advanced disease that precludes upfront resection.40 There is a paucity of data regarding the benefit of neoadjuvant chemotherapy. Nonetheless, such approaches have yielded a downstaging effect that can lead to surgical resection in some patients (Table 3). Single institution retrospective studies have demonstrated improved rates of resectability when patients with upfront unresectable or borderline resectable disease undergo neoadjuvant chemotherapy, with improved OS in resected versus unresected patients.41,42 Neoadjuvant chemotherapy not only improves resectability but also results in an increased rate of R0 resection, which is an independent prognostic marker for long-term survival.43 In a single arm Phase II trial by Matsuyama, 60 patients with borderline resectable perihilar cholangiocarcinoma received Gemcitabine/S1 for 3 cycles every 21 days followed by surgery. Resection with curative intent was performed in 43 of 60 patients (72%), and among those, R0 resection was achieved in 81%. OS was 55.8 months in resected group versus 36.4 months in the unresectable group.44
TABLE 3 - Variant 3: 72 year old male with clinical Stage IIA, 3.5cm hilar cholangiocarcinoma with prominent hilar adenopathy by MRI, encasing the right portal vein, left hepatic duct uninvolved. Non- metastatic. Good performance status, normal liver function. (Technically resectable disease but with hilar adenopathy) Treatment Rating category Group median rating Disagree SQ SOE SOR Treatment Options Surgery Alone U 3 - EC ↑ Neoadjuvant CT followed by surgery A 7 3,3,2,2 S ↑ Neoadjuvant RT followed by surgery M 4 - EC ↑ Neoadjuvant CRT followed by surgery A 7.5 3,3,2 S ↑ Surgery followed by adjuvant CT alone *M 5 X M,M,2,1 S ↑ Surgery followed by adjuvant RT alone U 3 3,3,3,3 S ↑ Surgery followed by adjuvant CRT *M 5 X 3,3,3,3,3,3,3,3,3,3,3,3 S ↑ Definitive CRT M 4.5 3,3,3,3 S ↑ If RT: Dose to Tumor/Tumor bed 45 -60 Gy/25 -33 fx A 8 3,3,2,3,3,3,3,3,3,3,2,3,3,3,3 S ↑ 45-67.5 Gy/ 15 fx A 7 3 M ↑ If RT: Dose to Elective nodes 40-45 Gy/20-25 fx A 8 3,2,3,3,3,3,2 S ↑ 46-50.4 Gy /23-28 fx M 5 - EC ↑ If RT: Volumes to be included in Clinical Target Volume Celiac A 8 3,2,3,3,3,3,3,3,2,3 S ↑ SMA A 8 3,2,3,3,3,3,3,3,2,3 S ↑ Porta hepatis (hepatoduodenal ligament and common hepatic) A 8 3,2,3,3,3,3,3,3,2,3 S ↑ Pancreaticoduodenal A 8 3,2,3,3,3,3,3,3,2,3 S ↑ Para-aortic M 5 3,2,3,3,3,3,3,3,2,3 S ↑ Tumor + margin A 9 3,2,3,3,3,3,3,3,2,3 S ↑Abbreviations: - indicates neutral; ↑, strong recommendation; ↓, weak recommendation; A, usually Appropriate; CRT, chemo-radiation; CT, chemotherapy; EC, expert consensus; EO, expert opinion; fx, fraction; L, limited; M, May be appropriate; M, meta-analysis; M, moderate; MBO, malignant biliary obstruction; NA, not applicable; RT, radiation therapy; S, strong; SMA, superior mesenteric artery; SOE, strength of evidence; SOR, strength of the recommendation; SQ, refers to the study quality (1, 2, 3, or 4) of the references listed; U, Usually not appropriate.
*Disagree: The variation of the individual ratings from the median rating indicates panel disagreement on the final recommendation.
Variant Discussion:
Dose to Tumor/Tumor bed may depend of final pathology. Preoperative radiation doses are typically 45 – 50 Gy, sometimes with simultaneous integrated boost doses as high as 60 Gy delivered to areas at risk for positive margin using intensity modulated radiation therapy with simultaneous integrated boost technique. Postoperative radiation doses are typically prescribed at 40 – 45 Gy with boost to 50 – 54 Gy for R0 resections and 55 – 59.4 Gy for R1 resections. Hypofractionation may also be considered as preoperative or definitive treatment. Available data most strongly support elective node dose of 40 – 45 Gy but it is not unreasonable to consider doses up to 50.4 Gy to control microscopic disease as the panel feels 40 Gy is somewhat low (expert consensus).
If first echelon lymph nodes are positive consider covering second echelon nodes. Common nodal sites of recurrence for distal ECCs are pancreaticoduodenal, porta hepatis, celiac and SMA.
Limited data suggest that neoadjuvant CRT may also improve locoregional control and survival by helping to facilitate margin-negative resection (R0), clearance of microscopic locoregional disease spread, and selecting optimal surgical candidates.45–47 Jung reported a multi-institutional retrospective series of 57 patients with perihilar cholangiocarcinoma comparing up-front surgery (n=45) versus neoadjuvant CRT (n=12) 45 to 50.4 Gy with concurrent 5-FU or gemcitabine.45 The neoadjuvant CRT group had higher rates of R0 resection (83% vs. 67%) and lower rates of pathologic lymph node involvement (25% vs. 56%), without increased risk of postoperative complications. A prospective phase 1 trial of 25 patients
留言 (0)