
記住我




We followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-analyses 2020 statement [17]. Additionally, we registered our protocol with the University Hospital Medical Information Network Clinical Trials Registration as UMIN000048111 (http://www.umin.ac.jp/ctr/index.htm [accessed on June 20, 2022]).
Eligibility criteriaOnly studies that reported functional results and complications of megaprosthetic reconstruction of the distal femur with a short residual proximal femur following bone tumor resection were included. A residual short proximal femur was defined as < 12 cm in length, where the standard modular-type megaprosthesis stem could not be inserted. Studies in which reconstruction was performed in patients without short residual proximal femurs were excluded. Studies that performed reconstruction in patients with short residual proximal femurs, but did not specify both functional results and complications, were also excluded. Only English- and Japanese-language literatures were included, with no restrictions on publication year.
Literature search and study selectionThe literature was searched according to a systematic search strategy using the Medline, Embase, and Cochrane Central Register of Controlled Trials databases on May 31, 2022 (Additional file 1). Additionally, the bibliographies of the retrieved literature were used to identify other relevant studies.
Data collection and presentationThe studies were independently selected, and data were extracted. In case of disagreement, an agreement was reached among the authors. The following data were collected using a data collection sheet: (1) Basic data (author name, year of publication, journal name, type of study, period investigated, number of patients, patient age, and tumor histology); (2) Surgical indication, method of reconstruction, cement fixation, porous coating, time to full weight bearing, stem length of prosthesis, adjuvant chemotherapy, adjuvant radiotherapy, non-union, aseptic loosening, implant breakage, fracture, infection, mechanical survival (where the endpoint was set to implant removal for any reason), oncological outcome, Musculoskeletal Tumor Society (MSTS) score [18], and postoperative follow-up period.
Data summaryTables 1 and 2 summarize the data extracted from the collected data. Table 3 summarizes the time to full weight-bearing, non-union, aseptic loosening, implant breakage, fracture, infection, mechanical survival, MSTS score [18], and postoperative follow-up period for each reconstruction method (custom-made megaprosthesis, APC, and CPS implant). All studies included in this review were non-randomized; therefore, data pooling (meta-analysis) was not appropriate and thus, not performed.
Table 1 Overall study characteristicsTable 2 Overall study characteristicsTable 3 Summary of complications and functional outcomes for each reconstruction methodAssessment of methodological qualityThe methodological quality of each study was independently assessed. When there was disagreement, agreement was reached among the authors through discussion. Articles included in the final analysis were independently assessed according to the Risk of Bias Assessment tool for Non-randomized Studies (RoBANS tool) to assess the quality of non-randomized studies in meta-studies [19].
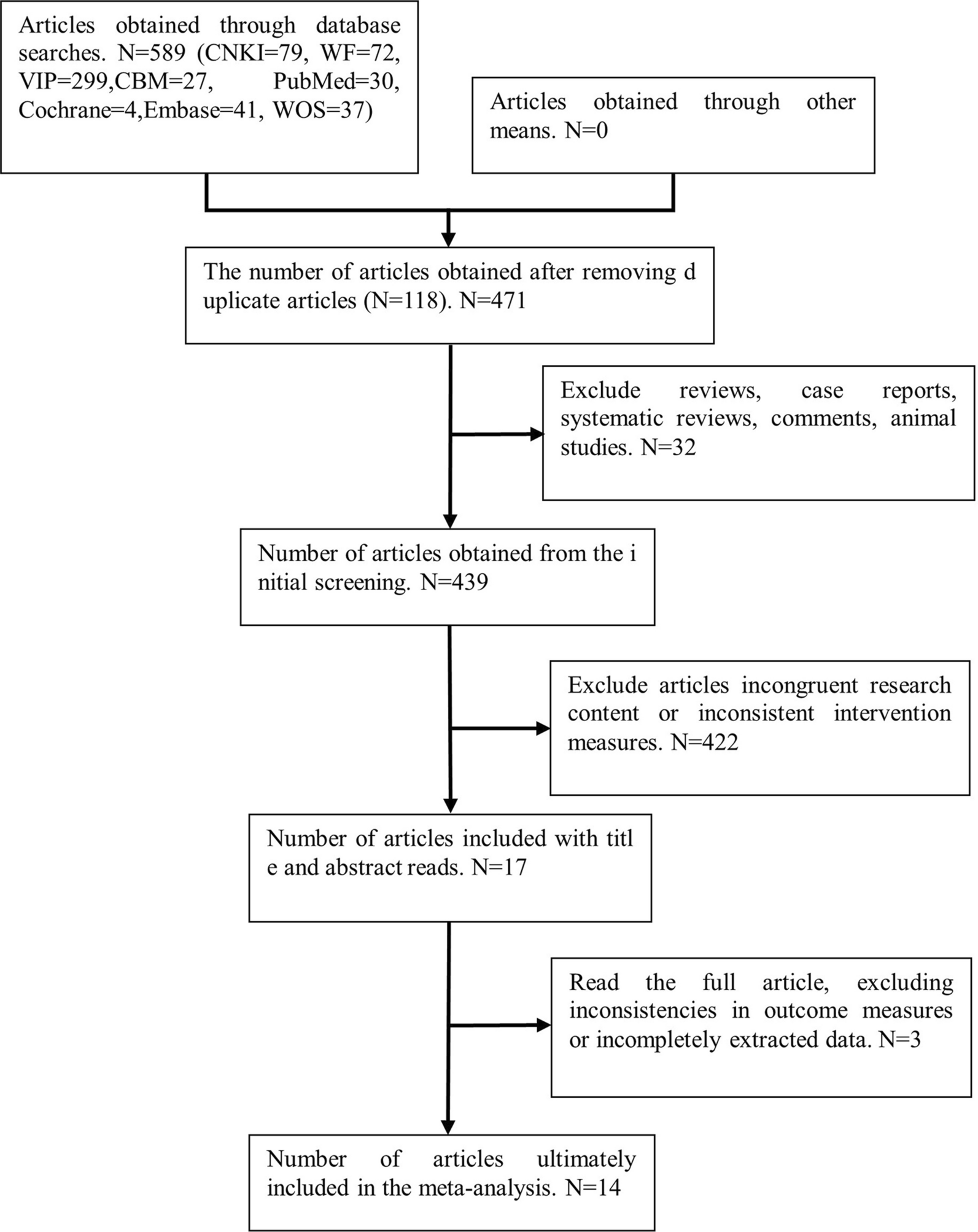
Search resultsOf the 236 studies identified by the search, eight were included in our review (Fig. 3; Tables 1, 2 and 3) [2, 5, 11,12,13,14,15,16]. These eight studies were not RCTs.
Fig. 3
Flow chart of the search for relevant articles
Demographic data and ratio of patients who underwent reconstruction with custom-made megaprostheses, APC, and compression-compliant pre-stress implantA total of 155 patients underwent megaprosthetic reconstruction of their distal femurs with a short residual proximal femur, following bone tumor resection. Of the 155 patients, 106 (68.4%) underwent reconstruction with a custom-made megaprosthesis, 12 (7.7%) with APC, and 37 (23.9%) with CPS implants (Tables 1, 2 and 3). Custom-made megaprostheses were the most commonly used from the 1980s until recently (Table 1). Between 2008 and 2018, at one institution, APC was the only method used to reconstruct the remaining short proximal femur after bone tumor resection of the distal femur [2] (Table 1).
Methodological quality of the included studiesThe quality of each study was assessed using the RoBANS tool; overall, there was a moderate risk of bias. All the eight included studies showed that ‘selection of participants’ and ‘confounding variables’ were high, while ‘measurement of exposure,’ ‘blinding of outcome,’ ‘incomplete outcome data,’ and ‘selective outcome reporting’ were low.
留言 (0)