In this issue of Critical Care Medicine, Bose et al (1) describe the frequency of unmet nonmedication healthcare needs (i.e., durable medical equipment, home health services, outpatient follow-up appointments) after hospital discharge for a cohort of patients admitted with acute respiratory failure. The vast majority of patients (98%) had at least one non medication need, with a median of 5 needs per patient. Unfortunately, 34% of patients had 1 or more needs unmet. For each need category, the authors identified a reasons as to why the needs were unmet, including: durable medical equipment was not delivered or the patient refused it; home health services were not scheduled or COVID restrictions interfered with availability; and follow-up appointments were not scheduled or patients were readmitted to the hospital before their appointment. Although 29% of patients died or were re-admitted to a hospital within 90-days of discharge, the study did not demonstrate an association between this composite endpoint and unmet needs. Despite a lack of statistically significant association, the sheer number of needs for each patient and the proportion of those needs that are unmet adds to the growing literature describing care gaps for ICU survivors.
A focus on ICU survivor care gaps is critical, given emerging research findings about postintensive care syndrome (PICS) since it was defined in 2012. PICS refers to “new or worsening impairments in physical, cognitive, or mental health status arising after critical illness and persisting beyond acute care hospitalization” (2), with the dynamic nature of patient needs across the phases of critical illness increasingly characterized in the literature (3). In 2020, the results of a Society of Critical Care Medicine (SCCM) consensus conference were published describing seven pragmatic recommendations to improve the functional status assessment of patients across the continuum of critical illness and recovery (3). These recommendations included: 1) assess pre-ICU functional abilities upon ICU admission; 2) document functional abilities in history and physical; 3) report pre-ICU and current functional abilities during ICU to floor handoff; 4) conduct pre-discharge functional assessment; 5) reconcile pre-ICU and predischarge abilities to guide post-acute care referrals; 6) screen at-risk patients using recommended tools after discharge; and 7) conduct initial postdischarge screening within 2–4 weeks of hospital discharge.
Three of these seven SCCM recommendations target processes surrounding hospital discharge and outpatient follow-up, with evidence that there are ongoing challenges in these areas (5–7). Failure to effectively transition ICU survivors from inpatient to outpatient settings may contribute to, or at minimum fail to mitigate, morbidities faced by ICU survivors (2,4). Hirshberg et al (8) reported that 43% of ICU survivors were readmitted to a hospital within the first year of hospital discharge and 24% of these readmissions were for a condition for which strong linkage to ambulatory care might have had an impact (e.g., uncontrolled diabetes, heart failure, and urinary tract infections). Although it is unlikely that all hospital re-admissions are preventable and current risk models are imperfect, there is almost certainly significant room to improve in this area (4,9).
Thus far, multiple studies have documented limited success, despite dedicated efforts focused on improving hospital-to-outpatient transitions and decreasing readmissions. For example, transition programs to improve hospital discharge transitions for ICU survivors found little benefit with respect to readmission rates or other relevant outcomes (3,10). In a recent single-center study by Bloom et al (11), a multifaceted ICU recovery program extended the median time to hospital readmission by 2 weeks, but did not significantly decrease the 30-day hospital readmission rate. An important limitation of the study by Bose et al (1) was that although 90% of patients in the intervention arm received at least one inpatient intervention (e.g., an inpatient visit by a transition program nurse practitioner), only 13% of patients received any outpatient intervention (e.g. a case management screen).
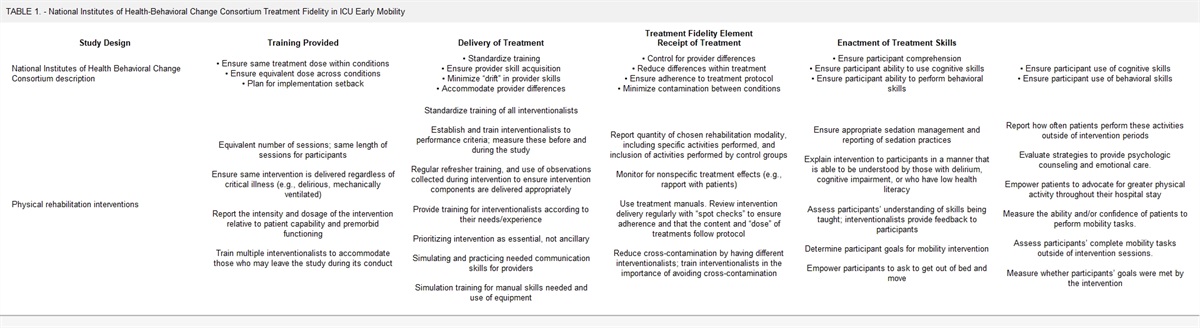
Interventions focused on care transitions and the outpatient setting therefore appear to be an essential next step. Bose et al (1) highlight the volume of outpatient needs typically present post-ICU stay, which was striking given the growing number of ICU survivors. This highlights the need to identify barriers to high quality post-ICU care and to implement targeted corrective actions. Especially with current healthcare staffing challenges, engaging human factors engineering to study care delivery systems may help to characterize the problem and identify potential solutions (12). Human factors engineers can assess the clinician, guideline, and system factors that contribute to gaps in care delivered by a health system (Table 1 for an example human factors tool that may support assessing gaps in supporting ICU survivor needs) (13).
TABLE 1. -
Example Tool to Assess Factors Contributing to Functional Status Assessment Gaps Across the Critical Illness and Recovery Continuum
Contributing Factors and Potential Questionsa
Example Gap
Clinician
Knowledge
What do you know about PICS and the recommendations?
Hospitalists and outpatient clinicians unaware of PICS and recommendations
Attitude
What is your perspective regarding PICS and the recommendations in general?
ICU physicians deemphasize functional conditions and rarely discuss (focusing instead on acute critical patients)
Applicability to patient population
How often do you think the recommendations apply to your patients?
Outpatient clinicians
Guideline
Evidence supporting the guideline
How strongly does evidence support recommendations?
Perceived adherence with guideline
How often are the recommendations followed in your practice?
Ease of adhering to the guideline
How do these recommendations impact workload?
ICU, ward, and clinic perceive guidelines to be cumbersome and unsupported
System
Task
Who is responsible for each aspect of the guideline?
Tools and technologies
Are necessary supplies and equipment available and used appropriately?
No postdischarge follow-up tool
Decision support (e.g., checklists, ordersets, prediction tools)?
How often are aids available and used?
Physical environment
How does the unit’s lay out affect adherence?
Step down unit does not have usable patient/caregiver education space
Organizational structure (e.g., staffing, policies)
How does organizational structure influence adherence?
No inpatient process for telephone patient follow-up after discharge
Administrative support
How does the administration visibly (and substantially) influence recommendation adherence?
Performance monitoring and feedback mechanism?
How does the team know that it is consistently (and appropriately) applying the recommendation?
No feedback system regarding functional ability assessment, posthospital needs, or long-term outcomes.
Unit culture
How does the unit culture influence adherence?
External community environment
How do available community resources influence adherence?
PICS = postintensive care syndrome.
aFor each question, respondents are asked to “Please consider PICS and associated recommendations (i.e., functional ability assessment, approaches to meet needs) across the critical illness and recovery continuum.”
Several barriers particularly relevant to nonmedication needs for ICU survivors may be informed by human factors insights. First, explicit understanding of PICS and the posthospital discharge needs of ICU survivors by the clinical community, including outpatient clinicians, is limited (14). New techniques are needed to engage and educate the broader clinical community to ensure a shared understanding regarding patient needs and the roles of individual clinicians, particularly in ambulatory settings, across the continuum of critical illness and recovery. Furthermore, when developing effective clinician support tools for patients after an ICU stay, such as new workflow designs and decision aids, outpatient perspectives should be incorporated to ensure optimal utility.
Second, we need to increase the tools available to increase patient and caregiver health literacy about PICS and related needs. The SCCM “After the ICU” website (sccm.org/MyICUCare) can serve as an educational model. Human factors approaches can inform the development of these tools to increase patient and caregiver understanding of PICS, associated nonmedication needs, and specific strategies to meet these needs. For example, these tools would benefit from usability assessments to ensure that they can be accessed easily and avoid jargon not understood by the general public.
Third, communication regarding patient functional abilities, both at ICU to floor transition and at patient discharge must be enhanced. The importance of including patient functional assessment in discharge summaries was highlighted in the 2012 consensus conference, but the quality of assessments for ICU survivors and how effectively results are communicated remains relatively understudied (2,3,6,15). Human factors techniques can inform the development of, and response to, these assessments (16)—for example, by ensuring that assessments are structured to identify survivor needs, and by evaluating the process of addressing these needs (e.g., appointment scheduling and coordination of home health support). Incorporating these assessments into handoff tools would be beneficial to ensure a shared understanding of addressed and outstanding needs among clinicians, patients, and their caregivers.
Fourth, timely outpatient follow-up for ICU survivors following hospital discharge should be ensured, as an extended discharge to follow-up appointment intervals may hinder the ability of many patients to have PICS-related concerns addressed and to prevent readmission. The SCCM conference therefore recommended screening at-risk patients using recommended tools and conducting an initial post-discharge screening within 2–4 weeks of hospital discharge (4). However, timely follow-up has historically been a challenge; a Kaiser study found that almost 30% of patients admitted for a heart failure exacerbation were not seen within 30 days despite evidence supporting the importance of early follow-up in that population (17).
Human factors research may inform approaches to structure outpatient care models to more rapidly receive ICU survivors and provide necessary resources. For example, scheduling outpatient (including telehealth visits) may increase outpatient follow-up by decreasing the effort that patients and caregivers must exert to schedule and travel to appointments. Furthermore, community factors (e.g., housing density, availability of nursing home beds, food insecurity) heavily influence hospital readmissions and outpatient care models (18,19). A robust understanding of these local social determinants of health and their effect on ICU survivors, can inform health system and community leader efforts to link patients to appropriate resources.
CONCLUSION
The analysis by Bose et al (1) is a stark reminder of the significant nonmedication needs for ICU survivors and current limitations of our current care models to meet patient needs after hospital discharge. Failure to effectively support ICU survivors exacts a significant cost on our patients and society. Optimal support for ICU survivors across the continuum of critical illness and recovery will likely require a transformative change across our health system built upon multiple incremental changes. Achieving both changes will be bolstered by effectively leveraging the insights of multiple stakeholder and expert resources, including human factors engineers. As we continue to implement incremental changes and consider broader changes, our profession and society should examine how we are investing our resources.
Significant resources have been invested to improve and deliver acute care to critically ill patients with associated improvement in short term outcomes, yet morbidity burden for ICU survivors remains. If our goal as a profession and as a society is merely to ensure that critically ill patients are discharged alive from the ICU or the hospital, then this is sufficient. If, however, our goal is to support optimal patient outcomes beyond the ICU or hospital, then we must diversify our investments to support and improve care models across the entire care continuum.
REFERENCES
1. Bose S, Groat D, Dinglas VD, et al.: Addressing Post-Intensive Care Syndrome (APICS-01) Study Team: Association Between Unmet Nonmedication Needs After Hospital Discharge and Readmission or Death Among Acute Respiratory Failure Survivors: A Multicenter Prospective Cohort Study. Crit Care Med. 2022; 51:212–221
2. Needham DM, Davidson J, Cohen H, et al.: Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit Care Med. 2012; 40:502–509
3. Brown SM, Bose S, Banner-Goodspeed V, et al.; Addressing Post Intensive Care Syndrome 01 (APICS-01) study team: Approaches to addressing post-intensive care syndrome among intensive care unit survivors. A narrative review. Ann Am Thorac Soc. 2019; 16:947–956
4. Mikkelsen ME, Still M, Anderson BJ, et al.: Society of Critical Care Medicine’s international consensus conference on prediction and identification of long-term impairments after critical illness. Crit Care Med. 2020; 48:1670–1679
5. Haines KJ, Sawyer A, McKinnon C, et al.: Society of Critical Care Medicine’s Thrive Initiative: Patient and caregiver-derived health service improvements for better critical care recovery. Crit Care Med. 2022; 50:1778–1787
6. King J, O’Neill B, Ramsay P, et al.: Identifying patients’ support needs following critical illness: A scoping review of the qualitative literature. Crit Care. 2019; 23:187
7. Donaghy E, Salisbury L, Lone NI, et al.: Unplanned early hospital readmission among critical care survivors: A mixed methods study of patients and carers. BMJ Qual Saf. 2018; 27:915–927
8. Hirshberg EL, Wilson EL, Stanfield V, et al.: Impact of critical illness on resource utilization: A comparison of use in the year before and after ICU admission. Crit Care Med. 2019; 47:1497–1504
9. Horwitz LI, Bernheim SM, Ross JS, et al.: Hospital characteristics associated with risk-standardized readmission rates. Med Care. 2017; 55:528–534
10. Schofield-Robinson OJ, Lewis SR, Smith AF, et al.: Follow-up services for improving long-term outcomes in intensive care unit (ICU) survivors. Cochrane Database Syst Rev. 2018; 11:CD012701
11. Bloom SL, Stollings JL, Kirkpatrick O, et al.: Randomized clinical trial of an ICU recovery pilot program for survivors of critical illness. Crit Care Med. 2019; 47:1337–1345
12. Werner NE, Gurses AP, Leff B, et al.: Improving care transitions across healthcare settings through a human factors approach. J Healthc Qual. 2016; 38:328–343
13. Gurses AP, Murphy DJ, Martinez EA, et al.: A practical tool to identify and eliminate barriers to compliance with evidence-based guidelines. Jt Comm J Qual Patient Saf. 2009; 35:526–32, 485
14. Haines KJ, Hibbert E, Leggett N, et al.; Society of Critical Care Medicine’s Thrive Initiative: Transitions of care after critical illness-challenges to recovery and adaptive problem solving. Crit Care Med. 2021; 49:1923–1931
15. Horwitz LI, Jenq GY, Brewster UC, et al.: Comprehensive quality of discharge summaries at an academic medical center. J Hosp Med. 2013; 8:436–443
16. Murphy DJ, Lane-Fall MB: Leveraging robust mixed methodologies to advance implementation research and practice. Crit Care Med. 2022; 50:1159–1161
17. Lee KK, Yang J, Hernandez AF, et al.: Post-discharge follow-up characteristics associated with 30-day readmission after heart failure hospitalization. Med Care. 2016; 54:365–372
18. Spatz ES, Bernheim SM, Horwitz LI, et al.: Community factors and hospital wide readmission rates: Does context matter? PLoS One. 2020; 15:e0240222
19. Soto GJ, Martin GS, Gong ML: Healthcare disparities in critical illness. Crit Care Med. 2013; 41:2784–2793

留言 (0)