A systematic literature review was performed by searching databases, including PubMed, ScienceDirect, Web of Science, and SCOPUS, using the terms “SCA34” or “ELOVL4 ataxia”. Publications with English abstracts describing cases with an identified ELOVL4 variant were included.
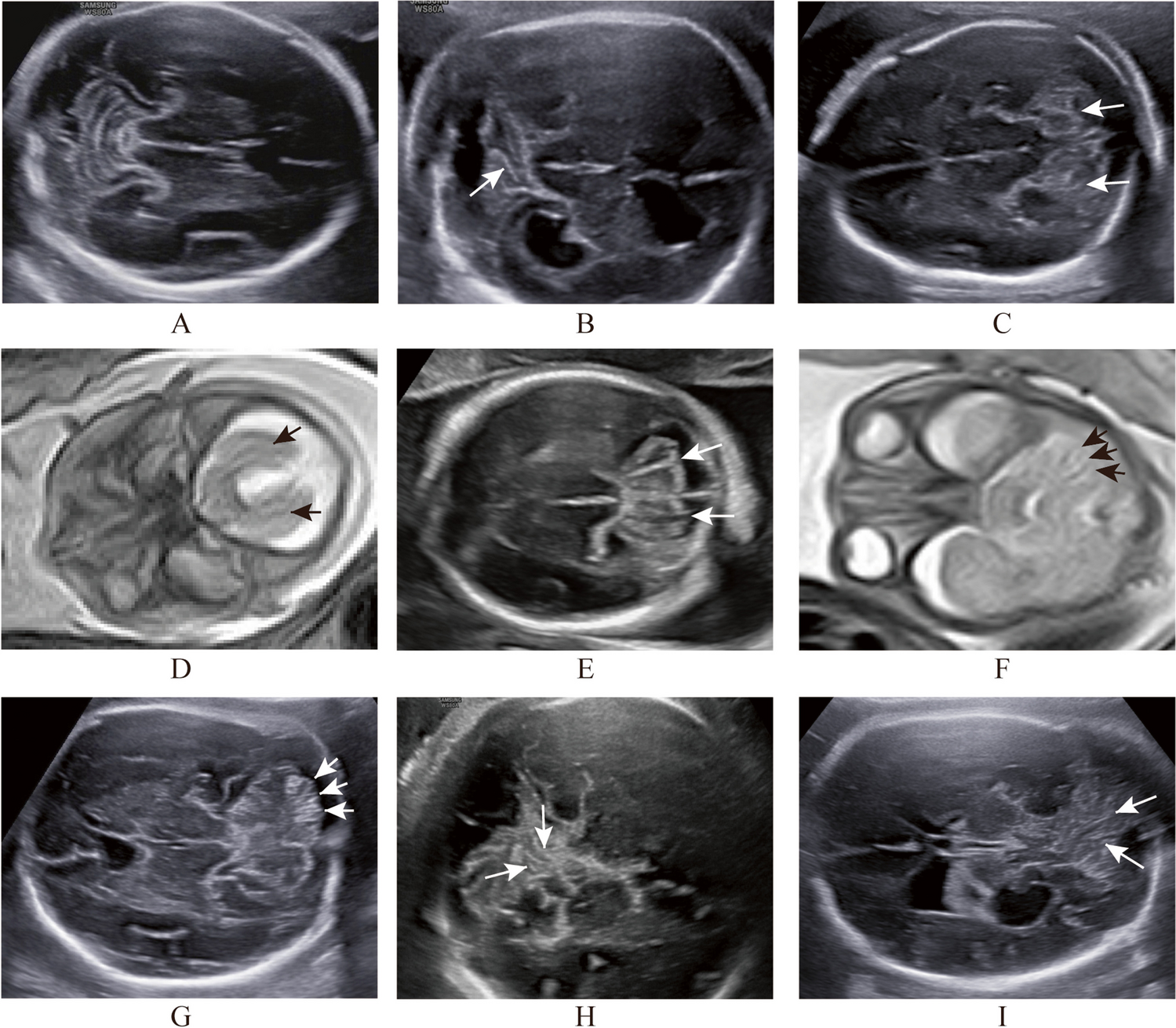
In total, we identified 60 reported cases of SCA34 (Tables 2 and 3). The estimated mean age of onset was 31.85 (± 12.76) years (mean ± SD). Most cases had cerebellar ataxic features including gait ataxia (88.3%), limb ataxia (76.7%), dysarthria (63.3%), and nystagmus (58.3%). On brain MRI, cerebellar atrophy was reported in all cases (100%), and the hot cross bun sign, usually associated with multiple system atrophy cerebellar type, was seen in 32.4% of cases (Table 4).
Table 2 Clinical findings according to variant in reported cases of ATX-ELOVL4Table 3 Summary of extracerebellar clinical findings in reported cases of ATX-ELOVL4Table 4 Summary of brain MRI finding in reported cases of ATX-ELOVL4Importantly, EK-related skin lesions were only seen in a minority of cases (33.3%), which is in contrary to the reported prototypic manifestation of SCA34/ATX-ELOVL4 (OMIM #133190). Whilst the majority of cases with EK skin lesions had EKV [3], several cases had lesions more consistent with progressive symmetric erythrokeratoderma (PSEK) rather than EKV [10, 12]. Of note, one study reported a 16-year-old boy with PSEK skin lesions with no neurological or cerebellar clinical signs who was found to have the c.698C > T ELOVL4 variant [12]. This case highlights the potential clinical phenotypic variability for ELOVL4-associated disease, though it is plausible that this individual develops ataxia later in his life. Similarly, the aforementioned large French-Canadian family study also reported three variant carriers who displayed EKV but no ataxia which may be attributed to their younger ages [3]. Additionally, some cases demonstrated skin lesions unrelated to EK, such as ichthyosis [13] and nummular dermatitis [4], and thus were not included in the calculation of the prevalence of EK-related skin lesions (Tables 2 and 3). Interestingly, there were a total of five reported SCA34 cases with the c.698C > T variant in ELOVL4, and four of them exhibited EK skin lesions [6, 9, 10] in contrast to the present study where the four individuals did not exhibit EK-related skin lesions despite having the exact same nucleotide variant. This finding supports inter-familial phenotypic variability and points against a clear genotype–phenotype correlation. It may also suggest that additional factors, such as environmental and genetic modifiers, may affect the dermatological manifestation of ELOVL4-related disease.
In terms of other extracerebellar manifestations, pyramidal tract signs, such as DTRs abnormalities or abnormal plantar reflexes, were found in 48.3% of the cases. Autonomic disturbances, cognitive impairment, and ophthalmologic pathologies were found in 11.7%, 11.7%, and 8.3% of reported cases, respectively; however, these values may not be accurate considering the relatively small number of reports on these phenotypic manifestations. However, it should be noted that one study reported retinitis pigmentosa in four out of eight affected members in a family with c.512 T > C p.(Ile171Thr) variant [5], and another study described cognitive impairment and psychiatric symptoms in five affected members of the studied family which were characterised by c.504G > C p.(Leu168Phe) variant [4].

留言 (0)