
記住我










Humoral immune response after COVID-19 vaccination can be impaired in patients with immune-mediated inflammatory diseases (IMIDs).
A third vaccination is safe and efficient in healthy individuals.
WHAT THIS STUDY ADDSA third vaccination is safe and immunogenic in patients with IMIDs.
Reduced anti-receptor-binding domain and neutralising antibody levels were observed in patients with IMIDs treated with biological disease-modifying anti-rheumatic drugs and combination therapy as compared with healthy controls.
Cellular immune response is enhanced in patients with IMIDs after a third vaccination.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICYIntroductionThe SARS-CoV-2 pandemic poses an unprecedented challenge to the general population and in particular to patients with immune-mediated inflammatory diseases (IMIDs). The risk of developing severe forms of COVID-19 may be increased in patients with IMIDs, likely due to higher frequency of comorbidities as well as the use of immunosuppressive therapies especially glucocorticoids and rituximab among these patients, while data for Janus kinase inhibitors remain disputed.1–6 Furthermore, impaired humoral immune responses to a primary COVID-19 vaccination have been documented in these patients.7–18
Following the guidelines of the Centers for Disease Control and Prevention (CDC), the American College of Rheumatology (ACR) recommends a third vaccination for immunocompromised individuals who are not expected to mount an adequate vaccine response.19 Limited information on the effects of a third vaccination have been highlighted in the most recent EULAR recommendations.20 While currently available data support safety and immunogenicity of a third dose in healthy individuals, solid organ transplant recipients and patients with hemato-oncological malignancies, data on patients with IMIDs with low antibody titers after primary vaccination are still sparse.21–37 Promising results have been reported in patients with rheumatic diseases after a third vaccination with an inactivated SARS-CoV-2 vaccine.25 Recent studies provided further evidence for the efficacy of a third vaccination in patients with IMIDs.38 39 However, clinical trials that address safety and immunogenicity in immunosuppressed patients with IMIDs are currently missing. We have therefore performed a clinical trial comparing safety and immunogenicity of a third vaccination in patients with IMIDs as compared with healthy controls (HCs).
MethodsTrial design and participantsIn this prospective open-label clinical trial, adults (age>18 years) with a diagnosis of an IMIDs and HCs, both with anti-receptor-binding domain (anti-RBD) antibody levels<1500 BAU/mL (binding antibody units per millilitre) after primary COVID-19 vaccination, were enrolled to receive a third vaccination. The cut-off was selected based on previously published data on the antibody response to primary COVID-19 vaccination in healthy individuals.40 41 All participants have received two doses of an mRNA vaccine with either BNT162b2 or mRNA-1273 for primary immunisation. The third dose was administered at least 4 weeks after the second dose. Major exclusion criteria were known allergies to vaccines and previous SARS-CoV-2 infection. Patients needed to be under immunosuppressive treatment during the past 12 months; however, those receiving B-cell-depleting therapies, such as rituximab, as well as those with primary immunodeficiency were excluded. HCs without immunosuppressive therapy were recruited from the Vienna General Hospital. Detailed information on the trial design can be found in the study protocol. The trial was registered in the European Clinical Trials Database (EudraCT No: 2021-002693-10) on 15 July 2021.
InterventionsFive trial visits were performed. At the screening visit, patient eligibility was confirmed. Patients and participants with anti-RBD antibody levels below 1500 BAU/mL were vaccinated open label at visit 2 (week 0) within 28 days of screening, using either BNT162b2 (30 µg dose) or mRNA-1273 (100 µg dose). The cellular immune response was assessed at week 1 and the humoral immune response at week 4. Serum samples were stored below −70°C at the Biobank of the Medical University of Vienna, a centralised facility for the preparation and storage of biomaterial with certified quality management (International Organization for Standardization (ISO) 9001:2015).42 Peripheral blood mononuclear cells (PBMCs) were isolated at screening and 1 week after the third vaccination by density gradient centrifugation and stored in the vapour phase of liquid nitrogen until further use. A patient diary was used to gather safety data for the first week after vaccination, adverse events were assessed until week 4. Symptom intensity was rated between 0 (no symptom) and 3. In total, 1 patient did not return the diary, leaving 47 HCs and 55 patients for consecutive analysis.
All trial visits were conducted in a single centre (Vienna General Hospital). The first participant was enrolled on 28 September 2021 and the last completed the 4-week follow-up on 22 December 2021.
Characterisation of peripheral lymphocytesDetermination of lymphocyte subsets was performed as described previously10: In brief, flow cytometry (FACSCanto II, Becton Dickinson, San Jose, California, USA) was used to determine immunological phenotypes of lymphocyte subsets. Hereby, the whole blood staining was done prior to erythrocyte lysis (Becton Dickinson). A combination of the following monoclonal antibodies (all provided by Becton Dickinson) was applied: fluorescein isothiocyanate (FITC)-labelled anti-CD3, phycoerythrin (PE)-labelled anti-CD16+56+, peridinin-chlorophyll-protein-cy5.5-labelled anti-CD4, PE-Cy7-labelled anti-CD19, allophycocyanin (APC)-Cy7-labelled anti-CD8, V450-labelled anti-human leucocyte antigen-DR, V500-labelled anti-CD45 and APC-labelled anti-CD14.
Anti-SARS-CoV-2 antibody testingQuantitative assessment of antibodies to the receptor-binding domain (RBD) of the viral spike (S) protein was performed by an Elecsys Anti-SARS-CoV-2 S immunoassay as previously described,43 44 with a detection range between 0.4 and 2500.0 BAU/mL. A concentration greater than 0.8 BAU/mL was considered positive. Concentrations>2500 BAU/mL were approximated by manual predilutions up to a value of 750 000 BAU/mL. Analysis was performed on a Cobas e801 (Roche Diagnostics, Rotkreuz, Switzerland) at the department of laboratory medicine, Medical University of Vienna (certified acc. to ISO 9001:2015 and accredited acc. to ISO 15189:2012).
SARS-CoV-2 neutralisation test (NT)The NT against the wild type (WT) virus and the Omicron BA.2 variant was performed as described previously.45–47 Twofold serial dilutions of heat-inactivated serum samples were incubated with 50–100 TCID50 SARS-CoV-2 for 1 hour at 37°C before the mixture was added to Vero E6 (ATCC CRL-1586) cell monolayers. Incubation was continued for 3–5 days. NT titers were expressed as the reciprocal of the serum dilution required for protection against virus-induced cytopathic effects. NT titers≥10 were considered positive and samples that failed for technical reasons were excluded from the analysis.
T-cell responsesFor T-cell stimulation (see below), PepMix SARS-CoV-2 peptide pools for WT and Omicron were acquired from JPT (Berlin, Germany). Peptides were dissolved in dimethyl sulfoxide and diluted in AIM-V medium for use in enzyme-linked immunosorbent spot (ELISpot) assays as described previously.48
For ex vivo T-cell interferon (IFN)-γ ELISpot assay, PBMCs from patients before and after the third vaccination were thawed and processed on the same day. A total of 1–2×105 cells per well were incubated with SARS-CoV-2 peptides (2 µg/mL; duplicates), AIM-V medium (negative control; 3–4 wells) or phytohemagglutinin (PHA) (L4144, Sigma; 0.5 µg/mL; positive control) in 96-well plates coated with 1.5 µg anti-IFN-γ (1-D1K, Mabtech) for 24 hours. After washing, spots were developed with 0.1 µg biotin-conjugated anti-IFN-γ (7-B6-1, Mabtech), streptavidin-coupled alkaline phosphatase (Mabtech, 1:1000) and 5-bromo-4-chloro-3-indolyl phosphate/nitro blue tetrazolium (Sigma). Spots were counted using a Bio-Sys Bioreader 5000 Pro-S/BR177 and Bioreader software generation 10. Data were calculated as spot-forming cells (SFCs) per 106 PBMCs after subtracting the spots from the negative control (mean spot numbers from three to four unstimulated wells).
Outcomes and sample sizePrimary endpoint was the comparison of response rate (defined as anti-RBD antibody levels>1500 BAU/mL) between patients with IMIDs and HCs. Secondary outcomes included the difference in anti-RBD antibody level change between patients with IMIDs and HCs at week 4, the effects of immunosuppression and patient characteristics on antibody levels at week 4 and cellular immune responses 1 week after the third vaccination. Assessment of safety included incidence and severity of adverse events over 28 days. A paper-based diary was used to evaluate reactogenicity. Assuming an estimated vaccination response rate of 70%, we planned to include a total of 65 patients and 65 HCs. This number would have allowed us to achieve at least 80% power to test the primary endpoint, based on non-inferiority (allowing a non-inferiority limit of a maximum of 20%).
Statistical analysisData analysis was performed in R V.4.1.2 (R Development Core Team, Vienna, Austria) with the use of the following packages: ‘tidyverse’, ‘ggpubr’ and ‘tableone’. For primary endpoint, a χ2 test was used to assess different rate of vaccine responders (anti-RDB-antibody level>1500 BAU/mL at week 4) between patients with IMIDs and HCs. Secondary endpoints were defined either as absolute levels or changes (absolute and fold change) between week 0 and week 4. Normality was tested by Shapiro-Wilk normality test and non-parametric tests were used according to the distribution of the data. Anti-RBD antibodies, NT titers and T-cell data were compared using Wilcoxon signed-rank test or Spearman’s rank correlation coefficient for numerical assessment of correlations. All subjects vaccinated with a third dose who completed week 4 were included in the analysis. Post-hoc exploratory analysis to assess cellular immune responses between week 0 and week 1 was performed using paired Wilcoxon test. For intergroup comparison a two-sided Wilcoxon test was used.
Patient and public involvementPatients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
ResultsPatient characteristicsIn total, 90 patients from our outpatient clinic and 53 HCs who had been immunised with 2 doses of an mRNA vaccine were screened for eligibility. Overall, 30 patients were excluded: 7 patients withdrew informed consent, 6 failed screening criteria and 1 patient was excluded due to pregnancy, 16 were excluded due to primary immunodeficiency. Five HCs were excluded: two withdrew informed consent and three failed screening criteria. In total, 108 individuals were vaccinated with an mRNA-based vaccine. After vaccination, one HC was excluded due to a newly acquired SARS-CoV-2 infection. In total, 60 patients and 47 HCs returned at week 1 and subsequently 3 patients were lost to follow-up and 1 patient was excluded due to SARS-CoV-2 infection. Thus, a total of 56 patients and 47 HCs presented at follow-up visits and completed the trial at week 4 after vaccination (figure 1). Patient and HCs characteristics are presented in table 1. Disease entities in the patient cohort consisted of inflammatory arthritis (44.6%), connective tissue diseases (33.9%), vasculitis (14.3%) and other patients receiving immunosuppressive therapy (7.1%) (online supplemental table 1).
 Figure 1
Figure 1 Screening, vaccination and follow-up of patients. FU, follow-up.
Table 1Characteristics of patients and healthy control subjects who completed week 4
Humoral immune responseAntibodies against the SARS-CoV-2 RBD of the spike (S) protein were analysed before and 4 weeks after the third dose of either BNT162b2 or mRNA-1273 vaccine. The proportion of individuals reaching antibody levels>1500 BAU/mL, defined as the primary endpoint, was not significantly different between patients with IMIDs and HCs (91% of patients vs 100% of HCs, p=0.101). A significant increase of anti-RBD antibodies was observed for patients as well as HCs, although median antibody levels at week 4 were lower in patients as compared with HCs (11 900 BAU/mL (5215–19 765) vs 17 880 BAU/mL (12 925–32 550) p=0.002) (figure 2A). The absolute change of anti-RBD-antibodies between week 0 and week 4 was lower in patients as compared with HCs (11 661.9 BAU/mL (5033.9–19 546.3) vs 17 483 BAU/mL (12 511.5–32 097); p=0.003) (figure 2B). However, fold change was significantly higher in patients with IMIDs (p<0.001) reflecting lower antibody levels at week 0 (figure 2C). Anti-RBD antibodies correlated with neutralising antibodies against the WT virus and Omicron BA.2 variant at week 4 (R=0.87, R=0.86, both p<0.001) (online supplemental figure 1A). Accordingly, neutralising antibodies against SARS-CoV-2 WT were significantly reduced in patients as compared with HCs (median NT level: 160 (80–480) vs 320 (160–640); p=0.016) (figure 2D). The absolute change in NT levels between week 0 and week 4 was numerically lower in patients than in HCs; however, this did not reach statistical significance (median absolute change (Δ) of NT level: 160 (80–452.5) vs 310 (150–610); p=0.06) (figure 2E). Neutralising antibodies against the Omicron BA.2 variant were significantly lower in patients when compared with HCs at week 4 (median NT level: 50 (15–130) vs 120 (60–240); p=0.001) (figure 2F). Overall, Omicron BA.2 NT titers were significantly lower than titers against the WT virus in all groups (figure 2D,F and online supplemental figure 1B).
 Figure 2
Figure 2 Humoral immune response at week 4 after the third vaccination. (A) Antibody levels to the receptor-binding domain (RBD) of the viral spike (S) protein in patients (Pat., n=56) and healthy controls (HCs, n=47) at screening (week 0) and at week 4 after the third vaccination. (B) Absolute change (Δ) of anti-RDB antibody levels between week 0 and week 4 after the third vaccination. (C) Fold change (FC) of anti-RBD antibody levels between week 0 and 4 in patients and HCs. (D) Neutralising antibodies against SARS-CoV-2 WT at week 0 and at week 4 after the third vaccination in patients (n=55) and HCs (n=45). (E) Absolute change (Δ) of neutralising antibodies against SARS-CoV-2 between week 0 and week 4 after the third vaccination. (F) Neutralising antibodies against the SARS-CoV-2 Omicron variant (BA.2) at week 4 after the third vaccination in patients (n=56) and HCs (n=46). NT, neutralisation test.
Cellular immune responseSARS-CoV-2-specific T-cell responses were determined by ELISpot assay before and at week 1 after the third vaccination in 41 patients and 20 HCs. Characteristics of the patients and HCs in whom T-cell responses were assessed are shown in online supplemental table 2. Post-hoc analysis revealed a significant increase in SARS-CoV-2-specific spot-forming cells (SFCs) after a third vaccination for patients after restimulation with WT (median, week 0: 35 (12.5–95.0) vs week 1: 104, (45–370) per 106 SFCs; p<0.001) and Omicron peptides (median, week 0: 44.5 (23.875–85.5) vs week 4: 121.5 (49.75–300.75) per 106 SFCs; p<0.001) 1 week after a third vaccination. Similar effects of a third vaccination on T-cell response were observed for HCs after restimulation with Omicron peptides (p=0.021), whereas only a modest increase could be detected after restimulation with WT peptides (p=0.11) (figure 3A,B).
 Figure 3
Figure 3 SARS-CoV-2-specific T-cell response. SARS-CoV-2-specific T-cell responses were determined by enzyme-linked immunosorbent spot (ELISpot) assay from peripheral blood mononuclear cells (PBMCs) stimulated with wild type (WT) and Omicron spike subunit S1 and S2 peptide pools 1 week after the third vaccination. (A) Representative ex vivo IFN-γ ELISpot result from unstimulated PBMCs (neg) and PBMCs stimulated with phytohemagglutinin (pos) or spike subunit S1 and S2 peptide pools (S1, S2) shown for one healthy control (HC). Y-axis indicates the number of spot-forming cells (SFCs) per 106 PBMCs. Data show the sum of average SFCs/106 PBMCs from S1 and S2 peptide pools. (B) Composite ELISpot results from 41 patients and 20 HCs before and after a third vaccination. Dots show the sum of total responses from S1 and S2 peptide pools.
Contributing factors for vaccination responseOverall, 48.2% of the patients received conventional synthetic (cs) disease-modifying anti-rheumatic drug (DMARD) monotherapy, 26.8% were treated with biologic (b)DMARD monotherapy and 19.8% of the patients received combination therapy (csDMARD and bDMARD). One patient received combination therapy with a targeted synthetic DMARD. In total, 12 patients received glucocorticoids as comedication with a maximum dose of 25 mg prednisolone (online supplemental table 3). Exploratory analysis revealed reduced anti-RBD antibody levels at week 4 in patients treated with bDMARDs and combination therapy (figure 4A and online supplemental figure 2A). Accordingly, NT levels against the WT virus and Omicron BA.2 variant were lower in patients treated with combination therapy (figure 4B,C and online supplemental figure 2B). Neutralising antibodies against the Omicron variant were consistently lower in all treatment groups when compared with the WT virus (online supplemental figure 2C). No clear difference of the fold change of RBD-specific antibody levels between week 0 and week 4 was detected between different treatment groups (figure 4D).
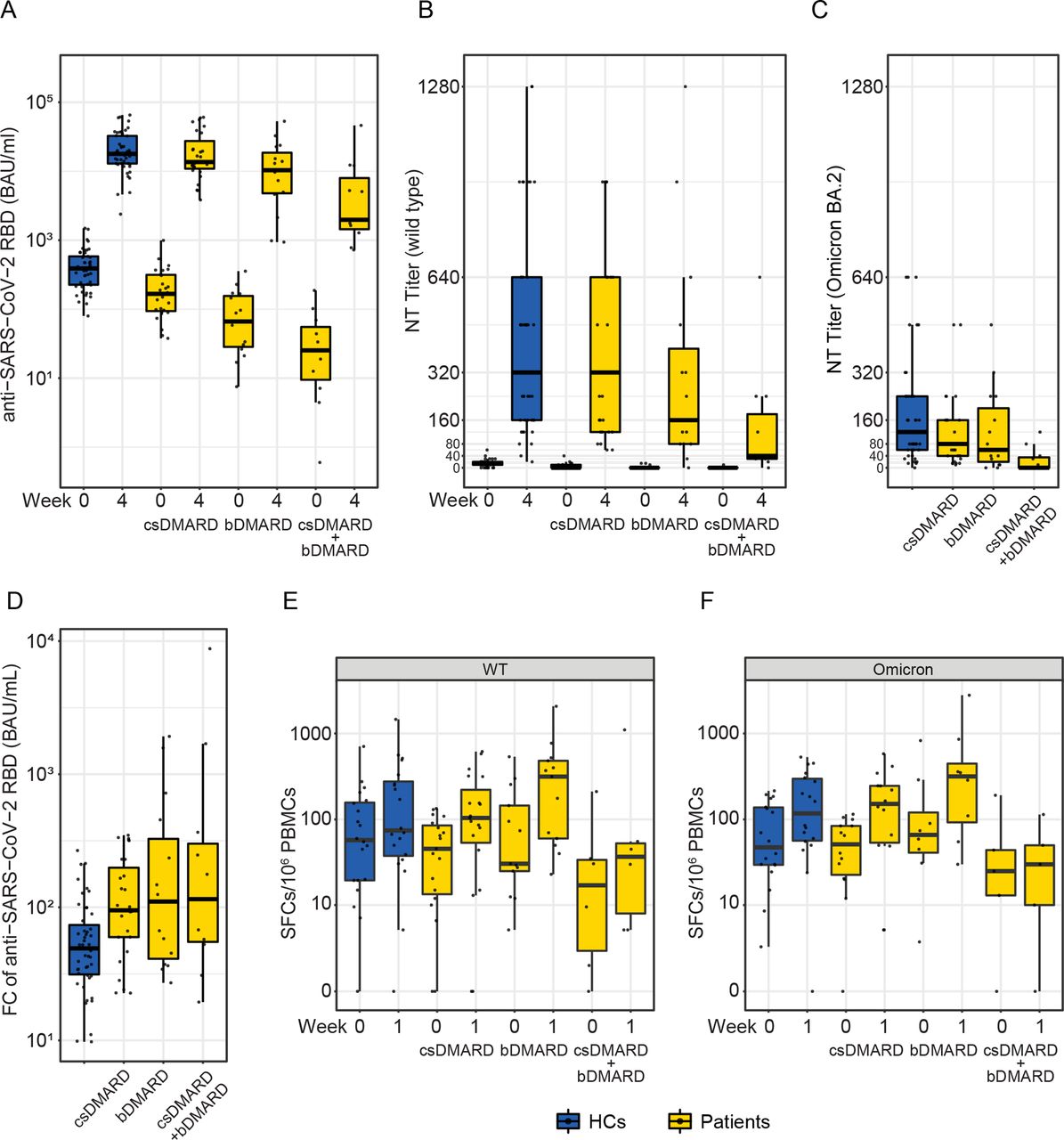 Figure 4
Figure 4 Treatment-specific response to the third vaccination. (A) Antibody levels to the receptor-binding domain (RBD) of the viral spike (S) protein in patients treated with conventional synthetic (cs) disease-modifying anti-rheumatic drugs (DMARD) (n=27), biological (b)DMARD (n=15) or a combination of csDMARDs and bDMARDs (n=11) and healthy controls (HCs, n=47) at week 0 and at week 4 after the third vaccination. (B) Neutralising antibodies against SARS-CoV-2 WT in csDMARD (n=27), bDMARD (n=15) or csDMARDs and bDMARDs combination (n=11) treated patients and HCs (n=45) at week 0 and at week 4 after the third vaccination. (C) Neutralising antibodies against the Omicron variant (BA.2) in patients treated with csDMARDs (n=27), bDMARDs (n=15) or a combination of csDMARDs and bDMARDs (n=11) and HCs (n=46) and at week 4 after the third vaccination. (D) Fold change of anti-RBD antibodies between week 0 and 4 was calculated for patients and HCs. (E,F) SARS-CoV-2-specific T-cell responses were determined by ELISpot assay from peripheral blood mononuclear cells stimulated with WT and Omicron spike subunit S1 and S2 peptide pools at week 1 after the third vaccination in 41 patients and 20 HCs. Dots show sum of total responses from S1 and S2 peptide pools. NT, neutralisation test.
An increase in spike-specific T-cells in patients under csDMARD therapy and bDMARD therapy was observed in response to WT and Omicron S peptide pools (S1/S2) after the third vaccination, whereas no difference was detected in patients with combination therapy of csDMARDs and bDMARDs (figure 4E,F).
ReactogenicityOverall, 92.7% of the patients and 89.4% of the HCs reported one or more systemic or local reactogenicity. Pain at the site of vaccination was the most common symptom reported in both groups (patients=78.2%, HCs=76.6%), followed by fatigue (patients=60.0%, HCs=51.1%) and myalgia (patients=34.5%, HCs=40.4%). Other symptoms occurred less frequently and are listed in online supplemental table 4 and shown in figure 5A,B.
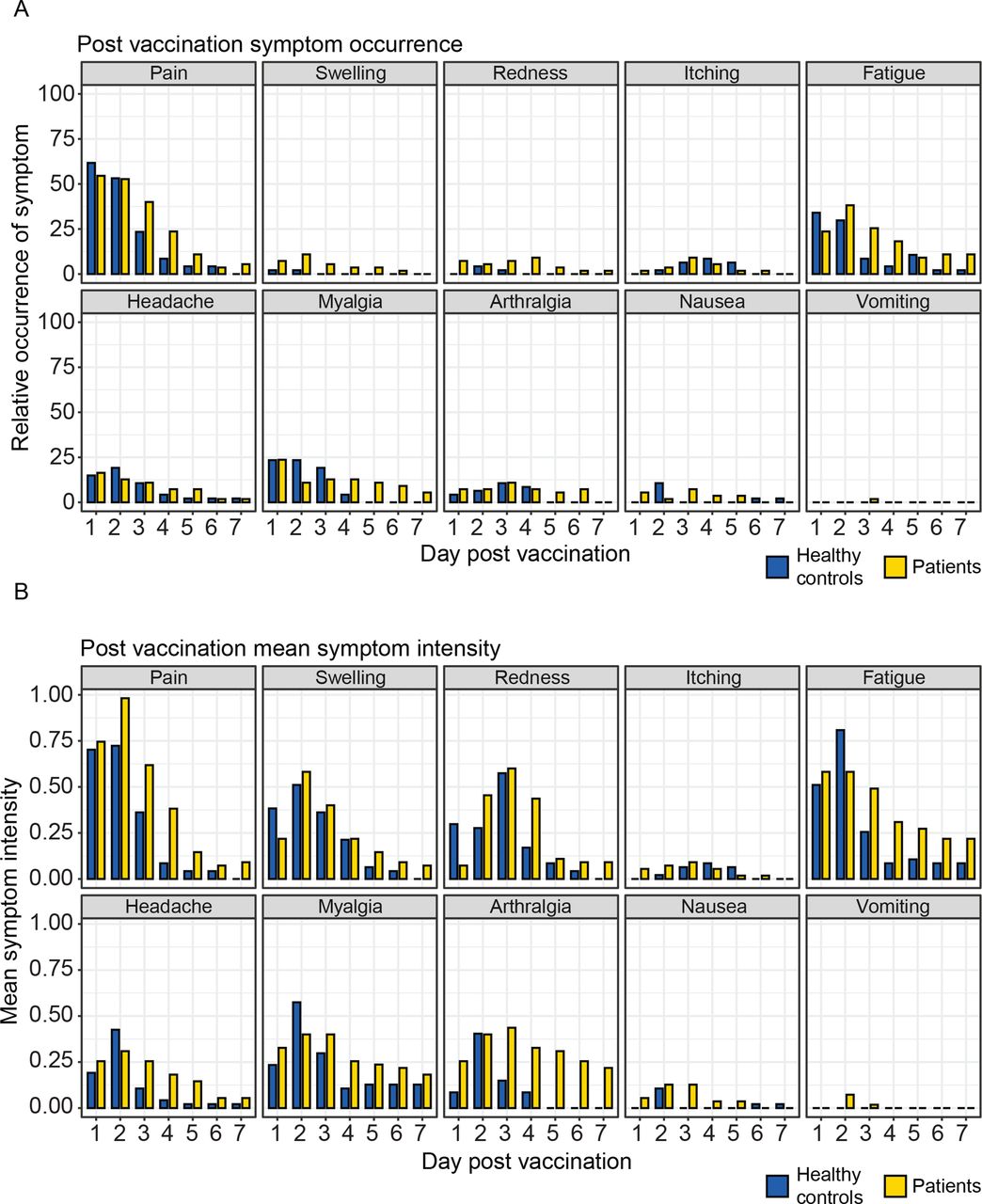 Figure 5
Figure 5 Reactogenicity. Reactogenicity after the third vaccination. Systemic symptoms and manifestations at the site of injection were recoded over a period of 7 days after vaccination: (A) Relative occurrence of the indicated symptom in patients and healthy controls. (B) Mean symptom intensity. Symptom severity was assessed on a numeric rating scale between 0 and 3.
Even though occurrence and intensity of pain at the vaccination site was comparable at day 1 post vaccination, pain was reported as prolonged and pronounced by patients when compared with HCs. Similar findings were found for fatigue, myalgia and headache. Arthralgia, reported by 21.8% of the patients and 14.9% of the HCs, however, was described as more severe in patients (figure 5A,B). Body temperature was measured once daily but did not show any differences between patients and HCs (online supplemental figure 3). One serious adverse event was reported, which was not related to vaccination (hospitalisation because of syncope and hypotension in the context of a urinary tract infection, 32 days after vaccination).
DiscussionIn the current trial, we could show an enhanced humoral and cellular immune response in patients with IMIDs and HCs after a third vaccination.
These findings are in line with the recommendations of the CDC and WHO, which unequivocally recommend a third vaccination for immunocompromised individuals and support the most recent statements of the ACR.19 49 50
Antibody levels after primary COVID-19 vaccination wane over time in healthy individuals and even more in immunosuppressed patients, underlining the importance of a third vaccination.51
In our study, we observed a good immune response to a third vaccination in patients with IMIDs and HCs, which is in contrast to current data for solid organ transplant recipients after a third vaccination.21 22 33 This discrepancy might be explained by differences in the patient cohorts as in our trial all patients and HCs already had seroconverted after primary vaccination. In addition, transplant patients have a higher immunomodulation due to the use of multiple immunosuppressants.
A detailed understanding of the impact of immunosuppressive therapies in patients with IMIDs on a third vaccination, however, is still lacking. Since we and others have already reported effects of a third vaccination in rituximab-treated patients, we excluded this group from our study.48 52–54 Analysis of our patients based on therapeutic strategy revealed a potential effect of bDMARDs and combination therapy of bDMARDs and csDMARDs on anti-RBD antibody levels. These data are in line with recently published results from Aikawa et al who identified that csDMARDs (mainly MMF) as well as bDMARDs (abatacept, rituximab and belimumab) can affect antibody levels after a third vaccination with an inactivated SARS-CoV-2 vaccine.25 Effects of csDMARDs such as methotrexate and/or combination therapy with TNF-inhibitors on seroconversion and antibody levels have also been reported after primary vaccination.38 41 55 56 However, when we compared the fold change of anti-RBD antibody levels between week 0 and week 4, we could not detect differences between various treatment groups, suggesting that the difference in antibody levels at week 4 might also be due to lower antibody levels at week 0. In line with previously published data, which reported a more rapid decrease of antibody levels over time in immunosuppressed patients, we observed reduced antibody levels in our patient with IMID cohort, even despite the shorter time period between a second and third vaccination.51
In contrast to Aikawa et al we did not see effects of glucocorticoids on antibody levels, which might be due to the different vaccines used. Additional studies with higher patient numbers might be needed to sufficiently address the role of glucocorticoids on a third vaccination. Data on neutralising antibodies in immunosuppressed patients after a third vaccination are scarce, in particular for new variants of concern (VOCs).21 57 58 We found a significant correlation of anti-RBD antibodies and neutralising antibodies against the WT virus and the Omicron BA.2 variant. Neutralising titers against the latter were significantly lower, suggesting a potential reduction of clinical protection against new VOCs.59 In line with recently published data, neutralising antibodies against the WT virus and Omicron variant were lower in patients treated with bDMARDs and combination therapy of bDMARDs and csDMARDs, consistent with reduced anti-RBD antibody levels.25 56
Cellular immune responses are a key for the development of a vaccination-induced immunogenicity. To our knowledge, this is the first study that investigates cellular immune responses after a third vaccination in patients with IMIDs as compared with HCs. We could show that a third vaccination leads to an enhanced cellular immune response in patients with IMIDs after restimulation with WT and Omicron peptides, highlighting the relevance of a third vaccination for the most recent variant of concern.
One reservation concerning a third vaccination is the risk of severe adverse events. However, within the observation period, we recorded no serious adverse events related to the third dose. Reactogenicity was comparable to initial reports.60 61 While the prevalence of side effects was comparable between patients with IMIDs and HCs, prolonged intensity of symptoms such as fatigue, local reactions, myalgia and arthralgia was observed for patients with IMIDs as compared with HCs. Our study has several limitations. Due to insufficient recruitment of HCs and an unexpectedly high drop-out rate, the study was underpowered (79% of planned sample size). A higher immunogenicity has been described for mRNA-1273 as compared with BNT162b2 vaccine.40 62 This has to be taken into account since a higher proportion of the patient cohort received a third vaccination with the mRNA-1273 vaccine, which might obfuscate differences in immunogenicity between both groups. Although reduced antibody levels were observed in patients with different treatment strategies, larger cohorts will certainly be needed to fully address the role of individual immunosuppressive drugs and disease entities for the immunogenicity and efficacy of a third COVID-19 vaccination.
Taken together, our data provide evidence for the immunogenicity and safety of a third vaccination in immunosuppressed patients.
Data availability statementData are available upon reasonable request. Anonymised data will be available upon request.
Ethics statementsPatient consent for publicationEthics approvalThis study involves human participants. The study procedures followed Good Clinical Practice guidelines and the Declaration of Helsinki. The trial protocol was approved by competent authorities and the ethics committee of the Medical University of Vienna (No: 1583/2021). Participants gave informed consent to participate in the study before taking part.
AcknowledgmentsWe thank all participants of the study. Special thanks go to Martina Durechova, Daffodil Dioso, Elyza Raymundo and Michael Zauner for their support. We thank Brigitte Meyer, Birgit Niederreiter, Carl-Walter Steiner, Jutta Hutecek, Ursula Sinzinger, Patrick Mucher and Sylvia Taxer for their assistance.
留言 (0)