
記住我

The setting of this study is the community health promotion programme Voorstad on the Move (VoM). This local programme was one of 46 small-scale projects under the umbrella of the Healthy Futures Nearby (HFN) programme funded by the private funding organisation, FNO, with the aim of reducing health inequalities within the Netherlands [35]. From September 2016 to the end of 2019, VoM was developed and implemented in a socioeconomically deprived city district of 10,750 inhabitants in a city in the eastern part of the Netherlands. In this city district, both the SES and the health status of inhabitants are relatively low compared with other parts of the city [36]. The VoM programme pursued multiple goals. On the one hand, it aimed to improve Voorstad inhabitants’ perceived health and achieve changes in the social and physical environment in order to support healthy behaviours. At the same time, it focused on finding keys to reducing health inequalities [37]. VoM is a local programme developed and implemented with the active involvement of low SES citizens, who – in the view of health professionals – are usually hard to reach and not very interested in health promotion activities. The programme was innovative, as it differed from usual health promotion programmes in which health and lifestyle themes and activities are set by professionals. Instead, this programme shifted from being a predetermined health promotion programme with a set of health behaviour interventions to being an open approach with a focus on the action principles, citizen participation and intersectoral collaboration. The VoM programme was guided by participatory action research (PAR) [13, 37]. During the programme, stakeholders were continually involved, and different perspectives of citizens and professionals were captured and used to optimize consequent actions. As such, the development of capacities, learning, and empowerment was facilitated [38, 39].
In September 2016, the VoM programme started as a collaboration of five organisations, all part of the existing social infrastructure: the municipal health service, the Voorstad social support team (SST), the welfare organisation, the neighbourhood viability coalition, and the local sports service organisation. The programme’s driving and leading force was the VoM coalition, with representatives of the five organisations, all community workers, along with a health broker, who was an inhabitant of Voorstad, working in a self-employed capacity. The benefits of a broker role, especially in health promotion, lie in connecting stakeholders from health and non-health sectors with citizens, and subsequently stimulating an integrated community approach to address health inequalities [40]. The coalition members built a communitywide network of organisations, workers, and citizens based on the existing social infrastructure and the contacts that each of them brought in. The health broker role was essential in connecting the VoM coalition with the broader network and in facilitating citizen participation [38]. Citizens’ perspectives on health were explored with existing community groups – consisting of Voorstad inhabitants (e.g., a walking, a yoga, and a knitting group) and volunteers at a community centre and a play garden – in two group sessions with each group [39]. These community groups were actively involved in the VoM programme from the start.
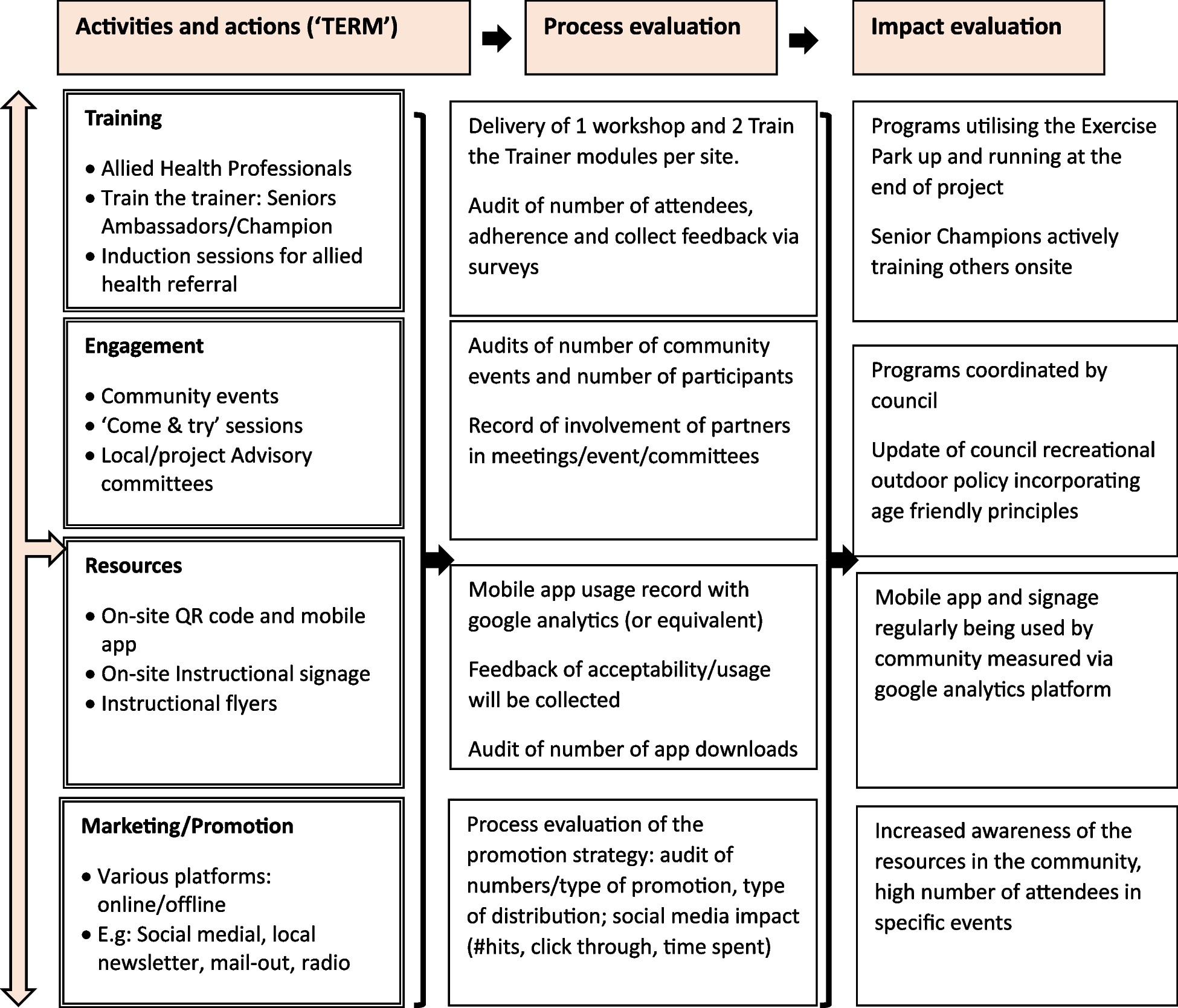
Based on the literature on community-based approaches and evaluation studies of complex community health promotion programmes [41,42,43,44], we composed an initial programme theory, represented by the a logic model (Fig. 1). This model was used for the development, implementation, and evaluation of the VoM programme [37].
Fig. 1
Logic model ‘Voorstad on the Move’ based on [37]
The assumption is that developing and implementing health activities at different levels – i.e., citizens, community workers, and community – will result in the long term in improved perceived health, a health-supportive environment, and sustainable local health policy, and ultimately lead to a reduction in health inequalities. These long-term expected outcomes will be preceded by short-term outcomes, defined as outcomes of interest such as health literacy, healthy alliances, and changes in the physical environment. Besides intended short-term and long-term outcomes, there might be unplanned outcomes that sometimes have a greater influence on the health determinants for a community than the more narrowly focused outcome goals of projects [45]. Programme outputs that precede and generate short-term outcomes include, for example, insight into citizens’ perception on health, new health-promoting activities, an extended community network, new coalitions of primary care professionals and social support workers, and municipal involvement. Another assumption is that, by applying the citizen participation and intersectoral collaboration action principles, programme outputs will be generated, leading to short- and long-term outcomes as already explained.
Study designA critical realist perspective was followed to study the citizen participation and intersectoral collaboration action principles in depth, in the single case of VoM. The critical realist perspective was used as the VoM programme was part of an open system which has implications for the outcomes being produced [46]. This method is based on the identification of outcome patterns, mechanisms, and contextual conditions that help to assess not only what works, but also for whom and in what circumstances [47,48,49]. The final research product from the critical realist methodology is not a statement of effect size, but rather a refinement of the programme theory [33] based on the gathered insights regarding the mechanisms that have triggered the outcomes in this specific community health promotion programme [50]. The step wise (secondary) analysis of data from multiple sources resulted in context-mechanism-outcome (CMO) configurations, related to the action principles part of the VoM programme theory [51].
Data collectionAs part of the PAR that accompanied the VoM programme, a range of qualitative data was collected throughout the programme between 2017 and 2019. In addition, data collected by researchers from the overall evaluation of the FNO HFN programme were analysed [52]. Data used in this study originated from multiple sources and methods to ensure validity. Sources and methods include for example midterm and end evaluation sessions with coalition members; individual interviews and group sessions with community workers, the health broker, and citizens; semi-annual progress reports prepared by the programme coordinator; and minutes of the VoM coalition meetings (Table 1). In addition, an activities database, in which characteristics and reports of the activities that were part of the VoM programme were registered and monitored, was consulted. All sources were used to study both action principles, except the data from the sub study ‘Benefits of participation’ (V), which was only used for the action principle citizen participation. The photo-voice study (IV), the semi-annual reports (VI) and minutes of coalition meetings (VII) were also used to clarify the context.
Table 1 Data collection schemeData analysisInterviews and group sessions were anonymised and transcribed ad verbatim. The analysis was stepwise, data driven, and thematic [56], using Atlas-ti 22. Coding was developed based on a realist synthesis protocol with the focus on CMO configurations, looking not only at what worked, but also for whom and why it worked [46,47,48]. The operationalisation of the concepts – context, mechanisms, and outcomes – is illustrated in Table 2.
Table 2 Operationalisation of context-mechanism-outcomes concepts in the VoM programmeStep 1Transcripts of the evaluation sessions (Sources I–III, Table 1) were coded in terms of context conditions (C), underlying mechanisms (M) in the actual programme, and outcomes observed by respondents (O) [58].
Step 2Quotes coded as context were further thematised into historical-, organisational-, and programme-related codes. Quotes coded as mechanisms were also further thematised into programme- or participant-related. Quotes coded as outcomes were classified as related to citizens, community workers, or community. Each theme was further refined into subthemes and labelled as supportive ( +) or restraining (-), thus addressing the aim of differentiating and accumulating evidence on positive and negative CMO configurations [51].
The coding procedures were conducted independently by two researchers (first and second author). Both researchers found that the same phenomenon could be coded as outcome or context, or as context and mechanism, as was also found by Herens et al. [33]. Differences in coding were discussed until consensus was reached, thereby making explicit that all coding was based on the perspective of the actual VoM programme activities and processes.
Step 3Sources IV and V (Table 1) were part of sub-studies in which (IV) citizens’ perspectives on the living environment were studied [54] and (V) active citizens were asked about the benefits of participation in (health promotion) activities and volunteer work [55]. Transcripts of the interviews and group sessions were also coded in terms of contexts (C), mechanisms (M), and outcomes (O). Deductive or top-down analysis was applied by the first author, based on the mechanisms and CMO configurations resulting from Steps 1 and 2.
Step 4The reports and minutes of the meetings (Sources VI and VII, Table 1) were studied to check how often and in what manner the context conditions, mechanisms, and outcomes of interest found in Steps 1 and 2 had been reported.
Step 5The activities database (Source VIII, Table 1) was used to gather more in-depth information about the programme outputs, e.g., the number of participants, the involvement of community workers, duration of the activities, and so forth.
On completion of these steps, two researchers (MdJ, GW) brought together the results in an overview of the most important context conditions, mechanisms, and reported outcomes for each of the action principles. First, the citizen participation action principle was elaborated, followed by intersectoral collaboration, and this made an overlap in CMO configurations visible. The context conditions were divided into supportive and restraining, and programme-related context conditions were marked. The overviews were presented in two figures, one for each action principle (Figs. 2 and 3). Subsequently, these figures were discussed with all authors (MdJ, GW, MK, AW) and consensus was reached.
Fig. 2
CMO configurations citizen participation
Fig. 3
CMO configurations intersectoral collaboration
留言 (0)