The facial nerve is responsible for facial expression, lacrimation, and salivation. It emerges from the brainstem at the cerebellopontine angle; then, through the fallopian canal, it enters the petrous temporal bone via the internal auditory meatus; and finally, it exits through the stylomastoid foramen, becoming the extracranial facial nerve [7]. In this phase, the facial nerve forms 5 terminal branches supplying the motor function of the face [8]. Interestingly, the frontal branch has bilateral cortical input, which means that the motor function of the forehead is preserved in upper motor neuron lesions but absent in lower motor neuron lesions [7].
Understanding the anatomy of the facial nerve is essential to identify the level of the lesion in case of facial palsy. Facial palsy may be distinguished from facial nerve palsy (due to a peripheral lesion) or central facial palsy (due to a central lesion involving the upper motor neuron). They clinically differ in the preservation of function of the forehead muscles in the central form, which requires a prompt evaluation for the intracranial process [9].
On physical examination, the patient with facial nerve palsy is unable to raise the eyebrow or close the eyelid on the affected side. The nasolabial fold is typically absent and the affected side presents a dropping mouth rim, with possible saliva leakage and the inability to smile [10]. If stapedius muscle paralysis is present, the patient may experience hyperacusis.
Importantly, lacrimal and salivary production can be reduced, and lagophthalmos can promote corneal irritation with abrasion and ulceration. Therefore, the use of eye-protective measures is strongly recommended [9].
The possible etiologies of facial nerve palsy in children can be divided into congenital or acquired causes, which in turn can be further classified as infectious, traumatic, malignancy-associated, hypertension-associated, and idiopathic (Bell's palsy). Table 1 summarizes the possible causes of facial nerve palsy. The degree of facial nerve palsy can be scored using the House-Brackmann scoring system, as shown in Table 2 [11].
Table 1 Etiologies of facial nerve palsy in pediatric ageTable 2 House-Brackmann facial nerve grading systemHerein, we describe a case of AOM-related facial nerve palsy whose incidence has become extremely rare after the widespread use of antibiotics [12]. The etiology of facial nerve palsy in patients with AOM is unclear, although different hypotheses have been postulated. Firstly, in the early stage, AOM may cause retrograde infection within the facial nerve canal. Secondly, the presence of inflammatory bacterial toxins may induce peripheral demyelination of the facial nerve. Finally, the spread of the inflammatory process into the mastoid region may provoke inflammation or compression of the facial nerve. Moreover, once a chronic infection occurs, a cholesteatoma may directly compress and erode the facial nerve [8]. Other authors suggest that the insult is caused by the compression and thrombosis of the microvasculature supplying the facial nerve, determining neuritis and nerve palsy [13].
In our patient, an EBV primary infection was serologically documented. EBV belongs to the human herpesvirus family acknowledged to cause neurological complications in 0,5–7,5% of patients with acute infection [14, 15]. Facial nerve palsy with AOM associated with primary EBV infection is rarely encountered in children. Volgelnik et al. described 5 cases of unilateral facial nerve palsy with ipsilateral AOM and primary EBV infection [5] in otherwise healthy children between 17–27 month-old, which received antibiotic treatment and underwent a myringotomy of the affected ear with tympanostomy tube insertion within 24 h after admission. Only one patient underwent mastoidectomy in addition to myringotomy. Interestingly, in situ hybridization analysis of biopsied material showed EBV-specific ribonucleic acid. Complete recovery of the facial nerve was documented in 4 patients, whereas a slight paresis occurred in one patient two years after the hospitalization. Recently, Yamaguchi et al. have reported two cases of 18 and 19-month-old female children with unilateral facial nerve palsy with ipsilateral AOM and primary EBV infection [6]. They received oral corticosteroids and vitamin B12 supplementation, and both recovered after 12 and 6 weeks, respectively.
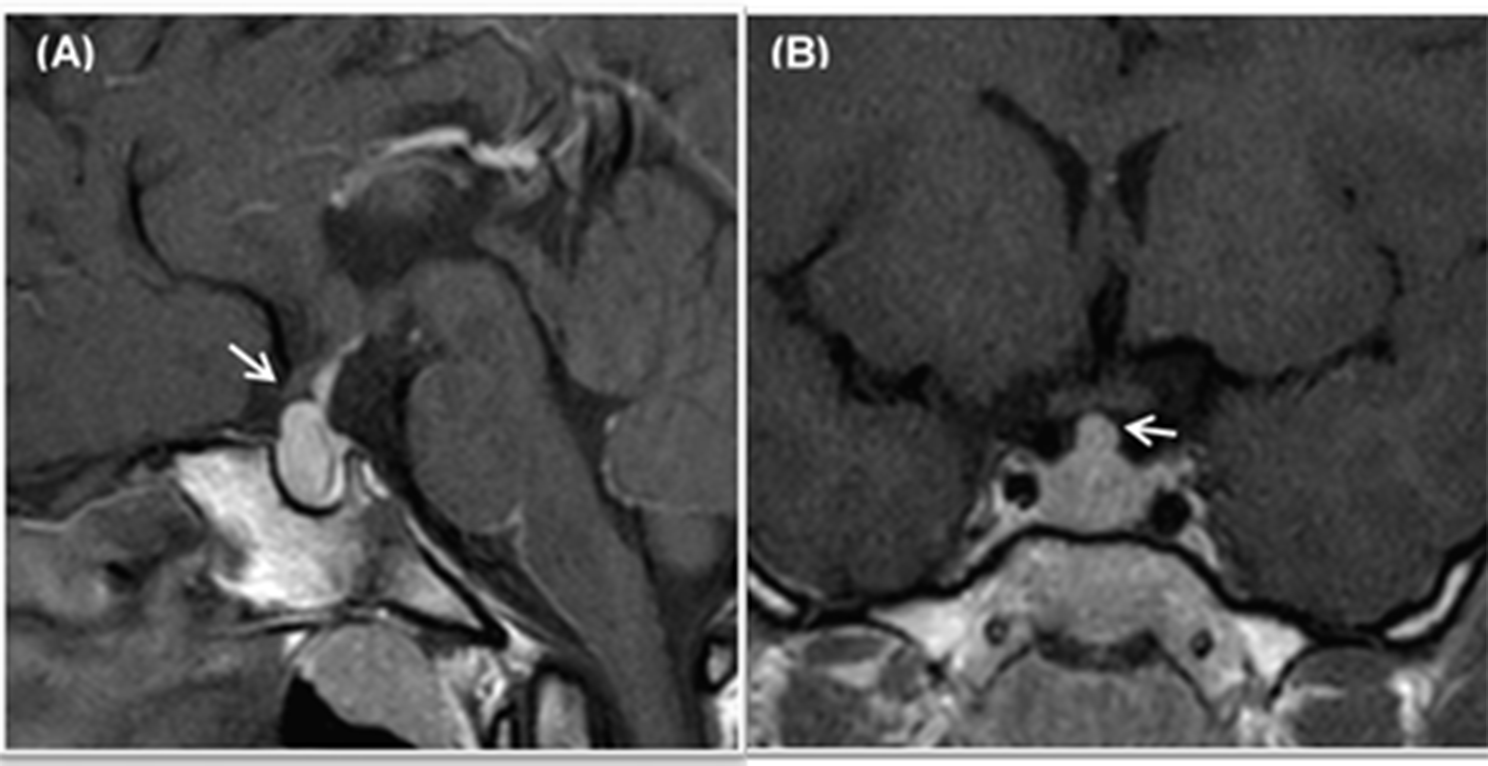
In our patient, the suffering of the facial nerve at the level of the geniculate ganglion and its labyrinthine portion detected through MRI, in absence of any bony erosion, suggested that acute infectious neuritis of the facial nerve spreading from the middle ear (probably through a microvascular route) was the underlying causative mechanism. Under these circumstances, a concomitant EBV infection could have paved the way to a following bacterial superinfection responsible for both the middle ear and the facial nerve infection.
In a patient with AOM-related facial nerve palsy, a CT scan of the head should be performed to exclude the radiological diagnosis of otomastoiditis and to document the presence of associated intracerebral orextracerebral complications [16]. Furthermore, MRI of the head can be used not only for diagnostic purposes but also to detect rare complications of otomastoiditis such as dural sinus thrombosis [17].
Once diagnosed, AOM-related facial nerve palsy should be adequately treated, with the eradication of the suppurative process as the first goal to achieve [18]. To this aim, the patient should receive a broad-spectrum intravenous third-generation cephalosporin (for example cefotaxime as in our case) as an initial antibiotic regimen, to be eventually adjusted based on the microbiological antibiotic sensitivity in positive cultures [16].
To date, no treatment consensus on AOM-related facial palsy is available. Indeed, the role of surgery, corticosteroids, and antivirals remains controversial. Several authors agree on the need for myringotomy with or without tympanostomy tube placement in cases with otomastoiditis without perforation of the tympanic membrane, suggesting to perform mastoidectomy or, rarely, facial nerve decompression if no improvement is achieved within a few days [13, 19, 20]. Recently, Eeten et al. have described two cases of EBV otomastoiditis complicated by facial nerve palsy that, initially not improved with the medical treatment alone, subsequently recovered after a surgical approach with mastoidectomy plus atticoantrotomy and a transmastoidal surgical decompression of the facial nerve, respectively [21].
Antiviral therapy has been used to treat peripheral facial palsy by considering the potential association with herpes simplex virus infection [22]. However, as the real effectiveness of antivirals’ administration in cases with facial nerve palsy is not fully understood yet, antiviral treatment should be avoided if no infectious cause is suspected [9]. As a consequence, in our case acyclovir was interrupted once herpetic virus serology resulted negative.
As far the use of corticosteroid treatment for facial nerve palsy, despite a few studies are available, it seems that steroids may reduce the time of recovery, especially when administered early in the disease course [7, 9]. To better understand the role of corticosteroids in the treatment of children with idiopathic facial nerve palsy, two randomized, double-blind, placebo-controlled trials have recently been started [23, 24].
As observed in our patient, the prognosis of AOM-related facial nerve palsy is generally good after the appropriate therapy, even though a 6% incidence of residual dysfunction has been described [25, 26], and the recovery of facial palsy usually occurs within 3-months. Furthermore, in the case of infectious etiology and incomplete forms, the recovery may be more quickly [12].
In conclusion, our case highlights a rare complication of AOM and primary EBV infection in children the pediatricians should be aware of. A prompt diagnosis and adequate treatment are essential to achieve a good outcome and to avoid chronic neurological sequelae.








留言 (0)