Patients
The present study included 62 newly diagnosed MM patients who were diagnosed during the period from May 2017 to December 2019. All patients were presented to the Outpatient Clinic of the Medical Oncology Department, National Cancer Institute (NCI), Cairo University, Egypt. Patients who received any previous chemotherapy outside NCI or with incomplete data were excluded from the study. All patients provided informed consent. The study was performed following the Declaration of Helsinki and was approved by the internal review board of the NCI.
Methods
The diagnosis of MM was based on the morphological examination of the peripheral blood (PB), BMA and BMB smears, serum protein electrophoresis (SPEP), serum immunofixation (IF), serum lactate dehydrogenase (LDH), albumin (ALB), serum calcium, serum ß2 microglobulin (β2M), serum creatinine (sCr), in addition to conventional cytogenetics, FISH. Radiographs (X-ray or CT chest) and magnetic resonance imaging (MRI).
The diagnosis of MM required 10% or more clonal plasma cells in the BM (and/or a biopsy proven plasmacytoma) plus any one or more myeloma defining events (MDE): end-organ damage (hypercalcemia, renal insufficiency, anemia, or bone lesions) attributable to the underlying plasma-cell disorder, BM clonal plasma cells ≥ 60%, serum involved to uninvolved free light chain (FLC) ratio ≥ 100 (provided involved FLC level is ≥ 100 mg/L), or more than 1 focal lesion (≥ 5 mm) on mMRI [5]. The treatment responses were evaluated according to the International Myeloma Working Group Panel Consensus.
Immuno-histochemistry
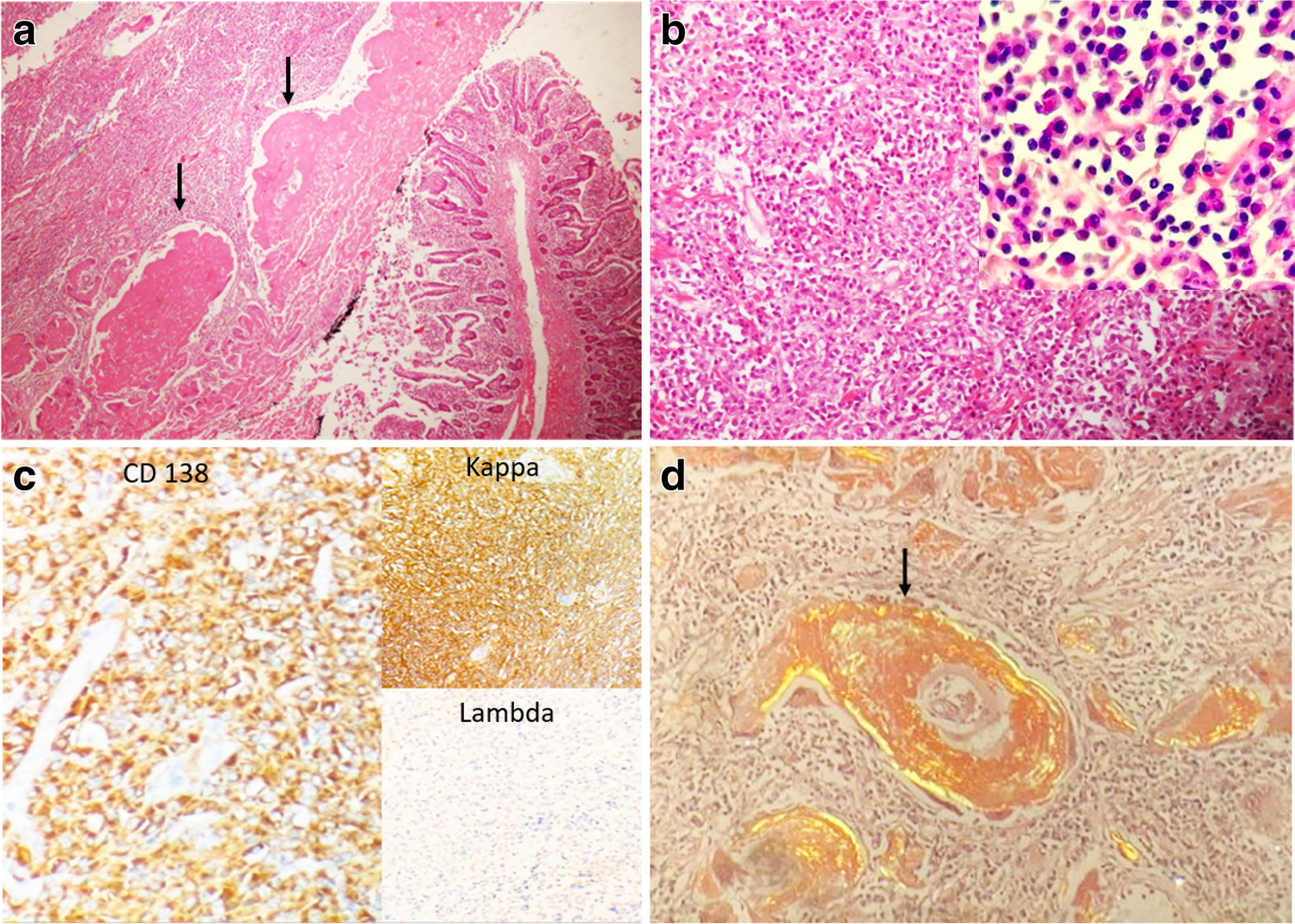
Immunohistochemistry analysis was performed to evaluate the expression of IFR4. Specimens of pre-treatment BM trephine biopsy were transported and fixed in formalin, decalcified in Formic acid-Sodium Citrate and processed to paraffin-wax embedding. Representative sections (3–4 μm) of each case were cut. For each case, 3 slides were prepared: one for Haematoxylin and Eosin (H&E) staining, the second for IHC staining using anti-CD138 and the third IHC assessment of IRF4 using anti-IRF4 (rabbit monoclonal, IgG, Chongqing Biospes Genemed, Biotechnologies, INC), according to manufacturer’s instructions.
Two senior hematopathologists independently scored the percentage of plasma cells and IRF-4 positive cells, using the staining of the endothelium as positive internal control in the tested slides by IRF4, and graded the immunostaining intensity as follows: plain: 0 point; shallow yellow: 1 point; pale yellow: 2 point; sepia: 3 point. For the scoring of positive results, a cut off of 10% was used. Based on the percentage of IRF4 positive cells, the patients were bichromatized into positive (≥ \(10\%)\), and negative (< 10%).
Based on staining intensity and the percentage of cells staining positively, the proportion of cells expressing IRF4 were further sub-classified as follows: 0, < 10% of plasma cells or no staining intensity, 1+, \(\ge \hspace\)10% with light staining, 3+, \(\ge \hspace\)60% with strong staining intensity, and 2+: for cases not scored as 1+ nor 3+.
Cytogenetic Analysis
For conventional cytogenetic analysis, BM specimens were cultured for 24 and 72 h without mitogens, and stained by G-banding, following the standard techniques. In most of the cases, at least 20 metaphases were analyzed using an IKAROS imaging system (Metasystems, Altlussheim, Germany).
Interphase FISH (iFISH) analysis was performed using IgH Breakapart probe (Metasystems, Altlussheim, Germany), according to the manufacturer’s instructions. A minimum of 200 interphase nuclei and 10 metaphases were analyzed using a fluorescence microscope (AxioImager.Z1 mot, Carl Zeiss Ltd., Hertfordshir, UK) with ISIS imaging system (Metasystems, Altlussheim, Germany). The karyotypes were interpreted using the International System for Human Cytogenetic Nomenclature (ISCN 2016) [28].
Management of the Patients
After diagnosis of MM, patients were divided into two main groups, transplant eligible and transplant ineligible. Transplant eligible patients with no marked co-morbidities and good performance status (PS 0–2) were offered bortezomib based regimen, namely VCD protocol (Cyclophosphamide 300 mg/m2, Bortezomib 1.5 mg/m2, Dexamethasone 40 mg on D1,8,15,22). Patients were requested to repeat SPEP (with IF), sβ2M monthly and BMA after 12 weeks therapy. Monitor of renal and liver functions were requested before each cycle. Responders continued same regimen and were prepared for Autologous BMT.
Patients with poorer PS & ineligible for transplant were offered either VCD or Lenalidomide. Patients with refractory/progressive disease were offered 2nd line therapy versus best supportive care (BSC) according to their performance and comorbidities. Second line protocols included Lenalidomide/Dexamethasone, VAD and Melphalan and prednisone. All patients were offered supportive treatment including Zoledronic acid and palliative radiotherapy (if clinically/radiologically indicated).
Statistical Analysis
Data management and analysis were performed using SPSS, version 22 (IBM, Armonk, Ny, USA). Qualitative data were presented as numbers and percentages, while the quantitative data were presented as median and interquartile ranges (IQR) or mean and standard deviation (SD), according to the appropriate normality test. The comparison between groups were performed using Chi-square test and/or Fisher exact test which appropriate. Mann–Whitney test was used for comparing numerical variables between two groups.
Survival analysis was done using the Kaplan–Meier test, and comparison between survival curves was done using the log-rank test. All tests of hypotheses had been conducted at the alpha level of 0.05, with a 95% confidence interval. All tests were two-tailed. The OS was calculated from the date of diagnosis till the date of last follow-up or death due to any cause while the DFS was calculated from the date of the diagnosis until the date of relapse, death during induction, death during CR, or second malignant neoplasms.



留言 (0)