
記住我


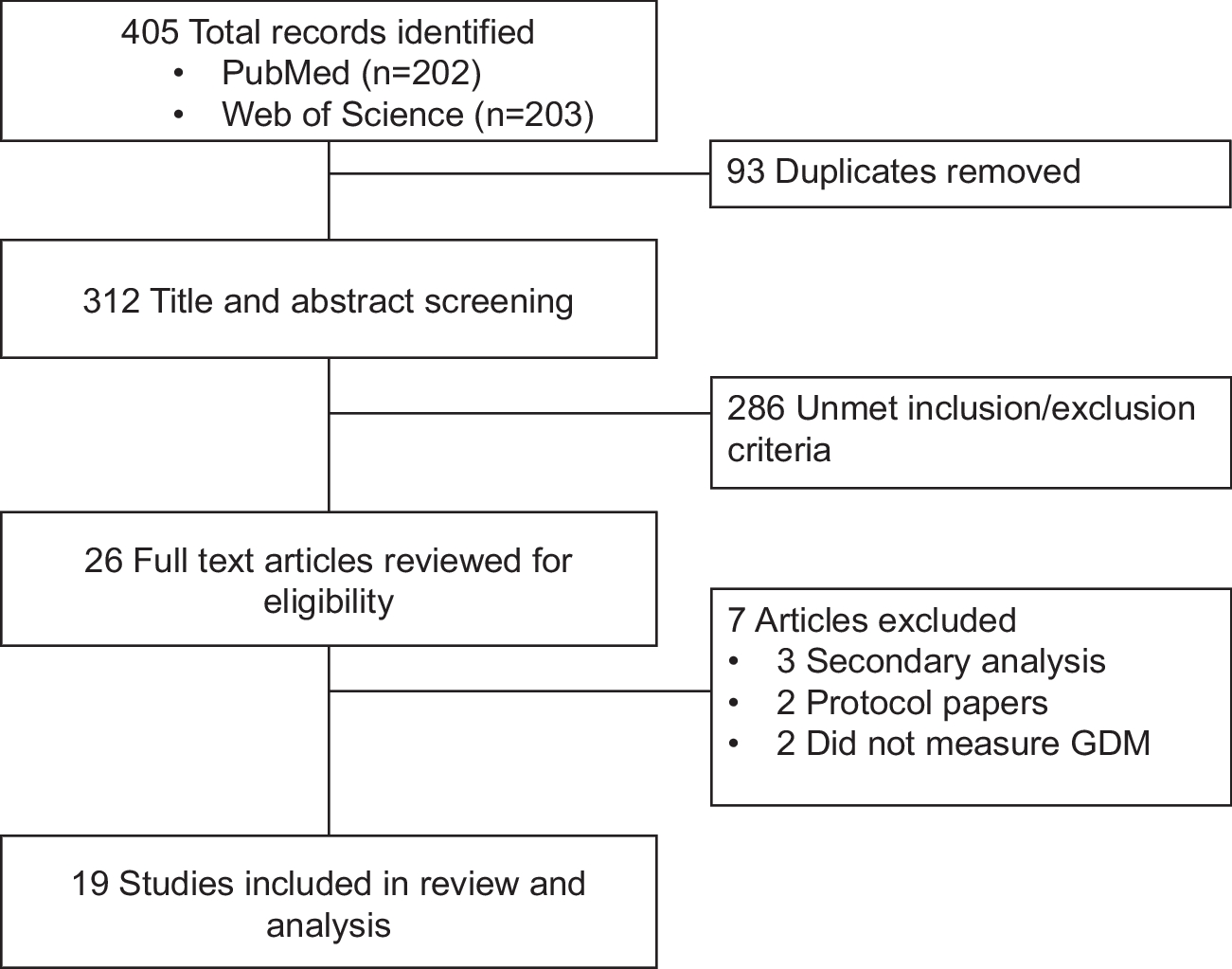
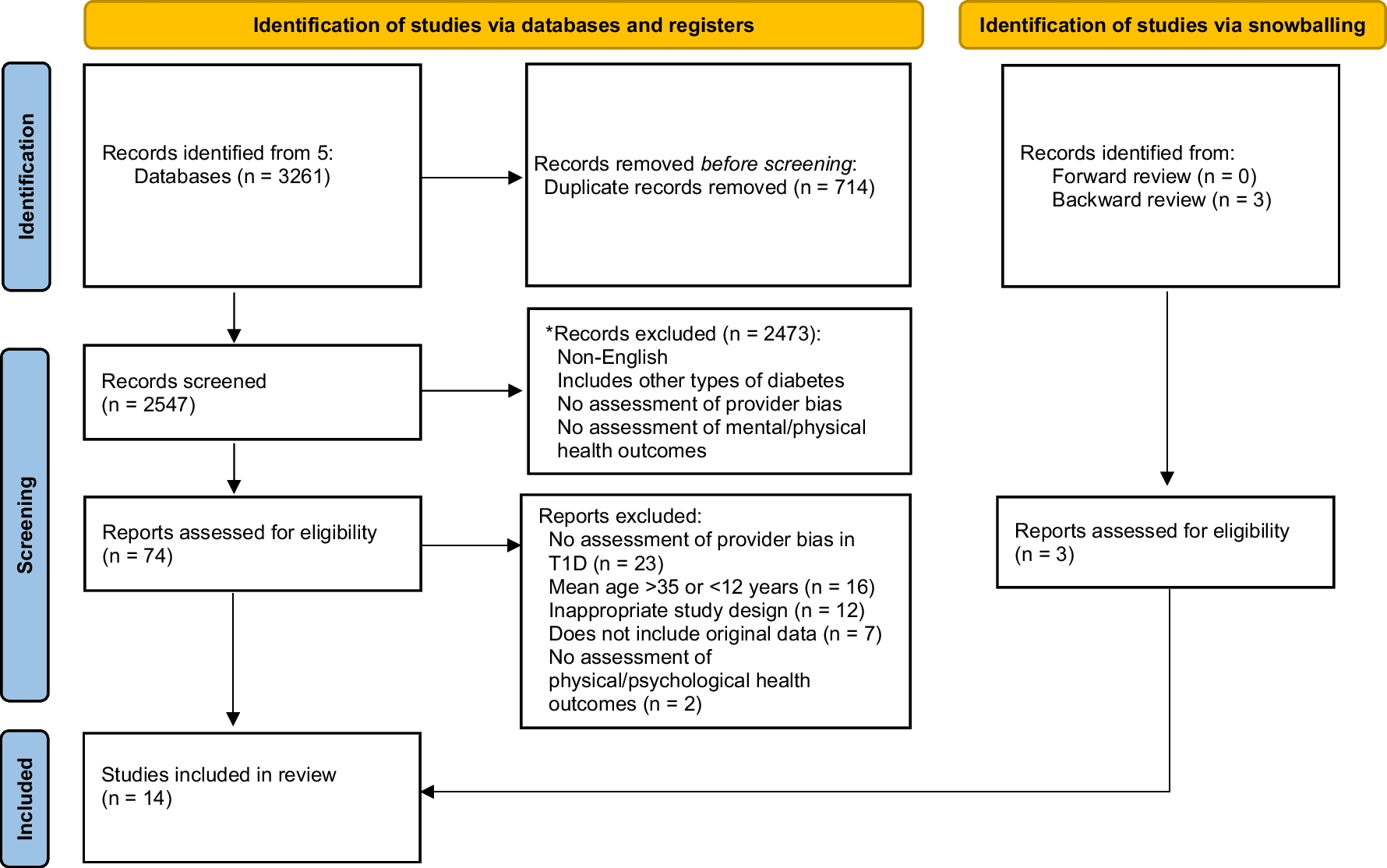

The initial search identified 138 publications, of which 123 were excluded at abstract-level screening because they were conducted in countries other than the US, were secondary analyses of the same study, not peer-reviewed, or irrelevant to the AYA with T1D population. Fifteen articles were further evaluated in full text. Of these, 8 provided original data on AYA with T1D regarding rates of substance use (see Fig. 1). We summarize findings from these 8 articles in Table 1, along with the most relevant comparison data from one of the national studies (YRBSS, BRFSS, and NSDUH).
Table 1 Recent rates of substance use in the AYA with T1D populationRates and Trends of Substance Use Among AYA in the USAAdolescentsThe CDC Youth Risk Behavior Surveillance System (YRBSS) was developed in 1990 to monitor health behaviors that contribute to leading causes of death, disability, and social problems among youth in the USA [20]. This survey is administered to students in grades 9–12, every odd calendar year, with 2019 being the latest data collection year. Surveys are self-administered in the school setting and students record their responses on a computer-scannable questionnaire booklet. From 2011 to 2019, the sample size ranged from 13,872 to 15,425 with an overall response rate of 60.3 to 71% [20, 21].
The most recent rates and trends for substance use, as reported by the 2019 CDC YRBSS, are as follows [20]:
Alcohol: 29.2% of high school students had at least one drink of alcohol in the past 30 days and 13.7% met the criteria for binge drinking (within the last 30 days) [20]. The trend data indicates that alcohol consumption rates among high school students have decreased by approximately 10% over the past 10 years [20].
Tobacco: 36.5% of high school students currently (within the last 30 days) smoked cigarettes, cigars, electronic vaping products, or smokeless tobacco [20]. Tobacco use is more difficult to trend as vaping data has only been collected since 2015. However, in general, rates of cigarette use have declined from 19.5 to 6% over the past 10 years, and vaping has increased from 24.1% in 2015 to 32.7% in 2019 [20].
Marijuana: 21.7% of high school students used marijuana in the past 30 days [20]. The trend data indicate that current marijuana use has remained about the same over the past 10 years [20].
Other illicit substances: 14.8% of high school students have used illicit drugs (cocaine, inhalants, heroin, methamphetamines, ecstasy, or hallucinogens) at least once in their lifetime [20]. The trend data indicate that lifetime illicit drug use has decreased by about 5% over the past 10 years [20].
Adolescents and Young Adults (AYA)The National Survey on Drug Use and Health (NSDUH) data are based on face-to-face interviews conducted by the Substance Abuse and Mental Health Services Administration (SAMHSA), an agency in the US Department of Health and Human Services. About 67,500 people ages 12 and above are surveyed annually, allocated across three age groups, with 25% allocated to adolescents aged 12 to 17, 25% to young adults aged 18 to 25, and 50% to adults aged 26 or older [4]. Comprehensive data reports are available from 2014 to 2020. In 2020, the sample size was 62,515 with a response rate of 60.41%. Of note, the 2020 report had inconsistencies in data collection compared to prior years due to the COVID-19 pandemic, so we include 2019 data in parentheses, when available.
The most recent rates and trends for AYA substance use, as reported by the 2020 NSDUH data, are as follows [4]:
Alcohol: 16.1% (18.5%) of participants aged 12–20 years reported alcohol use in the past month and 9.2% (11.1%) reported binge drinking [4]. This has decreased over the past 10 years, from 26.2% in 2010. 51.5% (54.3%) of participants in the 18–25 years age group reported current alcohol use (in the past 30 days) and 31.4% (34.3%) met the criteria for binge drinking [4]. These rates have decreased since 2010, when they were 61.4% and 40.5% in the 18–25 years age group for current alcohol use and binge drinking, respectively [4].
Tobacco: 11.8% of participants aged 12–20 years reported tobacco use (any method including tobacco products, cigarettes, or nicotine vaping) in the past month [4]. This rate has decreased from 35.7% in 2011, but nicotine vaping data was only included for the first time in 2020 [4]. 13.9% (17.5%) of participants in the 18–25 years age group reported current (in the past 30 days) cigarette use [4], which has also decreased from 34.3% in 2010 [4]. Vaping data were only collected in 2020 and indicated current use for 5.1% of adolescents 12–17 years old, and 11.7% of young adults 18–25 years old [4].
Marijuana: 34.5% (35.4%) of young adults, aged 18–25 years, reported using marijuana in the past year [4]. This has increased gradually over the past 10 years, with 30% of young adults using marijuana in 2010 [4].
Other illicit substances: 37% (39.1%) of young adults, age 18–25 years reported using illicit drugs in the past year [4]. This has increased since 2010, when 21.6% of young adults used illicit drugs in the past year [4].
Young AdultsThe CDC Behavioral Risk Factor Surveillance System (BRFSS) was established in 1984 to collect data about US residents regarding their health-related risk behaviors, chronic health conditions, and the use of preventative services [22]. The CDC conducts in-house interviewers and contracts with call centers or universities to administer the BRFSS surveys continuously throughout the year. The survey is conducted using Random Digit Dialing techniques on both landlines and cell phones. The latest data available is from 2020. In 2020, the sample size was 401,958 with a response rate of 47.9%, of which 25,652 (6.4%) were aged 18–24 years. Of note, the BRFSS data is stratified by age group, and the closest group to “young adults” is the 18–24 age group.
The most recent rates and trends for young adult substance use, as reported by the 2020 BRFSS are as follows (the BRFSS does not collect data on marijuana or illicit drug use) [22]:
Alcohol: 41.9% of young adults, aged 18–24 years old, reported having at least one drink of alcohol in the past 30 days, and 22% currently met the criteria for binge drinking [22]. The trend data indicates that current alcohol use (in the last 30 days) is down from 56.2% in 2011, and rates of binge drinking are also down from 29.9% in 2011 [22].
Tobacco: 8.3% of young adults, aged 18–24, currently smoked cigarettes [22], down from 22.3% in 2011. E-cigarette and vaping data are difficult to trend as data is only available for all adults 18 years and older for 2016 (4.7%) and 2017 (4.6%) [22].
Rates of Substance Use Among AYA with T1DIn the following section, we provide a brief description of each study included in Table 1. We then compare rates published by each T1D study to national surveys by age group. We considered the percentage of participants with reported use to be “similar” if they were within 10% of each other, and “lower” or “higher” if there was more than a 10% difference between the two percentages.
Studies Reporting Substance Use Rates Among AYA with T1DAlcohol and Marijuana Use and Treatment Nonadherence Among Medically Vulnerable Youth (Weitzman et al. [23])This paper describes a cross-sectional study of 403 adolescents (ages 9 to 18 years) with chronic medical conditions. The study assessed alcohol and marijuana use through self-report online surveys. Study staff recruited a convenience sample of 100 patients, each from 4 outpatient subspecialty clinics (1. type 1 diabetes; 2, juvenile idiopathic arthritis; 3, moderate persistent asthma or cystic fibrosis; and 4, ulcerative colitis or Crohn’s disease) at Boston Children’s Hospital during June 2013 to July 2015. The main findings were reported separately for youth with each medical condition. For the 100 youth with T1D (n = 100, M age = 16 ± 2.1), findings included that (1) rates of past year alcohol and marijuana were 34.9% and 23.8% respectively, and (2) alcohol use was associated with lower engagement in T1D treatment.
Prevalence of Tobacco Use and Association Between Cardiometabolic Risk Factors and Cigarette Smoking in Youth with Type 1 or Type 2 Diabetes Mellitus (Reynolds et al. [24])This paper is a cross-sectional, multi-center study that estimated rates of tobacco use in the past 30 days and the coexistence of cardiometabolic risk factors in 3466 AYA aged 10 to 22 years with T1D or T2D who participated in the SEARCH for Diabetes in Youth study from 2002 to 2005. Of the sample, 2887 AYA had T1D. Among AYA with T1D, current cigarette smokers were older with a longer duration of diabetes, more likely to be physically inactive, have higher HbA1c, and have lower household incomes than non-smokers. Smoking was associated with higher triglyceride levels and physical inactivity in AYA with T1D. Only 47.2 to 57.4% of AYA with T1D (rate depended on age group) reported having ever been counseled by their healthcare provider to not smoke or to stop smoking.
Alcohol Use Trajectories After High School Graduation Among Emerging Adults with Type 1 Diabetes (Hanna et al. [25])This paper describes a longitudinal, observational study that explored alcohol use trajectories during the year post-high school graduation among 181 AYA with T1D. Participants self-reported alcohol use via questionnaire at baseline and every 3 months for 1 year after high school graduation. Glycemic values were obtained from medical records around 41.8 days after the completion of the questionnaires. Three alcohol involvement categories best fit the longitudinal trajectory data based on latent class analysis: 1, consistent involvement group (13.8%) with stable, high use relative to other groups; 2, growing involvement group (30.4%) with increasing use; 3, minimal involvement group (55.8%) with no involvement until the ninth month. This study reported a lack of association between alcohol involvement with HbA1c. Those in the “minimal alcohol involvement” group also reported higher engagement in diabetes management and self-efficacy. Living independently of parents, having major life events, and having tried marijuana and cigarettes were identified as risk factors associated with the consistent alcohol involvement group. For the purposes of this review, we reviewed rates of substance use at baseline (for adolescents) and at the final data point (when participants were young adults).
Evaluating Substance Use and Insulin Misuse in Adolescents with Type 1 Diabetes (Snyder et al. [26])This cross-sectional study examined substance use and insulin misuse in 60 AYA with T1D aged 12 to 20 years old. Insulin misuse was described as chronic underdosing for purposes of weight loss or overdosing for euphoric sensation. Substance use and insulin dose questions were modeled from CDC YRBSS. The study found that older participants and those with diagnosed depression were more likely to use substances. Substance use and insulin misuse were not related to HbA1c or engagement in diabetes self-management behaviors in this sample.
Substance Use Among Adolescents and Young Adults with Type 1 Diabetes: Discussions in Routine Diabetes Care (Bento et al. [27])This observational study evaluated discussions of substance use in the clinic as well as self-reported substance use in 64 AYA aged 16–20 years with T1D. Participants completed select YRBSS questions at four visits, with 4–5 months between each visit in an outpatient pediatric diabetes clinic. Each visit was also audio-recorded to evaluate interactions between AYAs with T1D and their providers. Recordings were transcribed and coded to assess medical interactions. Despite many AYA reporting ever engaging in any kind of substance use (56.3% of the sample), only 5 patients or 8.5% had discussions about substance use during their most recent diabetes clinic visit.
Risk of Substance Use Disorders Among Adolescents and Emerging Adults with Type 1 Diabetes: a Population‐Based Cohort Study (Creo et al. [28])This retrospective chart review examined the incidence of substance use disorders and vaping among 230 AYA with T1D aged 12–25.9 years and compared them to age and gender-matched AYA without T1D from the same electronic medical record. The Rochester Epidemiology Project was used along with diagnosis codes to identify all those diagnosed with T1D between ages 12–25.9, over 9 years from January 1996 to December 2014. Substance use disorder diagnoses and vaping were restricted to before the patient’s 26th birthday to focus on events in the AYA population. The time-to-event analysis showed that the risk of incident substance use disorders was 1.7 times higher for those with T1D than those without T1D in this age group. When stratified by gender, group differences remained statistically significant in males, but not in females. There were too few cases of vaping for additional stratified analyses, emphasizing the need for further research on vaping in this population.
Alcohol Consumption Patterns in Young Adults with Type 1 Diabetes: the Search for Diabetes in Youth Study (Roberts et al. [29])This cross-sectional, multi-center study examined the alcohol consumption behaviors of 602 young adults (ages 18 to 25) with T1D via in-person SEARCH study visits from December 2011 to June 2015. Alcohol use was self-reported using the CDC BRFSS questionnaire. Participants were characterized as alcohol non-drinkers (n = 269, 44.7%), drinkers but non-binge drinkers (n = 167, 27.7%), or binge drinkers (n = 166, 27.6%). Risk factors for alcohol consumption identified by this study included being a current or former tobacco user, male, and 21 years or older.
Psychoeducational Messaging to Reduce Alcohol Use for College Students with Type 1 Diabetes: Internet-Delivered Pilot Trial (Wisk et al. [30])This intervention study examined drinking behaviors in 122 college students with T1D to determine the impacts of an alcohol use psychoeducational intervention delivered through web-based channels. This study compared the effects of an intervention delivered by either a peer or clinician narrator. All participants, despite the narrator differences, reported significant decreases in binge drinking. Participants across both groups increased in self-reported knowledge, health-protecting attitudes, and concerns regarding alcohol use. However, those who viewed a provider narrator were more likely to rate their narrator as trustworthy and knowledgeable. For this paper, we examined rates of alcohol use, as assessed at baseline.
Adolescents Only (Ages 12–17)Three of the reviewed studies (Weitzman et al., 2015; Reynolds et al., 2011; Hanna et al., 2014) included rates of substance use among only adolescents with T1D [23•] or provided data by age so we could report rates among adolescents and young adults separately [24, 25].
AlcoholRates of alcohol use in adolescents with T1D varied from 22% in the past 3 months [25] to 34.9% in the past year [23•]. Binge drinking for adolescents with T1D was reported solely by Weitzman et al. at 14.5% [23•]. In general, when compared to the national statistics, rates of current alcohol use among adolescents with T1D were similar in the Weitzman et al. study and lower in the Hanna et al. study. The Weitzman et al. study assessed alcohol use more similarly to the NSDUH (use over the last month); thus, the rates might be more comparable to the NSDUH data than the Hanna et al. study, which assessed alcohol use over the last 3 months.
TobaccoRates of tobacco use in the studies of adolescents with T1D varied widely from 2.4–17.3% in the past month [24] to 30% in the past 3 months [25]. Of note, as the age group increased, so did the rate of tobacco use across both studies. Rates in the 10–14 age group (2.4%) were much lower than the 15–19 (17.3%) group [24], and the 17–19 group (31.9%) [25]. When compared to the most similar national survey data, Hanna et al. found similar rates of use among adolescents with T1D, whereas Reynolds and colleagues (2011) reported lower rates compared to the same-age range on the NSDUH. However, the comparison between the NSDUH and Reynold’s sample is notably more robust, given the larger sample size of youth with T1D, and the similar timeframe assessed. The NSDUH assessed tobacco use over the last month, whereas Hanna et al. assessed the use over the last 3 months.
MarijuanaRates of marijuana use in adolescents with T1D varied between 17.1% in the past month [23•] and 23% in the past 3 months [25] to 30.9% in one’s lifetime [23•]. Compared to the NSDUH and YRBSS, rates reported by both Weitzman and colleagues (2015) and Hanna and colleagues (2014) were similar.
Illicit SubstancesNone of the identified studies examined illicit substance use in only adolescents with T1D.
Adolescents and Young Adults, Combined (Ages 12–20)Of the five studies that included participants spanning the adolescent to young adult age range, three of them (Snyder et al., 2016; Bento et al., 2020; Creo et al., 2021) did not examine these age ranges differently, and instead analyzed their whole group together (ages 12–20 years, 16–20 years, and 12–26 years, respectively). While Snyder et al. and Bento et al. had similar sample sizes with the same time intervals of measurement (past 30 days and lifetime), Creo et al. had a sample size about 4 times larger and was the only study that reported rates of substance use disorders in the AYA with T1D population. Since these three studies could not contribute to either the adolescent or young adult–only findings, we present their findings in this interim category of AYA, combined.
AlcoholRates of current alcohol use, within the last 30 days, varied from 18.3 to 37.5%, while lifetime use varied from 31.7 to 39.1% in AYA with T1D [26, 27•]. Rates of current alcohol use (within the last 30 days) were similar to the NSDUH rates, but lifetime rates of alcohol use were lower among AYA with T1D [26, 27•]. Creo and colleagues (2021) reported similar rates of alcohol substance use disorder in their sample of AYA with T1D compared to rates of past year alcohol abuse or dependence reported by the NSDUH for ages 12–25 years.
TobaccoRates of current tobacco use varied between the two studies from 6.25 to 11.7%, while lifetime use varied from 9.4 to 18.3% in AYA with T1D [26, 27•]. Snyder and colleagues (2016) reported that the current tobacco use among AYA with T1D was similar to that reported by the NSDUH, while Bento and colleagues (2020) reported a lower rate than the NSDUH. The rate of lifetime use was lower than that reported by the NSDUH for both studies. We were unable to compare the rate of tobacco and vaping substance use disorders reported by Creo and colleagues (2021) to the national survey data, because the NSDUH only provides data on alcohol and marijuana substance use disorders.
MarijuanaOnly Snyder and colleagues (2016) reported rates of marijuana use in AYA with T1D, with 5% having used marijuana in the past 30 days to 22% having ever tried it [26]. These rates are similar to those reported by the NSDUH. Creo and colleagues (2021) reported similar rates of marijuana substance use disorder in their sample of AYA with T1D compared to the past year of marijuana abuse or dependence reported by the NSDUH for ages 12–25 years.
Other Illicit SubstancesRates of illicit substance use in AYA with T1D varied from 0 to 7.8% in the past 30 days, to 1.7 to 17.2% in one’s lifetime [26, 27•]. Bento and colleagues (2020) reported rates that were consistently higher than Snyder and colleagues (2016) for both timeframes, within the past 30 days as well as lifetime use. It is possible that Bento and colleagues included marijuana in their definition of “illegal drugs,” considering they did not report on marijuana use separately, which resulted in higher rates than the Snyder et al. study. However, both studies were consistent with each other in that they reported rates of illicit substance use, in the past month and over one’s lifetime, that were lower than those reported by the NSDUH.
Young Adults Only (Ages 18–25)Four of the reviewed studies (Roberts et al., 2020; Wisk et al., 2021, Hanna et al., 2014; Reynolds et al., 2011) included rates of substance use among only young adults with T1D [29•, 30] or provided data by age so that we could report rates among adolescents and young adults separately [24, 25]. Hanna et al.’s 12-month follow-up data were used to report on young adult data.
AlcoholRates of alcohol use in young adults with T1D varied from 44% in the past 3 months [25] to 55% in the past 30 days [29•], to 82.8% in the past year [30]. Binge drinking in young adults with T1D was reported solely by Roberts et al. at 27.6% [29•]. Roberts and colleagues (2020) reported rates of current alcohol use (in the past 30 days) that were similar to those reported in the BRFSS and NSDUH. Hanna and colleagues (2014) reported similar rates of alcohol use in the past 3 months compared to the NSDUH for the past month. Of note, Hanna et al. (2014) are not as strong of a comparison due to the discrepancy in the timeframe assessed. The rate of binge drinking, reported by Roberts and colleagues (2020), was lower than that reported by NSDUH, but similar to the rate reported by the BRFSS. Finally, Wisk and colleagues (2021) reported a higher rate of alcohol use in the past year than that reported by NSDUH.
TobaccoRates of tobacco use in young adults with T1D varied from 23 [29•] to 31.9% [24] in the past 30 days, to 38% in the past 3 months [25]. The rate of current tobacco use (in the past 30 days) reported by Roberts and colleagues (2020) was similar to those reported by the BRFSS and NSDUH, but the rate of former tobacco use was higher than BRFSS. Hanna and colleagues (2014) reported similar rates of tobacco use in the past 3 months compared to the NSDUH’s for the past month. As noted above, this is not a strong comparison due to the discrepancy in the timeframe assessed. The Reynolds et al. (2011) study, which had a much larger sample size of youth with T1D, reported lower tobacco use rates in the past 30 days compared to the NSDUH national data.
MarijuanaOnly one study, Hanna et al. reported on marijuana use in the young adult population as 24% in the past 3 months [25]. This rate is similar to that reported by the NSDUH for the past month. But we should note, again, the discrepancy in the timeframe assessed.
Other illicit substancesNone of the identified studies examined illicit substance use in only young adults with T1D.
留言 (0)