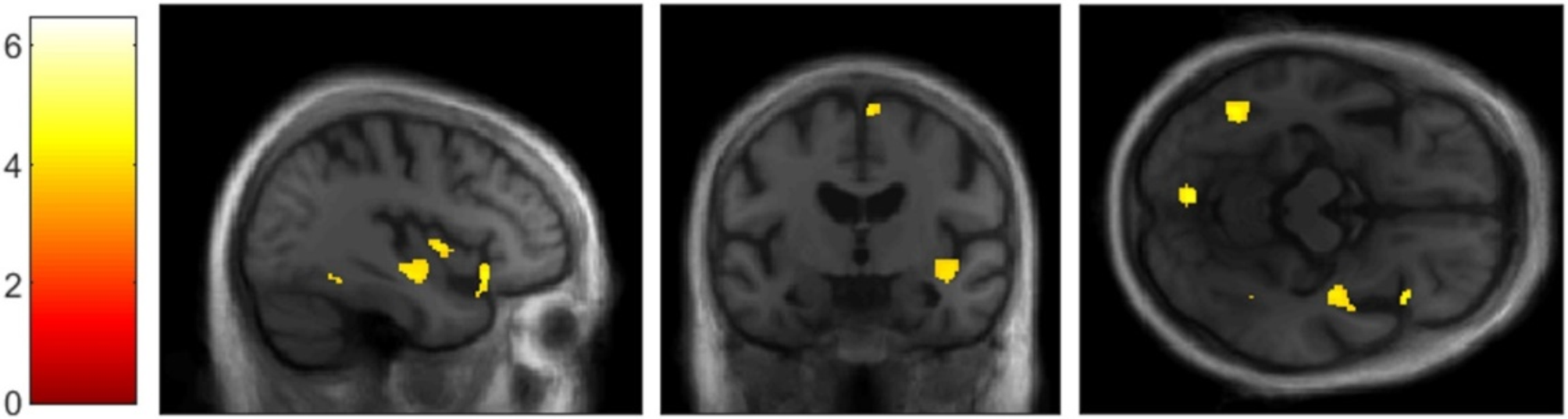
Glucose metabolism differed between patient groups, with the greatest and most extensive decreases—involving also frontal cortical regions and the caudate nucleus—in patients with right-predominant neurodegeneration of the ATL. Profiles of cognitive deficits differed slightly between patient groups, but direct comparisons did not reach significance in any of the tests applied. Mortality risk was six times higher in patients with right- than those with left-predominant ATL neurodegeneration. Median survival was shortest in the right- and longest in the left-predominant group.
In order to be able to characterize the biological entity of right ATL neurodegeneration, we did not use a clinical syndrome (e.g., SD, svPPA, or bvFTD) as an inclusion criterion. However, a considerable proportion of our RATL and LATL patient groups had the clinical picture of rtvFTD and svPPA, respectively.
Hypometabolism in patients with right-predominant neurodegeneration of the ATL was not restricted to this region but also involved regions outside the temporal lobe, particularly in the right frontal lobe. This finding is consistent with previously reported frontal atrophy in rtvFTD [6] and in right SD [7]. This frontal involvement might be reflected by greater behavioral disturbances in right compared to left SD [3]. Although behavioral symptoms were present in all three groups in our study, their prevalence was not statistically different between groups. This might be due to the small number of patients and the retrospective search for documented symptoms in clinical records.
SvPPA is usually associated with TDP-C neuropathology [21]. The topography of neurodegeneration in our patient group with left-predominant ATL neurodegeneration was very similar to that of svPPA patients [6], that of patients with TDP-C [22, 23], and that of PPA patients with TDP-C [24]. Importantly, hypometabolism was overall more widespread in the right-predominant group, which might indicate that patients with right-predominant neurodegeneration of the ATL have been examined at a later disease stage.
All three patient groups were impaired in the naming task of the CERAD-NAB. Consistently, metabolism of the left ATL, the region most tightly linked to naming difficulties [25,26,27,28], was decreased in all three groups compared to controls.
All patient groups were impaired in at least one of the typical memory tests (wordlist learning and recall, figure recall). This unexpected finding might be due to our inclusion criteria: As noted above, in previous studies clinical syndromes and hence the presence of specific symptoms were often among the inclusion criteria. The majority of related previous studies included only patients fulfilling the criteria for SD which is per definition associated with semantic rather than episodic memory deficits [13]. In contrast, the current study included all patients with ATL neurodegeneration irrespective of the kind of cognitive symptoms.
Cognitive performance differed only slightly between patient groups, and differences did not reach statistical significance. The lack of differences between patients with right-predominant and those with left-predominant neurodegeneration of the ATL contradicts previous reports on patients with greater right versus left ATL involvement [1,2,3,4,5,6]. It might be explained by examination of patients with right-predominant ATL neurodegeneration at a later disease stage, with neurodegeneration already involving the contralateral temporal lobe. This could have led to similar impairment of the group with right-predominant ATL neurodegeneration in naming and verbal memory, functions usually assigned to the left hemisphere.
The only impaired “right-hemisphere” function of the right-predominant group was figure recall, reflecting that the standard test battery used here does not contain the most sensitive tests to detect right ATL degeneration (e.g., recognition of famous faces was not tested).
Survival durations were 5.7 to 8.3 years (patients with right- and left-predominant ATL neurodegeneration, respectively) after PET imaging. From clinical experience, it is our impression that PET imaging is usually performed close to the time of diagnosis, and hence, we compare the survival durations of our study to the literature that reported survival durations from the time of diagnosis. Importantly, whereas the median survival duration of patients with left-predominant ATL neurodegeneration fits previous results from studies in SD (8 to 10 years [12]) and svPPA (9 years [9]), median survival of the right-predominant group was closer to previous figures from bvFTD (4 years [8]; 5 years [9]). Therefore, patients with right-predominant neurodegeneration of the ATL have in common with bvFTD not only frontal neurodegeneration (see Fig. 2), but also a particularly short survival. The observed shorter survival of the right-predominant ATL group might be due to a faster progressing underlying disease. While it might be assumed that right ATL neurodegeneration is most often due to TDP-C neuropathology, as is left ATL neurodegeneration (and svPPA) [21], Josephs et al. reported tauopathies among patients with rtvFTD, particularly in patients whose atrophy pattern also involved the frontal lobe [29].
Mesulam and colleagues recently reported that among PPA patients, those with underlying TDP-A have a shorter survival after symptom onset than those with TDP-C neuropathology (median 6 vs 14 years, respectively) [24]. In our patient sample, neuropathology and hence the proportion of TDP-A cases are unknown. However, the reported atrophy pattern of TDP-A, with equal temporal, frontal, and parietal involvement [24], more closely resembled that associated with Alzheimer’s disease than TDP-C. Patients with such a pattern of neurodegeneration (on FDG PET) were not included in our study (see inclusion criterion 2).
An additional survival analysis of our data with survival duration computed from estimated time of symptom onset yielded no significant group difference. The observed shorter survival from the time of FDG PET but not from the time of symptom onset might indicate that patients with right-predominant were admitted to FDG PET later in the disease course than those with left-predominant ATL neurodegeneration.
Taken together, greater hypometabolism, similar cognitive impairment, and shorter survival in our view indicate that patients with right-predominant neurodegeneration of the ATL were examined at a later disease stage. Although symptom durations (from patient records) in our study did not statistically differ between patient groups, it has to be noted that symptom durations have only been estimated retrospectively at the time of clinical visit by patients and/or caregivers, which might bear considerable inaccuracy. As discussed by Chan et al. [5], the (initially) rather non-verbal nature of symptoms in patients with rtvFTD (and right-predominant ATL neurodegeneration) might lead to a delayed recognition of symptoms, which is in line with a report on later recognition and delayed therapy of right hemisphere compared to left hemisphere stroke [30]. Similarly, it has been shown that among patients with syndromes associated with frontotemporal lobar degeneration, those with svPPA receive the diagnosis of a neurodegenerative syndrome much earlier than all others, e.g., bvFTD patients [9].
Limitations
Sample sizes were small in this retrospective, mono-centric study. Owing to the long time span during which FDG PET were acquired, different PET scanners were used. We tried to cope with this with different smoothing filters in image preprocessing and by including PET scanner as a covariate in statistical analyses. Patient selection in this study was based on imaging findings. It was neither based on clinical diagnoses, nor based on neuropathological findings (although all available amyloid PET were negative). It is hence possible that patients with non-neurodegenerative etiologies have been included. From all data presented here, we assume, however, that most included patients fall in the clinical spectrum of FTD and have a TDP-43 neuropathology, most likely TDP-C.

留言 (0)