
記住我
An ounce of prevention is worth a pound of cure
Benjamin Franklin
Postoperative atrial fibrillation (POAF) is a frequent complication in patients undergoing cardiac surgery, and its prevention is still troubling.1 Indeed, POAF is, up to the present time, the most prevalent secondary atrial fibrillation (AF), affecting approximately one-third of patients after cardiac surgery.2 Notably, POAF often occurs even after noncardiac surgery.3
POAF increases surgery complications burden and correlates with worse outcomes over time.4 POAF is also linked with rising hospital costs, prolonged intensive care unit, and hospitalization time.5 POAF affects both patients with pre-existing episodes of AF and naïve patients; in this last case, predictors of new-onset AF are age ≥65, anemia, history of heart failure, and valvular heart disease.2 Pre-existing atrial remodeling added to the surgical stress, ischemia, use of cardiopulmonary bypass, and reperfusion stress are the key elements in POAF multifactorial pathogenesis.1,6 It is worth to mention also inflammation and adrenergic activation, factors that may trigger AF in a vulnerable atrial substrate, enhancing the formation and activation of reentry circuits.1
For that reason, POAF prevention is still debated and troublesome. Numerous studies on β-blockers prophylaxis have shown efficacy in reducing POAF events; indeed, this is the most common prevention strategy, and international guidelines also recommend it.7,8 Many other medications were used in POAF prophylaxis management, such as amiodarone, corticosteroids, and statins, with unsatisfactory or unclear findings.1 Some studies also explored the function of perioperative infusion of human atrial natriuretic peptide (also known as carperitide) in patients undergoing coronary artery bypass grafting (CABG) with the use of cardiopulmonary bypass, finding a significant reduction of POAF.9,10 Nevertheless, the role of other natriuretic peptides (NP), such as recombinant human brain natriuretic peptide (rh-BNP), was not explored, and there is a lack of evidence in this field.
 FIGURE 1.:
FIGURE 1.: Role of rh-BNP in postoperative atrial fibrillation. Rh-bnp, recombinant human brain natriuretic peptide; pt, patients; CABG, coronary artery bypass grafting; RCTs, randomized controlled trials.
Natriuretic peptides are 3 biologically active molecules: atrial natriuretic peptide (ANP), brain natriuretic peptide (BNP), and C-type natriuretic peptide (CNP). In particular, the heart secretes ANP and BNP, and these hormones bind specific receptors, mediating an inhibitory effect on renin–angiotensin–aldosterone system. This is the reason why NP or agents capable of inhibiting neprilysin (a proteolytic enzyme involved in the degradation and inactivation of ANP and BNP) are used as therapeutic strategies against heart failure.11 A clear and strong example of inhibition of this pathophysiological pathway is sacubitril use in heart failure, an inhibitor of neprilysin which, combined with valsartan, has proved safe and effective in reducing mortality and hospitalization.12
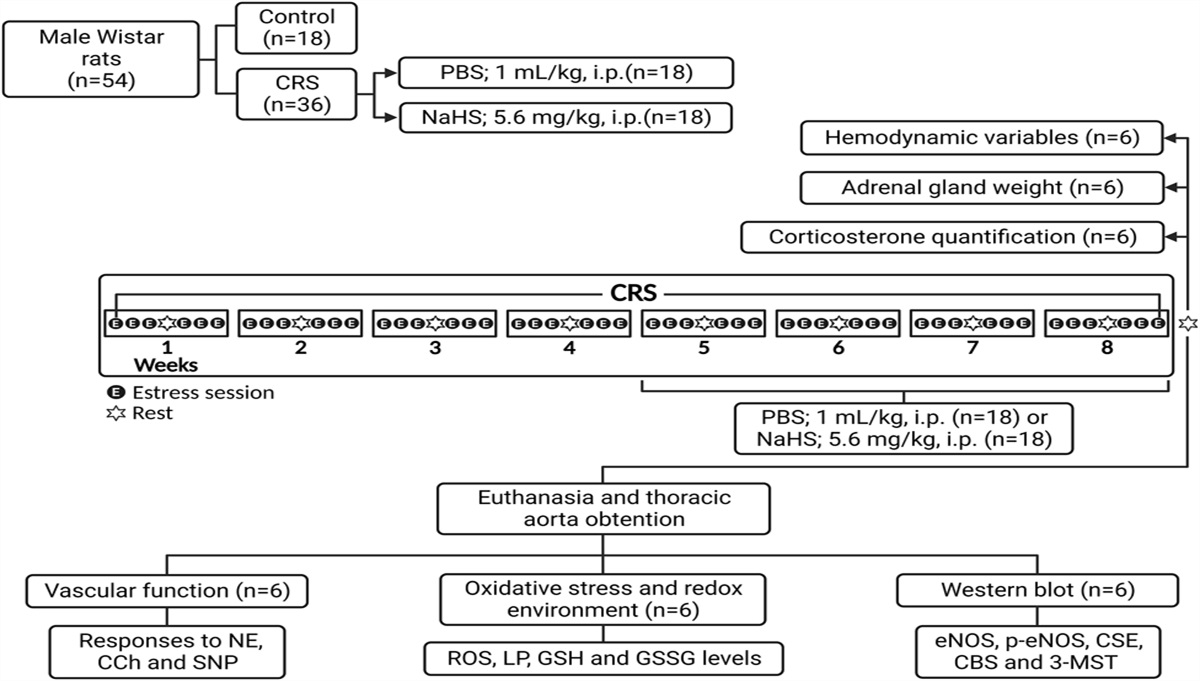
In the current issue of the Journal, Yangyan Wei et al13 aimed at appraising in a retrospective cohort study the role of rh-BNP in decreasing POAF (Fig. 1). Researchers have consecutively included in the retrospective analysis 1153 patients who underwent isolated CABG between 2018 and 2021 in the Affiliated Hospital of Qingdao University.
Two groups were identified: patients receiving rh-BNP and patients without rh-BNP. Rh-BNP was given to patients with cardiac insufficiency before surgery, diuretic resistance after surgery, or acute kidney injury. Physicians empirically defined rh-BNP doses. Thus, patients in the rh-BNP cohort were more critical, needed higher doses of inotropic support before and after surgery, and had a lower ejection fraction and greater body mass index. The authors applied propensity score matching to obtain 2 balanced groups. After propensity score matching, 53 patients from the rh-BNP group were compared with 148 patients from the non rh-BNP group. The major finding was that in the rh-BNP group the incidence of POAF was significantly lower than in the non rh-BNP group (18.9% vs. 37.2%, OR = 0.393, 95% CI 0.183–0.845, P = 0.017). Interestingly, rh-BNP usage seemed not to be associated with postoperative hypotension, mortality, or ventricular arrhythmias, maintaining an optimal safety profile.
Despite significant limitations, such as the single retrospective cohort design of the study, we should enthusiastically welcome Yangyan Wei et al insights against such a frequent surgery complication. Notably, the precise function of natriuretic peptides in preventing POAF needs to be further investigated, conceivably by designing randomized clinical trials, including patients from different centers worldwide.
Reasonably, BNP could prevent POAF by decreasing hemodynamic atrial stress; indeed, the action of NP is involved in the reduction of blood volume, blood pressure, and aldosterone, which contribute to atrial pathological remodeling.14 Therapeutic use of NP should also be explored in other settings, including patients undergoing valvular surgery, off-pump procedures, and percutaneous coronary interventions, which may benefit from these findings.15,16
We hope this study could be an encouraging step to improve the management of POAF prophylaxis and to track a new line of research on rh-BNP, whose effects may spread to a wide range of clinical settings.
1. Dobrev D, Aguilar M, Heijman J, et al. Postoperative atrial fibrillation: mechanisms, manifestations and management. Nat Rev Cardiol. 2019;16:417–436. 2. Greenberg JW, Lancaster TS, Schuessler RB, et al. Postoperative atrial fibrillation following cardiac surgery: a persistent complication. Eur J Cardiothorac Surg. 2017;52:665–672. 3. Kalra R, Parcha V, Patel N, et al. Implications of atrial fibrillation among patients with atherosclerotic cardiovascular disease undergoing noncardiac surgery. Am J Cardiol. 2020;125:1836–1844. 4. Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after cardiac surgery. Ann Intern Med. 2001;135:1061–1073. 5. Greenberg JW, Lancaster TS, Schuessler RB, et al. Postoperative atrial fibrillation following cardiac surgery: a persistent complication. Eur J Cardiothorac Surg. 2017;52:665–672. 6. Zakkar M, Ascione R, James AF, et al. Inflammation, oxidative stress and postoperative atrial fibrillation in cardiac surgery. Pharmacol Ther. 2015;154:13–20. 7. Arsenault KA, Yusuf AM, Crystal E, et al. Interventions for preventing post-operative atrial fibrillation in patients undergoing heart surgery. Cochrane Database Syst Rev. 2013;2013:CD003611. 8. Dunning J, Treasure T, Versteegh M, et al.; EACTS Audit and Guidelines Committee. Guidelines on the prevention and management of de novo atrial fibrillation after cardiac and thoracic surgery. Eur J Cardiothorac Surg. 2006;30:852–872. 9. Sezai A, Hata M, Wakui S, et al. Efficacy of continuous low-dose hANP administration in patients undergoing emergent coronary artery bypass grafting for acute coronary syndrome. Circ J. 2007;71:1401–1407. 10. Sezai A, Iida M, Yoshitake I, et al. Carperitide and atrial fibrillation after coronary bypass grafting: the Nihon University working group study of low-dose HANP infusion therapy during cardiac surgery trial for postoperative atrial fibrillation. Circ Arrhythm Electrophysiol. 2015;8:546–553. 11. Nakagawa Y, Nishikimi T, Kuwahara K. Atrial and brain natriuretic peptides: hormones secreted from the heart. Peptides. 2019;111:18–25. 12. McMurray JJ, Packer M, Desai AS, et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371:993–1004. 13. Wei Y, Zhang Q, Chi H, et al. Effects of recombinant human brain natriuretic peptide on atrial fibrillation after coronary artery bypass grafting. J Cardiovasc Pharmacol. 2022. In press. 14. D'Elia E, Iacovoni A, Vaduganathan M, et al. Neprilysin inhibition in heart failure: mechanisms and substrates beyond modulating natriuretic peptides. Eur J Heart Fail. 2017;19:710–717. 15. Chiariello GA, Villa E, Messina A, et al. Dislocation of a sutureless prosthesis after type I bicuspid aortic valve replacement. J Thorac Cardiovasc Surg. 2018;156:e87–89. 16. Nardi P, Pellegrino A, Bassano C, et al. The fate at mid-term follow-up of the on-pump vs. off-pump coronary artery bypass grafting surgery. J Cardiovasc Med. 2015;16:125–133.
留言 (0)