
記住我
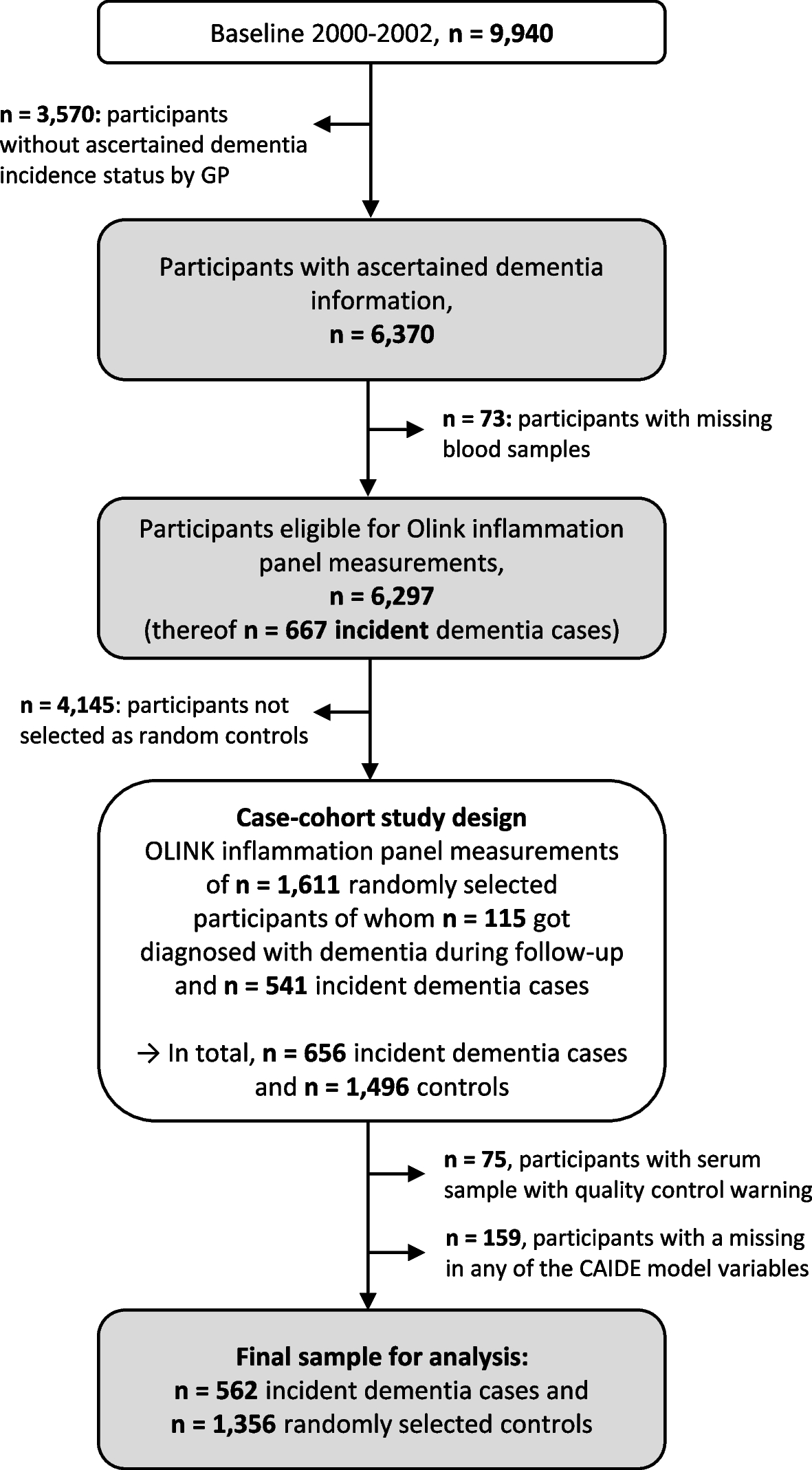
This study was a cohort study. Data were derived from the Tianjin Elderly Nutrition and Cognition (TENC) cohort study (registration identifier: ChiCTR2000034348). The TENC cohort study was conducted in the subjects aged 60 years or older and resided in the Baodi District of Tianjin, China. The sampling method in the TENC cohort study was multistage cluster sampling. In total, 5,577 eligible subjects from these communities were identified from March 2018 to June 2019. Those who were willing to participate were surveyed with a response rate of 88.60% (n = 4,933). All participants received a personal interview and a general physical examination by trained interviewers. The follow-up study was performed from March 2021 to June 2021. A total of 1,455 individuals were excluded from this analysis based on the following criteria: history of Parkinson's disease (PD), AD and stroke, which were clinically diagnosed by physician (n = 130); MCI at baseline (n = 391); missing demographic information (n = 74); abnormal total energy intakes (i.e., daily energy intake <800 kcal/day or >4800 kcal/day for male and <500 kcal/day or >4000 kcal/day for female, n = 453); and loss to follow-up (n = 407). Finally, a total of 2,944 individuals were included in this study (Figure 3). The study protocol was approved by the Ethics Committee of Tianjin Medical University (approval number: TMUhMEC2018013), and all participants provided informed consent before participation. All procedures in this study were conducted according to the Declaration of Helsinki.
Fig 3.
Flow diagram of the study process. Abbreviations: FFQ, food frequency questionnaires; PD, Parkinson's disease; AD, Alzheimer’s disease; MCI, mild cognitive impairment; DII, dietary inflammation index; LTL, leukocyte telomere length; mtDNAcn, mitochondrial DNA copy number
Definition of MCIDiagnosis of MCI was based on the modified version of Petersen's criteria as previously described [36]: (i) subjective memory complaints over at least 6 months, preferably confirmed by an informant; (ii) Mini-Mental State Examination (MMSE) score of ≤ 17 points for illiterate people, ≤ 20 points for primary school level education, and ≤ 24 points for secondary education level and above; (iii) absence of dementia, AD, psychiatric disorders, cerebral damage or other physical diseases resulting in cognitive impairment; and (iv) little or no difficulty in activities of daily life, measured by the Activities of Daily Living Scale (ADL; <26 points). MCI patients had to meet all of these four criteria.
Dietary assessmentThe dietary assessment of participants was performed using a validated, simplified, and quantitative food frequency questionnaire (FFQ) that included 30 food items. Based on the FFQ, participants were required to recall their consumption frequencies and average amounts for the past 3 months. The frequency of each food item included 7 frequency categories as follows: (1) rarely eat or drink; (2) less than 1 time per week; (3) once a week; (4) 2-3 times per week; (5) 4-6 times per week; (6) once per day; and (7) twice or more per day. The consumption frequency of each food item was converted to daily intakes. According to the similarity of nutrient profiles and culinary usages among the foods and the grouping scheme used in other studies, we collapsed 30 food items into 20 predefined food groups. Information on frequency of intake and portion size were used to calculate the amount of each food item consumed on average, using the China Food Composition Table as the database.
Calculation of DII scoreThe details of DII were available elsewhere [37]. Briefly, the dietary data for each study participant was first linked to the regionally representative global database of dietary surveys from 11 countries for each of the 45 parameters (i.e., foods, nutrients, and other food constituents). This global database provides a robust estimate of a mean and standard deviation for each of the food parameters considered. A z-score was derived by subtracting the “standard global mean” from the amount reported and then dividing this value by the standard deviation. This value was then converted to a centered percentile score, which was then multiplied by the respective food parameter inflammatory effect score to obtain the subject’s food parameter-specific DII score. All of the food parameter-specific DII scores were then summed to create the overall DII score for each participant. In the current study, DII score was calculated based on 24 available food parameters, which were as follows: energy, carbohydrate, protein, total fat, saturated fatty acids, monounsaturated fatty acids, polyunsaturated fatty acids, fiber, cholesterol, niacin, thiamine, riboflavin, folate, vitamin A, β-Carotene, vitamin C, vitamin E, iron, magnesium, selenium, zinc, isoflavones, alcohol, and anthocyanidins. To control the influence of total energy intake, we calculated the energy-adjusted version of the DII per 1000 calories of food consumed.
Measurements of LTL and mtDNAcnIn the present study, LTL and mtDNAcn were determined using quantitative real-time polymerase chain reaction (q-PCR) method. The relative telomere length was calculated by the telomere to single-copy gene ratio. The mtDNAcn was calculated by the ND1 to single-copy gene ratio. The hemoglobin (HGB) gene was used as the reference gene (single-copy gene) for both LTL and mtDNAcn. All reactions were performed on a Roche LightCycler® 480 machine (Roche, Manheim, Germany) in the same lab. Each reaction was performed in triplicate and expressed as 2(−ΔΔCt).
Measurements of immunity markersBlood samples were used to assay full blood count immediately after the blood draw. These measurements (including absolute counts of neutrophils, platelets lymphocytes, and monocytes) were performed using an Olympus AU5811 clinical chemistry analyzer (Tokyo, Japan) with standard laboratory techniques. The SII was defined as (P*N)/L and SIRI was defined as (N*M)/L, where N, M, and L represent the counts of peripheral neutrophil, monocyte, and lymphocyte, respectively. Enzyme-linked immunosorbent assay (ELISA) was applied to detect the inflammatory cytokines using MILLIPLEX®MAP Kit obtained from EMD Millipore Corporation (Billerica, MA).
Genotyping of APOE ε4 alleleGenomic DNA was extracted from fasting venous EDTA blood using the QIAamp DNA Mini Kit (Spark Jade Science Co., Ltd, Shandong, China). Genotypes were determined via the Custom Taqman SNP Genotyping Assay by sequencing rs429358 (codon 112) and rs7412 (codon 158) at exon 4 of the APOE polymorphism, with the technical support of Shanghai OE Biotech Company.
CovariatesDemographic and clinical characteristics as well as lifestyles were collected using a structured questionnaire. The demographic data included age, sex, educational levels, medical history, smoking status, alcohol consumption status. Physical activity (PA) was measured using a short version of the International Physical Activity Questionnaire (IPAQ), which reported as metabolic equivalent hours per day (METs-h/day) [38]. Body mass index (BMI) was measured by weight (kg)/height (m2). APOE polymorphism status was dichotomized as APOE ε4 carriers or non-carriers.
Statistical analysisContinuous variables were expressed as means ± SDs or medians (IQRs) based on the test of normality. Categorical variables were shown as frequencies (percentages). Normality of continuous variables was assessed using the Skewness-Kurtosis test. An independent-samples t-test was conducted for continuous variables and the chi-square test was used for categorical variables to compare the differences between those with and without MCI in all characteristics. Tertiles for DII were defined as follows: first tertile, less than -1.02 (T1); second tertile, -1.02~0.96 (T2); and third tertile, more than 0.96 (T3). Cox proportional hazard regression was performed to analyze the longitudinal associations of DII, immunologic parameters, LTL, and mtDNAcn with MCI. Results were presented as hazard ratios (HRs) and 95% confidence intervals (CIs). Linear regression analysis was performed to explore the relationships between DII, immunologic parameters, LTL, and mtDNAcn. Results were presented as β-coefficients with 95% CIs. Model 1 was crude model; Model 2 adjusted for age, sex, BMI, smoking, alcohol consumption, history of hypertension, diabetes and hyperlipidemia, and total PA at baseline. Model 2 further adjusted for APOE ε4 carrier status when detecting MCI-related associations. Ordinal variables were not set to dummy variables, but as continuous variables to test the monotonic (upward or downward) trend (P for trend). The path analysis was performed using the procedures PROC REG and PROC CALIS from SAS 9.4. A nested case-control study was designed within the TENC cohort as a sensitivity analysis. For the nested case-control study, we matched up to two controls to each recurrent MCI patient following to the difference between case and control in age ≤ 3 years, and with the same sex and follow-up period. The nested case-control study repeated all analyses using inflammation cytokines as indicator of inflammation instead of immune cells to validate the primary findings of cohort. Paired t-test and conditional logistic regression were used to compare the differences between case and control in all characteristics and obtain odds ratio (OR) and 95% CI of inflammation cytokines on MCI, respectively.
All analyses were performed using SPSS Version 25.0 (SPSS Inc., Chicago, IL, USA) and SAS version 9.4 (SAS Institute, Inc.). A two-sided P value< 0.05 was considered to be statistically significant.
留言 (0)