
記住我








The population of this study included patients who were diagnosed with GC and developed VTE complications during treatment in the Affiliated Cancer Hospital of Zhengzhou University from 2017 to 2021. The inclusion criteria were: 1) age over 18 years old; 2) histological diagnosis of gastric cancer; 3) having received antitumour treatment in our hospital for more than 4 weeks; 4) VTE occurred during the treatment and was clearly diagnosed and treated with antithrombotic therapy. Patients who had VTE or received chronic anticoagulation therapy before the diagnosis of GC were excluded.
We selected paraffin sections of the cancer tissues of the enrolled patients for FISH of F. nucleatum and confirmed the positive and negative results. From these patients' electronic medical records, we extracted demographic variables and treatment variables, including radiotherapy, surgery, and chemotherapy. The specific variables of cancer included presentation state, stage, histological type, and whether distant metastasis occurred at diagnosis. For the sake of comparison, we divided the stages into early, middle, and late stages, corresponding to stage I, stage II-III, and stage IV, respectively (the majority of the patients were in stage IV), the histological types into adenocarcinoma and nonadenocarcinoma, and the ECOG score (used to evaluate the patient's performance status) into 0 and ≥ 1. Given the low body weight of GC patients in Asia, we defined BMI > 25 kg/m2 as obesity. We also obtained clinical and biochemical data related to mortality, especially the Khorana VTE risk score (KRS), platelet-lymphocyte ratio (PLR), and neutrophil–lymphocyte ratio (NLR). According to the normal value range, biochemical indicators were defined as increased when they were above the upper limit (High) and decreased when they were below the lower limit (Low) (Table S1). According to the KRS standard, 0 is low risk of VTE, 1–2 is medium risk, and ≥ 3 is high risk (Table S2). We used the previously defined PLR > 260 and NLR > 3 as the critical values to distinguish the high and low risks of VTE. We also extracted the data of targeted drugs and PD-1 used that may affect the prognosis. Regarding the data of VTE occurrence and treatment, we selected the time of VTE occurrence (the time from diagnosis of GC to VTE occurrence as a continuous variable, and the time of VTE occurrence during chemotherapy or surgery was classified into four categories), location (including DVT, PE, splanchnic vein thrombosis (SVT) (Table S3), and catheter-related thrombosis), antithrombotic therapy (including thrombolysis, inferior vena cava (IVC) filter placement, low molecular weight heparin (LMWH), and direct oral anticoagulants (DOACs)), and whether there was bleeding during treatment. The above data were maintained and provided by our hospital's radiology department, ultrasound department and medical record room.
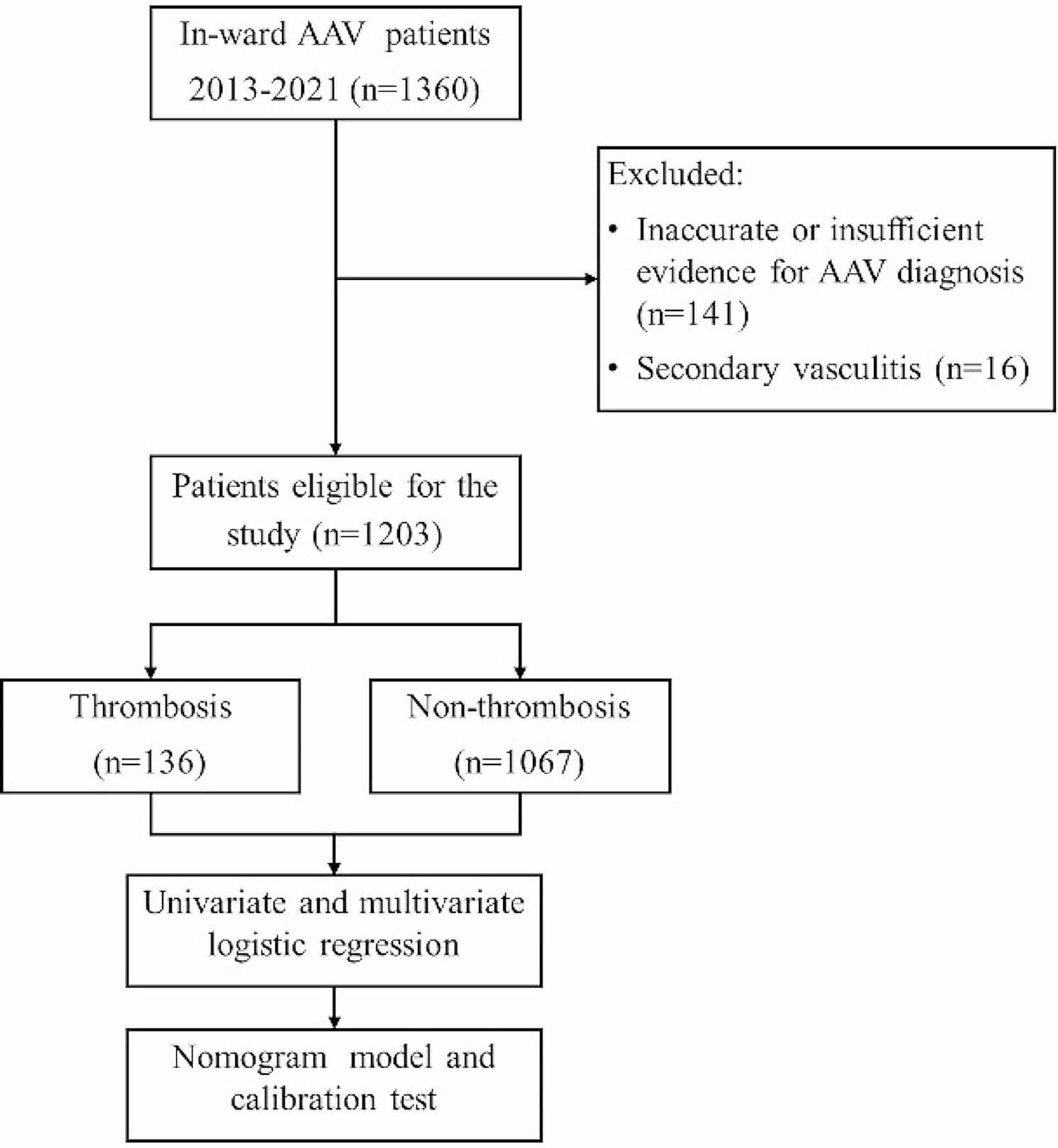
Outcome measureThe main outcome was overall survival (OS), that is, the survival time from the diagnosis of GC to death (or the last follow-up). VTE includes symptomatic or accidental DVTs in the upper and lower limbs, PE, SVTs, and catheter-related thromboses. All selected patients with VTE were confirmed by Doppler ultrasound, computed tomography (CT), CT angiography or ventilation perfusion scanning. From January 1, 2017, to March 31, 2021, a total of 359 eligible patients were enrolled. Among them, 304 patients completed the follow-up during the study period, while 55 patients were lost to follow-up because they did not receive treatment for VTE and changed to other medical institutions during the treatment (Fig. 1).
Fig. 1
Flow diagram of selection of patients
Fluorescence in situ hybridization (FISH)F. nucleatum was detected in formalin-fixed paraffin-embedded tissues by FISH. The tissue slides (4 µm) were then deparaffinized at 60 °C, followed by treatment with 100% xylene for 20 min and a graded series of ethanol at room temperature. The slides were incubated with a denatured, Cy3-labelled F. nucleatum probe (5 ng/μL) at 37 °C for 18 h. After five washes, the cell nuclei were stained with DAPI. Images were captured on a confocal microscope (LSM800, Zeiss), and the number of F. nucleatum signals was counted. Five random 100 × fields were chosen for evaluation by two pathologists blinded to tumour/normal status. The sequence for the F. nucleatum probe was 5’-CGCAATACAGAGTTGAGCCCTGC-3’ (Fig. 2).
Fig. 2
FISH results of F. nucleatum in paraffin sections of 304 GC patients complicated with VTE showed that 199 cases were negative and 105 cases were positive. The photos were taken at 10 × and 100 × of the objective lens
Statistical analysisThe patients included in the analyses were divided into two groups according to their FISH results of F. nucleatum, namely, positive and negative groups. The continuous variables are presented as the median and interquartile range (IQR), while the categorical variables are expressed as the number and percentage (%). The t test, Mann‒Whitney U test, Chi-square test, or Fisher's exact test were applied to detect the differences between the positive and negative groups when appropriate.
The Kaplan‒Meier method was employed to estimate the median survival time (MST) and survival curves, and the significant differences between survival probabilities were formally evaluated by the log-rank test. To identify the possible influencing factors on the prognosis of GC, a Cox proportional hazard model was constructed between covariates and the outcome. Specifically, univariate Cox regression was first conducted for each covariate, and those variables with a P value of less than 0.1 were considered potential prognostic factors for mortality. Furthermore, a stepwise multivariate Cox regression with a widely used backwards selection procedure was constructed on those variables to assess the adjusted risk of mortality for each factor. The final results were expressed as hazard ratios (HRs) with 95% confidence intervals (95% CIs), and factors with HRs higher than 1 increased the risk of mortality. Similarly, univariate and multivariate logistic regressions were applied to explore the potential influencing factors associated with F. nucleatum colonization. To avoid the possible impact of multicollinearity, which could bias the estimations of the multivariate Cox model, we additionally calculated the generalized variance inflation factor (GVIF) for each included variable. Those variables with GVIF larger than 2.24 were removed [11]. We did not impute any missing values in the original data, and P < 0.05 (two-sided) was considered statistically significant. All analyses were conducted in R software (Version 4.1.2).
留言 (0)