
記住我

The principles of the Declaration of Helsinki for the research with human subjects involved were followed, and the study was approved by the Institutional Ethics Committee (CEI21-001). VISSUM Innovation (Cornea, Cataract and Refractive Surgery Unit, Alicante, Spain), Keratoconus IBERIA databases (Universidad Miguel Hernández de Elche, Elche, Spain) and Bioengineering and Applied Computational Simulation Research Group databases (Universidad Politécnica de Cartagena, Cartagena, Spain) contributed data for the study.
This retrospective non-randomized cross-sectional study was conducted at VISSUM Innovation and comprised consecutive 99 non-DS subjects with KC (99 eyes) and age- and sex- matched 43 DS patients (43 eyes) with genotypic confirmation, who were examined between 2017 and 2019.
One eye was selected for statistical analysis in bilateral cases using randomization function of the Statistical Package for Social Sciences (SPSS) version 24 software (IBM SPSS Statistics Inc., Chicago, IL, USA). Eyes with history of surgery, hydrops, corneal trauma, scarring, infection, and unacceptable quality of the topographic test (score < 90%) were excluded.
All participants underwent a detailed ophthalmological examination and anterior segment tomography (Sirius System®, CSO, Firenze, Italy). Topography measurements were performed by a single experienced optometrist for three times for each eye and the one with the highest coverage and centration scores over 90% with a green checkmark was used for further analysis.
Contact lens wearers were requested to remove their contact lenses for 2 (for soft lens) and 4 weeks (for hard lens) prior to the measurements.
Two cornea specialists performed clinical and topographical examinations (JLA and JADB). To avoid bias, the Sirius System® topographic classifier outputs (as “Normal,“ “KC suspect,“ “KC compatible,“ and “Abnormal or treated”) were validated by two observers with consensus. Following criteria were used to confirm the KC diagnosis; presence of typical biomicroscopic and retinoscopic signs of KC (if any) such as Rizzuti’s phenomenon, Fleischer’s ring, scissoring, Vogt’s striae, Munson’s sign and and/or any typical pattern for KC on axial/tangential curvature map [superior steep, inferior steep, irregular, oval, round, inferior-steep and superior-steep asymmetric bowtie, symmetric or asymmetric bowtie with skewed radial axes (SRAX) > 22 degrees and inferior-superior (I-S) keratometric asymmetry ≥ 1.5 D] and coexistence of central/paracentral or inferior focal steepening (anterior and/or posterior) with corresponding corneal thickness reduction. All measurements were performed following the standard operative procedures defined by the EVICR.net for the corneal topography examination and performed by personnel certified in Good Clinical Practices.
The Sirius System® classifier report was also considered; borderline topographical alterations were considered “KC suspect” when they did not comply with the above-mentioned KC criteria. Topographical findings that did not match any sort of corneal ectasia pattern were considered “Abnormal or treated”. Topographical maps those lacked any of the above-mentioned abnormalities were defined as “Normal”.
Based on topographical categorization, the overall DS group was categorized into two subcategories: DS with KC topography (eyes with topographic classification of “KC compatible” and “KC suspect”), and DS with non-KC topography (eyes with topographic classification of “Abnormal or treated” and “Normal”).
The non-DS and DS groups were compared in terms of age, gender, spherical equivalent, central corneal thickness (CCT), high-order corneal aberrations (HOA), and 3D morphogeometric and volumetric parameters.
Patient-specific 3D corneal modelling & morphogeometric parametersThe patient-specific 3D corneal model used to determine the morphogeometric parameters used in this study was generated directly from the raw data acquired by the Sirius tomographer (clouds of topographical points that define anterior and posterior corneal surfaces), following a procedure created by Cavas and colleagues [14], that has been validated and has also already been applied to the diagnosis of KC [16, 17], to the detection of subclinical keratoconus [15] and to the study of the evolution of invasive treatments on corneal ectasias [18] in several previous studies.
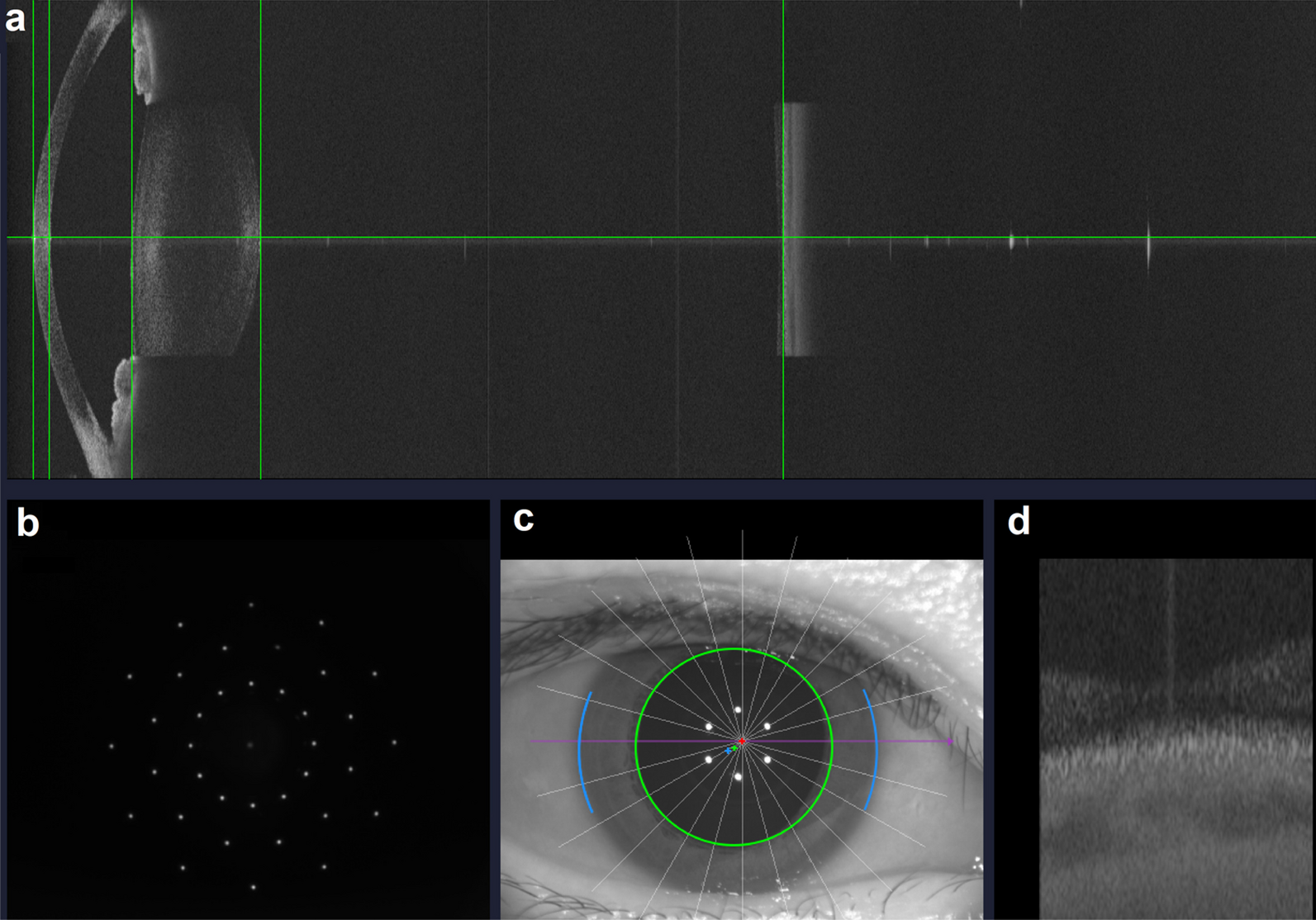
The procedure consists of two well-differentiated phases (Fig. 1): an initial one in which the tomographical data is obtained, followed by a final one in which 3D model is generated and a morphogeometric analysis is made to determine several linear, surface, volumetric and/or angular parameters. A detailed description of both the procedure and the definition of the main morphogeometric parameters can be found in [14].
Fig. 1
Scheme of the procedure used to study the similarity between Down syndrome (DS) and non-DS corneas
Statistical analysisA minimum sample of 40 eyes per group was needed (DS and non-DS KC groups) at 95% power and 95% confidence level with an effect size (d) of 0.78 (GPower v0.3.1.9.6, Universität Düsseldorf, Düsseldorf, Germany).
After completing the study, statistical power was re-calculated based on the comparisons among non-DS KC group (n = 99), DS with KC topography (n = 16) and DS with non-KC topography (n = 27) groups and was found to be 90.6% (GPower v0.3.1.9.6, Universität Düsseldorf, Düsseldorf, Germany).
SPSS version 24 (IBM SPSS Statistics Inc., Chicago, IL, USA) was the software selected for statistical analysis. The Chi-square test was selected for comparison purposes with qualitative data (gender) between groups. The Kolmogorov-Smirnov test was conducted to ensure that the variables had a normal distribution. Age, volumetric, morphogeometric, aberrometric, pachymetric and refractive data were represented as mean ± standard deviation (SD). When the parametric test assumptions were fulfilled, a t-test for independent samples (Student’s t-test, two-tailed) was used for quantitative data comparison purposes between both non-DS and DS groups. The Mann-Whitney U test (two-tailed) was utilized in all other cases. At the 95% confidence interval, a P value less than 0.05 was considered statistically significant.
留言 (0)