











記住我


Conceptualization, G.M.B. and Z.Z.M.; methodology, A.O., G.M.B., Z.Z.M., M.I., D.H. and A.M.P.; software, Z.Z.M. and R.E.D.; validation, I.Ṣ.F. and A.O.; formal analysis, D.H., A.M.P. and R.E.D.; investigation, G.M.B. and Z.Z.M.; resources, D.H., A.M.P. and M.I.; data curation, R.E.D.; writing—original draft preparation, G.M.B. and Z.Z.M.; writing—review and editing, I.Ṣ.F. and A.O.; visualization, A.O. and I.Ṣ.F.; supervision, I.Ṣ.F. All authors have read and agreed to the published version of the manuscript.
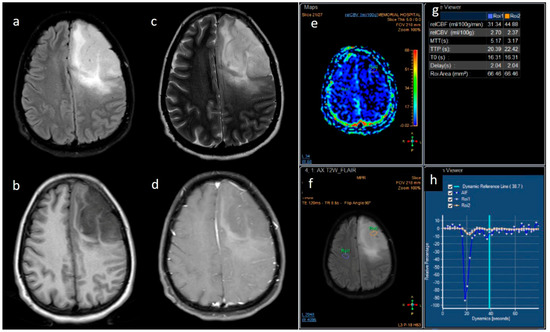
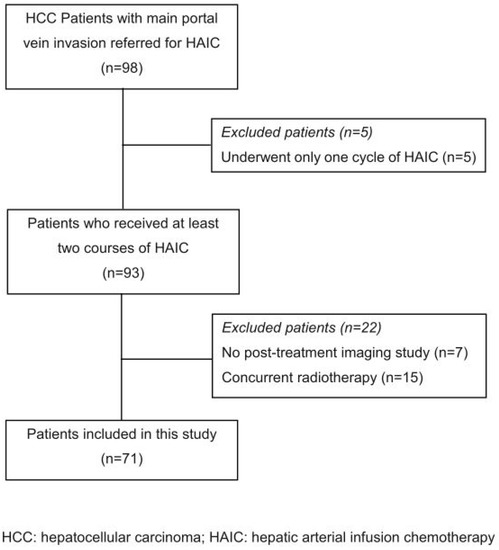
Figure 1. Right vestibular schwannoma, 1st patient, preoperatory (a), and prior to nastomosis (b).
Figure 1. Right vestibular schwannoma, 1st patient, preoperatory (a), and prior to nastomosis (b).
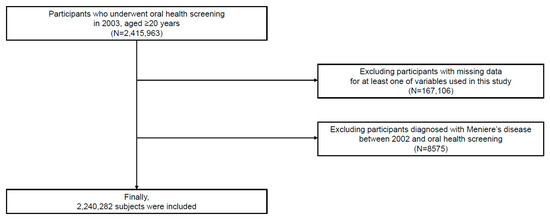
Figure 2. Left vestibular schwannoma, 3rd patient, preoperatory (a), and prior to anastomosis (b).
Figure 2. Left vestibular schwannoma, 3rd patient, preoperatory (a), and prior to anastomosis (b).
Figure 3. Motor nerveconduction: Left deepperonealnerve.
Figure 3. Motor nerveconduction: Left deepperonealnerve.
Figure 4. Sensory nerve conduction: Left superficial peroneal nerve.
Figure 4. Sensory nerve conduction: Left superficial peroneal nerve.
Figure 5. Sensorynerveconduction: Left suralnerve.
Figure 5. Sensorynerveconduction: Left suralnerve.
Figure 6. Patient positioning: (a) Left lateral decubitus. (b) Needle electrode insertion for FN monitoring (o. oris and o. oculi). (c) Electrode positioning for hypoglossal nerve monitoring (glossus). (d). Recorded potentials during mapping through electrodes positioned in the omohyoideus, sternohyoideus, and sternothyroideus muscles.
Figure 6. Patient positioning: (a) Left lateral decubitus. (b) Needle electrode insertion for FN monitoring (o. oris and o. oculi). (c) Electrode positioning for hypoglossal nerve monitoring (glossus). (d). Recorded potentials during mapping through electrodes positioned in the omohyoideus, sternohyoideus, and sternothyroideus muscles.
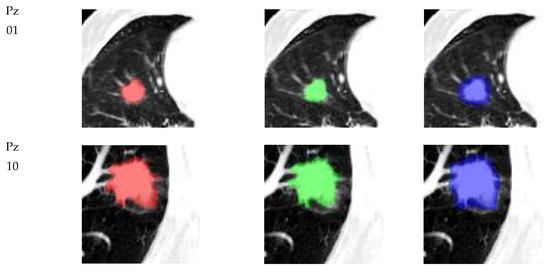
Figure 7. (a) Axial view at the level of the thyroid: Right thyroid lobe (1), isthmus (2), trachea (3), common carotid artery (4), internal jugular vein (5), sternocleidomastoid (6), sternothyroid (7), and sternohyoid (8). (b) Axial view showing the sternothyroid (1), omohyoid (2), sternocleidomastoid (3), thyroid (4), common carotid artery (5), and internal jugular vein (6). (c) Longitudinal view at the level of the thyroid shows the right thyroid lobe (1), sternothyroid (2), sternohyoid (3), and sternocleidomastoid (4).
Figure 7. (a) Axial view at the level of the thyroid: Right thyroid lobe (1), isthmus (2), trachea (3), common carotid artery (4), internal jugular vein (5), sternocleidomastoid (6), sternothyroid (7), and sternohyoid (8). (b) Axial view showing the sternothyroid (1), omohyoid (2), sternocleidomastoid (3), thyroid (4), common carotid artery (5), and internal jugular vein (6). (c) Longitudinal view at the level of the thyroid shows the right thyroid lobe (1), sternothyroid (2), sternohyoid (3), and sternocleidomastoid (4).
Figure 8. Anastomosis between the ansa cervicalis (AC) and facial nerve (FN).
Figure 8. Anastomosis between the ansa cervicalis (AC) and facial nerve (FN).
Figure 9. Measurements of facial asymmetry (a), HB grade VI right facial palsy—first patient before discharge after anastomosis, and symmetry (b), HB grade III right facial palsy—first patient after 16 months using the angle of the interpupillary and the intermodiolar line (pupillo-modiolar angle).
Figure 9. Measurements of facial asymmetry (a), HB grade VI right facial palsy—first patient before discharge after anastomosis, and symmetry (b), HB grade III right facial palsy—first patient after 16 months using the angle of the interpupillary and the intermodiolar line (pupillo-modiolar angle).
Figure 10. Progression of reinnervation in o. oris (left panels) and o. oculi (right panels). (a) Initial postoperative EMG: No activity. (b). O. oris with slight reinnervation. (c). O. oris with moderate activity. (d). O.oculi with slight reinnervation. (e). Cvasi-completely reinnervated o.oris and partially reinnervated o. oculi.
Figure 10. Progression of reinnervation in o. oris (left panels) and o. oculi (right panels). (a) Initial postoperative EMG: No activity. (b). O. oris with slight reinnervation. (c). O. oris with moderate activity. (d). O.oculi with slight reinnervation. (e). Cvasi-completely reinnervated o.oris and partially reinnervated o. oculi.
Figure 11. Compound motor action potential (CMAP) obtained after stimulation of the reinnervated facial nerve in the vicinity of the mandibular angle and recorded over the nasalis muscle (middle face). Notice the difference in amplitude; compared with the healthy side, the CMAP is quantifiable.
Figure 11. Compound motor action potential (CMAP) obtained after stimulation of the reinnervated facial nerve in the vicinity of the mandibular angle and recorded over the nasalis muscle (middle face). Notice the difference in amplitude; compared with the healthy side, the CMAP is quantifiable.
Table 1. Patient data.
PatientAge/GenderEtiologyAssociated Pathology Duration of Palsy before the AnastomosisTable 2. Total Neuropathy Score—clinical criteria.
Table 2. Total Neuropathy Score—clinical criteria.
TNSc Sensory symptoms01234NoneLimited to fingers or toesExtended to ankle or wristExtended to knee or elbowAbove knees/elbowsMotor symptomsNoneSlight difficultyModerate difficultyRequires help/assistanceDisabledAutonomic symptoms01234 or 5Pin sensationNormalReduced in fingers or toesReduced up to wrist/ankleReduced up to elbow/kneeReduced above elbow/kneeVibration sensibilityNormalReduced in fingers or toesReduced up to wrist/ankleReduced up to elbow/kneeReduced above elbow/kneeStrengthNormalMild weaknessModerate weaknessSevere weaknessParalysisTendon reflexesNormalAnkle reflex (AR) reducedAR absentAR absent and others reducedAll reflexes absent
留言 (0)