
 Figure 2.
PRISMA flow diagram of the search for randomized controlled trials and the inclusion and exclusion criteria [
Figure 2.
PRISMA flow diagram of the search for randomized controlled trials and the inclusion and exclusion criteria [





記住我


Conceptualization, H.K.; methodology, H.K.; software, E.A., G.J.C. and H.K.; validation, E.A. and H.J.K.; formal analysis, E.A. and G.J.C.; investigation, E.A. and G.J.C.; resources, E.A. and H.J.K.; data curation, E.A. and G.J.C.; writing—original draft preparation, H.J.K. and E.A.; writing—review and editing, H.K.; visualization, H.J.K.; supervision, H.K.; project administration, H.K. All authors have read and agreed to the published version of the manuscript.
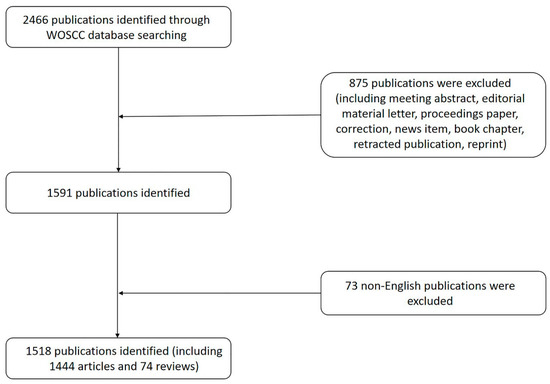
Figure 1. Schematic flow diagram of the study selection.
Figure 1. Schematic flow diagram of the study selection.
Figure 3. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on PON. (A) Early, (B) late, and (C) overall. The size of the filled squares of risk ratios reflects the effect size of individual trials. Horizontal bars represent 95% confidence intervals of difference. The diamond shape depicted the pooled estimates and uncertainty of the combined effects on early, late, and overall PON. The combined results showed no evidence of differences between palonosetron and ramosetron. For subgroup analysis, the pooled estimates of palonosetron showed that it was more effective than ramosetron in preventing early and late PON when they were administered early (*). Conversely, the pooled estimates of ramosetron indicated that it was more effective than palonosetron in preventing early PON when they were administered late (†).
Figure 3. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on PON. (A) Early, (B) late, and (C) overall. The size of the filled squares of risk ratios reflects the effect size of individual trials. Horizontal bars represent 95% confidence intervals of difference. The diamond shape depicted the pooled estimates and uncertainty of the combined effects on early, late, and overall PON. The combined results showed no evidence of differences between palonosetron and ramosetron. For subgroup analysis, the pooled estimates of palonosetron showed that it was more effective than ramosetron in preventing early and late PON when they were administered early (*). Conversely, the pooled estimates of ramosetron indicated that it was more effective than palonosetron in preventing early PON when they were administered late (†).
Figure 4. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on POV. (A) Early, (B) late, and (C) overall. The size of the filled squares of risk ratios reflects the effect size of individual trials. Horizontal bars represent 95% confidence intervals of difference. The diamond depicted the pooled estimates and uncertainty of the combined effect. The combined results showed no evidence of differences between palonosetron and ramosetron for early and overall POV. Notwithstanding, palonosetron was more effective than ramosetron in preventing late POV (*). For subgroup analysis, the pooled estimates of palonosetron indicated that it was more effective than ramosetron in preventing the overall POV when they were administered early (†), while the pooled estimates presented no evidence of differences between palonosetron and ramosetron when they were administered late.
Figure 4. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on POV. (A) Early, (B) late, and (C) overall. The size of the filled squares of risk ratios reflects the effect size of individual trials. Horizontal bars represent 95% confidence intervals of difference. The diamond depicted the pooled estimates and uncertainty of the combined effect. The combined results showed no evidence of differences between palonosetron and ramosetron for early and overall POV. Notwithstanding, palonosetron was more effective than ramosetron in preventing late POV (*). For subgroup analysis, the pooled estimates of palonosetron indicated that it was more effective than ramosetron in preventing the overall POV when they were administered early (†), while the pooled estimates presented no evidence of differences between palonosetron and ramosetron when they were administered late.
Figure 5. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on PONV. (A) Early, (B) late, and (C) overall. The size of the filled squares of risk ratios reflects the effect size of individual trials. Horizontal bars represent 95% confidence intervals of difference. The diamond depicted the pooled estimates and uncertainty of the combined effect. The combined results showed no evidence of differences between palonosetron and ramosetron for early, late, and overall PONV. For subgroup analysis, no evidence of differences was observed between palonosetron and ramosetron according to administration time.
Figure 5. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on PONV. (A) Early, (B) late, and (C) overall. The size of the filled squares of risk ratios reflects the effect size of individual trials. Horizontal bars represent 95% confidence intervals of difference. The diamond depicted the pooled estimates and uncertainty of the combined effect. The combined results showed no evidence of differences between palonosetron and ramosetron for early, late, and overall PONV. For subgroup analysis, no evidence of differences was observed between palonosetron and ramosetron according to administration time.
Figure 6. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on (A) retching, (B) complete response, and (C) use of rescue antiemetics. The diamond shape depicted the pooled estimates and uncertainty of the combined effect. The combined results showed no evidence of differences between palonosetron and ramosetron for the complete response and use of rescue antiemetics. On the other hand, palonosetron was more effective than ramosetron in preventing retching (*). For subgroup analysis, no evidence of differences was observed between palonosetron and ramosetron for the complete response according to administration time. Whereas, the pooled estimates demonstrated that palonosetron was more effective than ramosetron in the prevention of retching when they were administered early and late (†) and in the use of rescue antiemetics when they were administered early (*).
Figure 6. Forest plot of studies comparing the effectiveness of palonosetron with that of ramosetron on (A) retching, (B) complete response, and (C) use of rescue antiemetics. The diamond shape depicted the pooled estimates and uncertainty of the combined effect. The combined results showed no evidence of differences between palonosetron and ramosetron for the complete response and use of rescue antiemetics. On the other hand, palonosetron was more effective than ramosetron in preventing retching (*). For subgroup analysis, no evidence of differences was observed between palonosetron and ramosetron for the complete response according to administration time. Whereas, the pooled estimates demonstrated that palonosetron was more effective than ramosetron in the prevention of retching when they were administered early and late (†) and in the use of rescue antiemetics when they were administered early (*).
Figure 7. Funnel plots of (A) early PON, (B) early POV, (C) late PON, (D) late POV, (E) overall PON, (F) overall POV, (G) rescue antiemetics, and (H) headache. The horizontal axis demonstrates the log of risk ratio, and the vertical axis shows the inverse of the standard error.
Figure 7. Funnel plots of (A) early PON, (B) early POV, (C) late PON, (D) late POV, (E) overall PON, (F) overall POV, (G) rescue antiemetics, and (H) headache. The horizontal axis demonstrates the log of risk ratio, and the vertical axis shows the inverse of the standard error.
Table 1. Study characteristics of included studies.
Table 1. Study characteristics of included studies.
SourceAge (yrs)Sex (M/F)Weight (kg)Height (cm)ASA-PSRisk Factors for PONVType of AnesthesiaDuration of Anesthesia (min)Type of SurgeryChattopadhyay 2015 [26]18–350/10958.8 [7.2]NRI-II≥2Table 2. Further study characteristics of included studies.
Table 2. Further study characteristics of included studies.
SourceData Collection PeriodDose of Palonosetron/RamosetronAdministration TimingRescue AntiemeticsChattopadhyay 2015 [26]0–2/2–24/24–48 h0.075 mg/0.3 mgImmediate after clamping of the fetal umbilical cordMetoclopramide 10 mgKim 2013 [28]0–1/1–6/6–24/24/48 h0.075 mg/0.3 mgJust prior to induction of anesthesia1st choice, propofol 20 mg, metoclopramide 10 mg;Table 3. Risk of bias 2.0.
Table 3. Risk of bias 2.0.
SourceBias Arising from the Randomization ProcessBias Due to Deviations from the Intended InterventionsBias Due to Missing Outcome DataBias in Measurement of the OutcomeBias in Selection of the Reported ResultOverall Risk of BiasChattopadhyay 2015 [26]LowLowLowLowSome concernSome concernKim 2013 [28]LowLowLowLowSome concernSome concernKim 2015 [29]LowLowLowLowLowLowLee 2015 [30]Some concernLowLowLowSome concernHighPark 2013 [31]Some concernLowLowLowSome concernHighRoh 2014 [40]LowLowLowLowSome concernSome concernSwaika 2011 [32]Some concernLowLowSome concernSome concernHighYatoo 2016 [33]Some concernLowSome concernSome concernSome concernHighBang 2017 [34]LowLowLowLowSome concernSome concernPark 2021 [35]Some concernLowLowLowLowSome concernPatel 2018 [36]Some concernLowLowLowLowSome concernPiplai 2012 [37]Some concernLowLowLowSome concernHighSavalia 2021 [27]Some concernLowSome concernSome concernSome concernHighYoon 2016 [38]Some concernLowLowSome concernSome concernHighSong 2017 [41]LowLowLowLowLowLowAhluwalia 2015 [42]Some concernLowLowLowSome concernHighVinay 2017 [39]LowLowLowSome concernSome concernHighTable 4. The results of meta-analysis and GRADE evidence quality for each outcome.
Table 4. The results of meta-analysis and GRADE evidence quality for each outcome.
No of StudiesNo of PatientsConventional Meta-AnalysisTrial Sequential AnalysisNNTQuality AssessmentQualityRR with 95% CIHeterogeneity (I2)Publication Bias (Egger’s Test)Conventional Test BoundaryMonitoring BoundaryRISROBInconsistencyIndirectnessImprecisionPublication BiasEarly PON121263RR: 1.048; 95% CI 0.811 to 1.35446.34−1.090; 95% CI −2.489 to 0.308Not crossNot cross9.5% (1263 of 13,314 patients)NNTH: 741; 95% CI NNTH 25 to ∞ to NNTBNot seriousNot seriousNot seriousNot seriousNot serious⨁⨁⨁⨁
留言 (0)