1. IntroductionThe male gonads perform two very important functions that are essential for the male reproductive system; they produce gametes, i.e., spermatozoa, and release sex hormones [
1]. Their proper functioning depends on many different factors: age, the influence of nutrition, stimulants, hormones, pharmacological agents, and substances that disrupt the hormonal and vitamin balance [
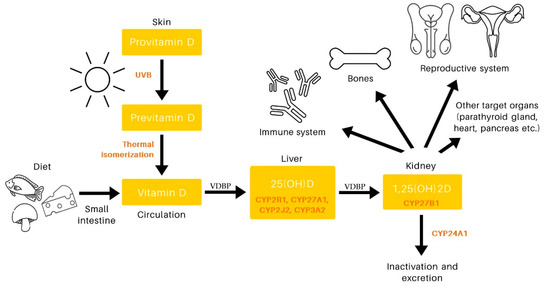
2]. Currently, the research on male reproductive health is focusing on the growing global trend of declining sperm count and increasing male reproductive system abnormalities, which has been related, among others, to lifestyle factors as well as environmental impact. Among these, numerous studies have investigated the role of vitamin D (VD) in the proper functioning of the male reproductive system.Initially, the action of VD was associated mainly with the maintenance of calcium and phosphorus homeostasis, which have a significant effect on skeleton mineralization. However, in recent years, new knowledge has emerged about its biological function and its potential to reduce the risk of many chronic diseases [
3]. The known range of its target organs has expanded, and the discovery of vitamin D receptor (VDR) expression and vitamin D metabolizing enzymes (VDME) in the testes, male reproductive tract, and human sperm suggests that VD plays a role in the male reproductive role [
4]. Although several reviews have been made on the subject, no consensus has been reached regarding the role of VD in male fertility. Moreover, new intervention studies in humans have only appeared in the last few years
The aim of this paper is to provide an up-to-date, comprehensive review of the existing literature regarding the experimental and clinical evidence for the effects of VD on the components of male fertility, sperm parameters, and sex hormone production.
3. Materials and MethodsA review of relevant literature was conducted using the MEDLINE, Cochrane, and Web of Science databases. The following keywords were used in the search: vitamin D, cholecarciferol, ergocarciferol, vitamin D levels, male fertility, male infertility, semen, sperm, sex hormones, testosterone, estradiol, follicle stimulating hormone, luteinizing hormone, sex hormone binding globulin, inhibin b. During the search, individual keywords and their combinations were typed using AND, OR, or both. The literature search covered papers published from January 2011 to June 2022. Only English-language scientific papers were taken into account. All published randomized clinical trials, retrospective, prospective, observational, and comparative human studies were included, while case reports, comments/letters to the editor, and reviews were omitted. The analysis did not include any in vitro or animal investigations. Title and abstracts were assessed, and articles were classified according to predefined inclusion and exclusion criteria. The eligibility of each article found was assessed independently by two reviewers, and excluded records were verified by another. Full text of selected articles was obtained for further review. Two reviewers independently assessed the quality of the full-text papers describing the strength and level of confidence of the results using the levels of evidence published by The Oxford Centre for Evidence-Based Medicine (CEBM) in 2009 [
44]. An Excel file was created containing the following data from selected publications: name of the first author of each study, year of publication, country, sample size, age of participants, health status, study design, variables used in adjustments, reported semen, and sex hormones rates. One reviewer extracted data, the correctness of which was checked by other reviewers, and all discrepancies were resolved through discussion. This review was registered in the INPLASY platform of registered systematic review and meta-analysis protocols (INPLASY2022110151) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA statement) guidelines [
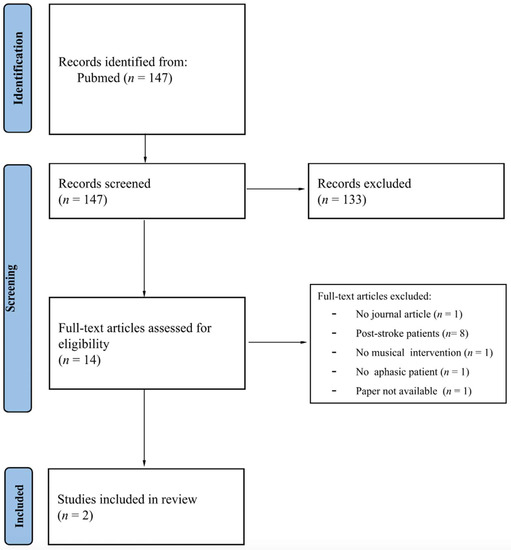
45]. 4. ResultsAn initial database search found 830 studies. After applying the eligibility criteria to the titles and abstracts, 193 articles were eligible for the full-text review. This number was reduced to 53 eligible studies by a literature search and screening process. The selection approach is shown in the PRISMA chart (
Figure 2). All detailed data collected from the studies are presented in
Table 1,
Table 2,
Table 3 and
Table 4. Studies on VD included patients from 24 different nations: Argentina, Austria, Bangladesh, Brazil, China, Denmark, Egypt, Germany, Holland, India, Iran, Ireland, Italy, Jordan, Malaysia, Norway, Pakistan, Poland, Qatar, Slovakia, South Korea, Spain, Turkey, and the USA. The age of the participants ranged from 18 to 97 years. Five studies focused on young people, six on elderly males, and the remaining studies examined middle-aged men or patients of various ages. The analyzed participants were drawn from the general population (n = 16), were patients of andrology clinics/had semen abnormalities (n = 27), or were selected on the basis of other criteria (n = 10). Out of the included 53 articles, 32 focused on the effect of VD on sperm parameters (
Table 1 and
Table 2) and 34 discussed the effect on sex hormones (
Table 3 and
Table 4). Furthermore, 36 studies were classified as observational and 17 as interventional. Various techniques were used to assess the level of VD in the serum: chemiluminescence immunoassay (n = 13), electrochemiluminescence (n = 7), enzyme-linked immunosorbent assay (n = 10), isotope dilution liquid chromatography tandem mass spectrometry (n = 8), radioimmunoassay (n = 5), high performance liquid chromatography (n = 4), competitive protein-binding assay (n = 2), enzyme-linked fluorescent assay (n = 1), liquid chromatography mass spectrometry (n = 1), chemiluminescent microparticle immunoassay (n = 1). Four studies did not report the method of measurement. 4.1. Vitamin D and Semen Parameters: Observational StudiesOf the included articles, 23 investigated the relationship between VD levels and semen quality using observational studies. All are cross-sectional studies. The studies are summarized in
Table 1.VD levels can be seen to have a beneficial effect on sperm quality, as indicated by a positive correlation between VD serum levels and total and/or progressive sperm motility [
35,
46,
47,
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60]. This correlation was significant in men from the general population [
35,
46], but also in patients of andrology clinics/men with semen abnormalities [
47,
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60]. However, seven studies failed to link VD to sperm motility or returned statistically insignificant results [
61,
62,
63,
64,
65,
66,
67]. In contrast, the existence of a correlation between VD levels and sperm count and sperm morphology is uncertain. Only eight studies showed a positive relationship between sperm concentration/total number and VD levels [
46,
52,
53,
54,
55,
57,
58,
60], and ten publications confirmed a correlation between VD levels and normal sperm morphology [
35,
47,
51,
52,
53,
54,
56,
57,
58]. Only one study found that low VD levels are not a risk factor for poor semen quality in a population of young healthy men, although high VD levels were unexpectedly associated with a lower percentage of normal sperm morphology. However, after the adjustment for potential confounders, the results were found to be insignificant [
61].In contrast, a cross-sectional study of 170 men revealed an association between U-shaped VD levels and semen parameters, showing that both low and high VD levels are associated with poor semen quality [
46]. In this study, men with 25(OH)D ≥ 50 ng/mL (≥125 nmol/mL) had lower sperm concentration, sperm progressive motility, sperm morphology, and total progressive motile sperm count compared to men with 20 ng/mL ≤ 25(OH)D
46].The first study on the relationship between serum VD levels and sperm DNA fragmentation in humans appeared in 2018. Azizi et al. [
51] postulated that there may be a link between serum 25-OHD and reactive oxygen species (ROS) in semen and sperm DNA fragmentation. The results suggest that increasing 25(OH)D levels are associated with a decrease in apoptotic cells and ROS, however, the relationship was not significant. Since then, only two studies have been conducted that showed a significant negative correlation between VD and sperm DNA fragmentation [
53,
58]. 4.2. Vitamin D and Semen Prameters: Interventional StudiesThe last few years have seen several studies on the effect of VD supplementation on sperm parameters. This review collated ten such studies, six of which were randomized clinical trials, two prospective interventional studies, one longitudinal observation study, and one case control. The summary and general effect of VD supplementation on semen parameters in clinical trials are presented in
Table 2.Many studies have shown an improvement in motility, especially progressive after supplementation with VD [
68,
69,
70,
71,
72,
73]. However, only four of the intervention studies demonstrated any efficacy in increasing sperm concentration [
69,
70,
71,
73]. Only one study found administration of VD to improve sperm morphology [
70]. The effects do not seem to be dependent on the length of VD supplementation: both short-term (2–3 months) and long-term (5–6 months) supplementation was able to improve patient outcomes [
68,
69,
70,
71,
72,
73,
74,
75]. In addition, studies of the same length differed in their results: both positive results [
71,
72,
73] and no changes [
75,
76] were obtained after three-month supplementation with VD. These differences may be due to adjustment for potential confounders; however, all of the three-month studies were unadjusted for any covariates. 4.3. Vitamin D and Sex Hormones: Observational StudiesBoth VDR and the enzymes metabolizing VD are expressed in Leydig cells [
4], suggesting that VD plays a direct role in regulating steroidogenesis. Twenty-two of the human studies of the association between 25(OH)D and sex hormones are summarized in
Table 3. The effect of VD on serum levels of male sex hormones has been analyzed in several studies, but with inconsistent results. Most observational studies indicate that serum 25(OH)D3 levels were not associated with circulating total testosterone (TT) or free testosterone (FT) levels [
46,
47,
48,
49,
50,
59,
61,
77,
78,
79,
80,
81], with exceptions in seven studies [
52,
57,
60,
82,
83,
84,
85]. In addition, some of these studies revealed a significant association between 25(OH)D and sex hormone binding globulin (SHBG) [
48,
59,
61,
77,
79]. In addition, two studies found a negative association with FT and a positive relationship with SHBG [
48,
79]. In such situations, VD deficiency may indirectly affect the hormonal state by modulating the bioavailable fraction of testosterone.The relationship between VD and testosterone may be age dependent. The majority of studies on older men (over 50) show a positive relationship between 25(OH)D levels and testosterone [
82,
83,
84,
86,
87]. However, this association disappeared after adjusting for confounding factors such as comorbidities [
86]. No association was found between 25(OH)D and testosterone in men aged under 35 [
46,
48,
61,
88]. This suggests that the relationship between VD and testosterone may be influenced by age-varying factors such as an increase of SHBG level, as well as age-related comorbidities including endocrine pathologies. Moreover, studies by Zhao et al. [
79] and Blomberg Jensen et al. [
48] revealed a negative correlation between 25(OH)D3 and estradiol (E2) level. In contrast, two other studies showed a positive relationship with E2 [
83,
87]. However, less promising results were noted for other hormones; none of the eligible studies discovered any connection between VD and FSH, and one study found a negative association between LH and VD [
52]. In addition, only one study investigated the correlation between VD and inhibin B, and it was found to be positive [
48]. 4.4. Vitamin D and Sex Hormones: Interventional StudiesThe search also encompassed the potential impact of VD supplementation on male hormones. The results are given in
Table 4. Unfortunately, intervention studies have not achieved any unequivocal findings on the effects of VD on sex hormones. The effects seemed to be variable and dependent on the length of VD supplementation. Short-term (1.5–4 months) supplementations were not capable to influence circulating levels of TT [
72,
75,
76,
89,
90,
91,
92]. Long-term (6–12 months) VD supplementation in different age groups may generate a significant increase in TT [
93] and/or FT and SHBG [
94] or no change [
70,
95]. However, even longer (36 months) interventions did not show a positive effect with a decrease in FT levels being noted [
96]. One study found VD therapy to have a positive effect on estradiol levels [
90] while another found a negative one [
93]. SHBG has been found to decrease with VD supplementation [
75,
90]. The other hormones were not affected by supplementation or were not taken into account in the studies. Ergocalciferol (VD2) supplementation was only used in one study [
93]. However, the findings do not indicate that VD3 supplementation yielded any significant benefits in this regard. 5. DiscussionLittle is known about the role VD plays in male reproduction, despite the identification of VDR, and its associated enzymes, in the reproductive system. Most knowledge in this area has been obtained from cross-sectional observational studies, with interventional studies only appearing recently. As such, the data provides only a vague answer. The main goal of this systematic review was to synthesize evidence showing a link between VD, sperm quality parameters and sex hormone production.
Table 5 summarizes the major findings from the studies included in this review.Four out of six studies comparing infertile and fertile men revealed that the serum vitamin D levels of infertile men were considerably lower than those of fertile men [
52,
55,
58,
60]. This finding is in line with previous meta-analysis on this topic and suggests that VD has beneficial effects on male reproduction [
98]. The analysis of the correlation between VD and sperm quality parameters showed it to have the most significant impact on sperm motility. In most of the included articles, serum VD levels were significantly associated with total sperm motility [
35,
47,
48,
49,
50,
51,
52,
53,
54,
56,
57,
58,
59,
60] and progressive motility [
35,
46,
48,
50,
53,
55,
56,
57,
59]. Sperm motility is one of the key elements affecting successful fertilization. Therefore, it is important to know the factors affecting it and the underlying mechanisms. Sperm motility, as an energy-consuming process, is strongly tied to mitochondrial adenosine triphosphate (ATP) synthesis. Mitochondrial function is regulated by many substances, one of which is cyclic adenosine monophosphate (cAMP). cAMP as a cellular second messenger acts by activating various downstream factors such as protein kinase A (PKA) [
99]. Jueraitetibaike et al. [
65] proposed a mechanism for increasing sperm motility by promoting ATP synthesis through the cAMP/PKA pathway, as well as an increase in intracellular ions, which is influenced by VD. In this in vitro study, sperm kinetic parameters increased after incubation with 1,25(OH)2D, and with them ATP concentrations, cAMP concentrations, PKA activity, and cytoplasmic calcium concentration also increased. This would support the experimental evidence that points to a direct non-genomic effect of VD on human sperm.There is considerable disagreement among researchers regarding the relationship between VD levels and other sperm parameters. Fewer than half of the studies found a positive and statistically significant correlation between VD levels and sperm concentration [
46,
52,
53,
54,
55,
56,
57,
58,
60] and/or morphology [
35,
47,
51,
52,
53,
54,
56,
57]. This is the first systematic review to examine the impact of VD on sperm DNA fragmentation; to date, only three articles on this subject appear to have been published, all of which are observational. Only two of them confirmed a negative correlation between the level of sperm DNA fragmentation and the level of VD [
53,
58]. In addition, in the MOXI study, where men from couples with a mild factor of male infertility were given multivitamin preparations containing, among others, vitamin D, it was not possible to find differences in sperm DNA fragmentation between men with and without vitamin D deficiency [
100]. Hence, it has been suggested that the sperm nuclear matrix plays a critical role in regulating DNA fragmentation and degradation. VDR is closely related to the nuclear matrix, and VD is believed to play a significant role in stabilizing the chromosomal structure and thus protecting DNA from harm and breakage. Therefore, it is plausible that VD and its receptor act as protectors of the sperm genome [
101,
102]. However, this requires further research.The evidence for the effects of VD on the production of male sex steroid hormones was less apparent. Sex steroids are produced by Leydig cells [
103]. On Leydig cells, VDR and VD metabolizing enzymes are also expressed. VD, when bound to VDR, acts as a transcription factor in the promoter regions of the gene encoding the steroidogenesis enzyme. The articles mentioned in the review show an inconsistent relationship between VD and the production of sex hormones. No significant correlation was found between LH, FSH, and VD levels in any of the analyzed studies. However, some studies have found a significant correlation between VD and TT, FT, and SHBG levels. Despite evidence from several studies [
93,
94,
104,
105], a recent meta-analysis did not support the hypothesis that VD stimulates testosterone levels [
106]. The exact molecular mechanism linking VD to testosterone production is still unknown. Some authors have suggested the hypothesis that genomic stimulation of osteocalcin expression by VD may play a key role in the regulation of testosterone production by the testes [
107].In men, estrogens are mainly derived from circulating androgens and metabolism is regulated by the enzyme aromatase. VD has been functionally related to estrogen signaling and VDR has been found to affect estrogen levels systemically and locally through tissue-specific regulation of aromatase [
108]. However, to date, no human studies have shown a convincing causal link between VD status and estrogen production [
109]. More research is needed to investigate how VD status affects not only estrogen production but also estrogen signaling, which may be another direct target of VDR.The role of VD in the male reproductive system is still poorly understood. However, evidence from animal research that connects VD insufficiency with infertility or gonadal malfunction strengthens the significance of VD in reproduction. In a study by Zamani et al. [
110], animals kept on a VD-deficient diet demonstrated profoundly impaired sperm concentration, morphology, and motility, and a significant reduction in serum testosterone levels and comparable gonadotropin levels compared to controls. The depletion of VD stores and the induction of moderate degrees of VD deficiency by dietary measures significantly impaired spermatogenesis and the microscopic testicular architecture in rats. These findings can be attributed, at least in part, to decreased androgen production. The first in vivo study brought attention to the strong relation between D hypovitaminosis in rats and decreased levels of circulating testosterone [
111]. However, it is difficult to establish the exact mechanism of the hormonal regulation of testosterone production. Some authors support the theory that in animals, testosterone secretion may be regulated by changes in intracellular calcium homeostasis in Leydig cells. It has been proposed that testosterone synthesis as a result of VD action may be mediated by osteocalcin, a hormone generated by osteoblasts that is involved in bone metabolism [
112]. Recent research has revealed the impact of the fat–VD relationship on sperm motility and mitochondrial membrane potential, with animals fed a high-fat diet demonstrating lower reproductive potential than animals fed a control diet; clearly, a high-fat diet and VD deficiency both influence sperm quality, which may therefore affect fertility [
113]. Additionally, significantly increased DNA fragmentation was observed in the sperm of animals fed a diet deficient in VD and those that were obese due to diet. Based on this, it can be concluded that the observed DNA damage may be the cause of the low reproductive potential in obese men deficient in VD [
104]. Testosterone biosynthesis is closely related to the lipid metabolism in the gonads around the testes. VD regulates the synthesis and metabolism of lipids in adipose tissue through VDR [
114]. Vdr knockout animals had impaired testicular and perinuclear adipose tissue histology, indicating a strong relationship between lipid metabolism and VDR-mediated testosterone production. These findings support the belief that VDR plays a crucial role in controlling testicular lipid metabolism, which in turn affects testosterone production and reproduction potential in male mice [
115]. Although the results of animal studies are very promising, they have not been reproduced in humans yet. It is possible that the relationship between VD and semen quality parameters noted in rodent studies is not relevant to humans, or that these associations may only be reflected in severe VD deficiency. The most important study examining whether VD has a direct effect on male reproductive function are randomized clinical trials with VD supplementation. Despite promising findings from animal studies and human observational studies, the results of interventional studies do not yield unequivocal conclusions. Of the 10 intervention studies reviewed, 6 showed that VD supplementation improved progressive sperm motility [
68,
69,
70,
71,
72,
73]. The remaining findings indicated that treatment with VD had no significant effect on changes in other sperm parameters. To ascertain whether VD supplementation can affect blood testosterone levels, several studies have been performed. One investigation found that treating VD-deficient individuals with VD increased testosterone levels. However, in the majority of randomized clinical trials, no substantial effect of VD supplementation on male testosterone levels was reported. These discrepancies should be regarded with caution. For example, conditions with severe VD3 deficiency are likely to respond more positively to VD3 supplementation on sperm parameters than those with mild or no deficiency. Previous studies on men found a relationship between severe VD3 deficiency and decreased fertility [
48,
74,
116]. Moreover, there is mounting evidence that traditional VD supplementation fails to achieve appropriate 25(OH)D levels. Since VD is fat-soluble, it accumulates mostly in adipose tissue [
117]. Obese men are more vulnerable to deficiency in this manner. When VD buildup in adipose tissue limits release into the systemic circulation, individuals with autoimmune disorders may require very large doses of VD treatment to boost blood 25(OH)D levels slightly [
118]. Given that obese people with autoimmune disorders frequently have 25(OH)D insufficiency and decreased testosterone levels, situations like these should be examined in future studies [
119,
120].
The results of the studies selected for this review should be treated with caution due to some limitations. Most studies used a small sample size with high levels of heterogeneity in the study design. In addition, possible confounding factors (other causes of infertility, comorbidities, lifestyle, eating habits, age, season, ethnicity) may hinder the correct interpretation of the research. The inability to make appropriate comparisons between studies is also due to the variability in the choice of cut-off values for determining vitamin D deficiency by the authors. Another limitation that certainly influences the results are the VDBP levels and VDR polymorphisms, neither of which were addressed in the studies. Therefore, no statistical analysis of these results was performed as high heterogeneity would lead to ambiguous or unreliable results. Moreover, most of the studies included in the review are cross-sectional studies, and their nature makes it impossible to delineate a causal relationship between the variables. For these reasons, the clinical relevance of all observations made should be confirmed by further research.

留言 (0)