1. IntroductionCirrhotic patients have an impaired defense system against bacteria associated with reduced bacterial clearance [
1,
2]. This immune defect facilitates bacterial translocation induced by increased intestinal permeability and intestinal bacterial overgrowth observed in cirrhosis [
3]. Bacterial infection is present at admission or develops during hospitalization in about 30% of patients with cirrhosis [
4]. The most common infection was spontaneous bacterial peritonitis (SBP) [
4].SBP is a serious complication representing an advanced stage in patients with cirrhosis and ascites [
5,
6]. There are three types of SBP: (1) classic SBP; (2) culture-negative neutrophilic ascites (CNNA); and (3) monomicrobial non-neutrocytic bacterascites (MNB). The 2013 American Association for the Study of Liver Diseases (AASLD) guideline on the management of adult patients with ascites due to cirrhosis suggested empiric antibiotic therapy for patients with ascites fluid PMN counts ≧ 250 cells/mm3 or 3 but with symptom/sign of infection [
7]. This implies that all three types of SBP need prompt treatment when a symptom/sign of infection is present. In addition, when first reported, the in-hospital mortality of an episode of SBP exceeded 90%; however, the rate has been reduced to approximately 20% through early diagnosis and prompt antibiotic therapy [
8]. Nevertheless, the prognosis of these three types of SBP is rarely compared with each other.Bacterial translocation from the gastrointestinal tract is the most common source of SBP. Thus, two-thirds of SBP cases were caused by GNB, of which Escherichia coli is the most frequently isolated pathogen [
4,
8]. Therefore, the 2013 AASLD guideline and 2018 EASL guideline recommended that the first-line antibiotic treatment for SBP is third generation cephalosporins [
7,
9]. However, changes in the patterns and microbiology of SBP have been observed in some regions over the past few years, such as the increased prevalence of CNNA, ESBL-producing bacteria, increased resistance rate to first-line antibiotics [
10], and higher frequency of Gram-positive organisms [
11]. In a Netherlands report, a nonsignificant increase in the proportion of patients with SBP caused by Gram-positive bacteria and multidrug-antibiotic-resistant bacteria over 10 years was found [
12], prompting our interest in studying the microbial pattern of SBP and whether it would influence the prognosis.
Therefore, the study aimed to investigate the incidence and prognosis of the three types of SBP, the microbial pattern, and to determine whether the form, the bacterial pattern, and the drug-resistant strain would influence the prognosis of SBP.
2. Materials and Methods 2.1. Patient Selection and Follow-Ups
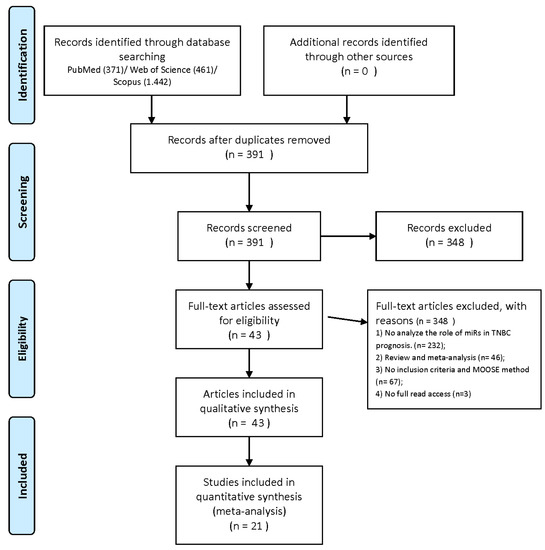
With the approval of the ethical committees of Chang Gung Memorial Hospital (202000112B0), a list of patients with a discharge diagnosis of SBP and liver cirrhosis between January 2006 and July 2017 was obtained sequentially from the medical record management committee. A total of 327 patients who met the criteria for SBP and were diagnosed for the first time were included in the retrospective study. Patients’ clinical, demographic, hematological, and biochemical data were obtained at diagnosis, and the MELD-based scores were calculated accordingly. Patients were followed up until February 2018 or until death.
2.2. Diagnosis, Definition, and Management of Liver Cirrhosis and Spontaneous Bacterial PeritonitisThe diagnosis of liver cirrhosis was based mainly on the following criteria: (1) Typical sonographic diagnosis for liver cirrhosis [
13]; (2) ascites were caused by liver cirrhosis (serum-ascites albumin gradient > 1.1 g/dL) [
14]; (3) exclusion of other underlying diseases such as malignancy (HCC or metastasis), right-sided congestive heart failure, Budd–Chiari syndrome, post-sinusoidal obstruction syndrome, portal or splenic vein thrombosis, and the possibility of schistosomiasis. Management of liver cirrhosis was in accordance with the AASLD, Baveno VI, as well as the Asian Pacific Association for the Study of the Liver (APASL) guidelines [
7,
15,
16].SBP was diagnosed upon positive ascites culture and/or an absolute neutrophil count in ascites fluid of ≧250 cells/mm3, in the absence of a surgically treatable source of infection and other causes of elevated ascites neutrophil count, such as hemorrhage, pancreatitis, peritoneal tuberculosis, or carcinomatosis [
17,
18,
19]. The treatment of SBP adhered to the recommendations of the International Ascites Club and AASLD guidelines [
17].
There are three variants of SBP: (1) classic SBP (elevated PMN count >250/mm3 and positive culture); (2) culture-negative neutrophilic ascites (CNNA): ascites culture is negative and PMN cell count is >250/mm3 (3) monomicrobial non-neutrocytic bacterascites (MNB), in which PMN count < 250/mm3 but the culture was positive.
2.3. The Outcomes of SBP
Due to the high short-term mortality, the outcome or prognosis of SBP was defined as the in-hospital, 3-month (3 M), and 6-month (6 M) mortality.
2.4. The Diagnosis of Hepatorenal Syndrome and Hepatic EncephalopathyThe hepatorenal syndrome was diagnosed based on clinical criteria brought up by the AASLD, the International Club of Ascites (ICA), and Kidney Disease: Improving Global Outcomes (KDIGO) [
20,
21]. The prerequisites were the absence of any other apparent cause for the acute kidney injury, including shock, current or recent treatment with nephrotoxic drugs, and the absence of ultrasonographic evidence of obstruction or parenchymal kidney disease.Hepatic encephalopathy (HE) was diagnosed according to the European Association for the Study of the Liver (EASL)/American Association for the Study of Liver Diseases (AASLD) guidelines [
22,
23] and by the exclusion of other causes of mental status changes. HE was graded by the West Haven Criteria [
24]. 2.5. The Diagnosis of Bacteremia (Sepsis)Bacteremia was diagnosed when at least two serial sets of blood cultures yielded positive bacteria species. Sepsis was defined as two or more SIRS criteria with documented infection focus [
25] (SBP in this study). 2.6. Calculations of Predicting ScoresThe MELD score was 11.2 × ln (international normalized ratio (INR)) + 9.57 × ln (creatinine, mg/dL) + 3.78 × ln (bilirubin, mg/dL) + 6.43) with lower bound of one for all three variables and an upper bound of four for serum creatinine. The MELD-Na score was MELD score − Na − (0.025 × MELD score × (140 − Na)) + 140, in which Na was bounded at 125 and 140. The iMELD score was MELD score + (Age × 0.3) − (0.7 × Na + 100) [
26]. 2.7. Methods/Assays Used For Serum Biochemistry and Hemogram
The method/assays used for serum biochemistry were as follows: serum creatinine: colorimetry (reference value: F:0.44–1.03, M: 0.64–1.28 mg/dL); serum bilirubin: spectrophotometry (reference value:0.3–1.2 for <60 y/o, 0.2–1.1 for 60–90 y/o, 0.2–0.9 for >90 y/o mg/dL); serum AST/ALT: enzymatic method (reference value: AST: ≦34 U/L, ALT ≦ 36 U/L); serum Na: ion-selective sensor (reference value: 136–146 mEq/L); serum albumin: colorimetry (reference value: 3.5–4.5 g/dL), respectively.
The method/assays used for serum hemogram were as follows: serum INR: electrochemical method (reference value: 2.0–3.0); WBC and PLT: automated cell count (reference value: WBC: 3.9–10.6 103/μL; PLT: 150–400 103/μL); Hb: spectrophotometric method (reference value: M:13.5–17.5; F:12–16 g/dL), respectively.
2.8. Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median and interquartile range (IQR, 25–75 percentile), depending on their distribution. Non-parametric Kruskal Wallis test or Mann–Whitney U test was used to compare continuous variables among three groups, or between two groups respectively. Post-hoc tests including Bonferroni correction were used to adjust for the significance level for multiple pairwise comparisons and multiple testing correction. Categorical variables were reported as frequencies or counts with percentages. Their significance was calculated by Chi-square test first while Fisher’s exact test was performed instead when more than 20% of the cells have expected frequencies less than 5. Survival analyses were performed by univariable and/or multivariable logistic regression analysis.
Statistics were performed using SPSS software (SPSS Inc., Chicago, IL, USA, Version 22). A p-value of <0.05 was considered statistically significant.
4. Discussion
In this study, we attempted to find better prognostic risk factors for cirrhotic patients with SBP, taking into account all clinical variables, including SBP types, bacteriology, and other cirrhotic complications such as HRS and HE. It was found that the prevalence of classic SBP was nearly equivalent to CNNA, followed by MNB. As for the microbial pattern, GNB was still more prevalent than GPC (75% vs. 25%), and E. coli were the most common bacteria species followed by K.P. and then Staphylococcus. The total percentage of ESBL strain in culture-positive patients was 10.9%. By univariable and multivariable logistic regression survival analysis, there was no significant difference in predicting short-term mortality among the three SBP types, neither between GNB vs. GPC, nor between ESBL- and non-ESBL- producing bacteria. Only bacteremia (sepsis), hepatorenal syndrome (HRS), and serum creatinine (Cr) were independent predictors of in-hospital and 3-month mortality, whereas HRS and Cr were independent predictors of 6-month mortality. The results could greatly help identify high-risk groups of patients with SBP, allowing more prompt and intensive management.
SBP has high short-term mortality. When first reported, the in-hospital mortality of an episode of SBP exceeded 90%; however, the rate has been reduced to approximately 20% through early diagnosis and prompt antibiotic therapy [
27,
28]. To improve the stratification of patient care, identifying the most robust predictors of mortality in cirrhotic patients with SBP is critical but often overlooked [
29]. The MELD score has been shown to be more accurate in predicting 3-month survival than the Child−Turcotte−Pugh (CTP) classification for patients with cirrhosis awaiting liver transplantation in the United States [
30]. However, the literature review showed limited information on whether they were applicable in subgroups of patients with liver cirrhotic-related complications such as SBP [
31,
32].We have previously demonstrated that for patients with HBV-related liver cirrhosis and SBP, the iMELD score had the highest AUC among the MEDL-based models and significantly outperformed CTP and ALBI scores in predicting 3-month and 6-month mortalities [
33]. However, baseline clinical parameters such as SBP types, bacteriology, HRS, and HE were not considered. In this study, univariable and multivariable logistic regression survival analyses were used to consider all these variables and MELD-based scores, including the iMELD score. The results showed that only HRS and serum Cr consistently predicted the in-hospital, 3-month, and 6-month mortalities. This corresponds to a meta-analysis that also demonstrated that renal dysfunction was the most important independent predictor of mortality in cirrhotic patients with SBP [
29]. In fact, renal failure occurs in 30% to 40% of people with SBP and is the leading cause of death [
34]. The risk of renal impairment as well as mortality may be decreased significantly (renal impairment 30.6% to 8.3%, mortality 35.4% to 16.0%) [
35] with an infusion of intravenous 25% albumin solution [
36]. Therefore, the up-to-date AASLD guideline has recommended albumin infusion in patients with SBP and renal dysfunction [
20]. Our result strengthens this notion that early identification of renal dysfunction at baseline in patients with SBP is critical and potentially life-saving.The study also demonstrated that bacteremia (sepsis) is an important prognostic factor in predicting in-hospital and 3-month mortalities. Our previous study also found that SBP was associated with high sepsis-related mortality [
37]. This implies that aggressive treatment for sepsis in patients with SBP is of utmost importance [
38]. Indeed, an important predictive scoring system designed to assess the severity of illness in patients with sepsis, the Chronic Liver Failure-Sequential Organ Failure Assessment (CLIF-SOFA) score, has been shown to be useful in determining the appropriate antibiotic regimen [
39]. Patients with suspected SBP who are not critically ill (CLIF-SOFA score
39].Furthermore, in this study, the prevalence of classic SBP was almost comparable to that of CNNA, which corresponds to other studies [
10,
40]. The mortality rates among these classic, CNNA, MNB SBP types were not significantly different if appropriate antibiotics are given promptly. In addition, GNB vs. GPC, nor ESBL-producing vs. non-ESBL-producing bacterial species did not affect outcomes. This finding is reasonable since empirical 3rd generation cephalosporins could cover 79.7% of patients without ESBL-producing bacteria strain. The finding that third generation cephalosporin (CRO)-resistant bacteria in ascites culture independently predicted patients’ in-hospital mortality reminds us of the need for timely antibiotic adjustment based on the susceptibility results.Thus, liver transplantation should be seriously considered for survivors of SBP who are otherwise good transplantation candidates [
35].

留言 (0)