
記住我

In patient care, critical incidents (CIs) are unexpected events that may reach patients and thus threaten patient safety. By allowing reporting and analysis of such events, critical incident reporting systems (CIRS)1 are expected to induce organizational learning from these events and near misses to improve the safety of healthcare organizations before a sentinel event happens.2 Thus, they play a role of leading indicators to highlight the importance of CIRS and near misses for organizational learning. Critical incident reporting systems offer potential value as risk management instruments.3 Therefore, most health care institutions in industrialized countries are legally obliged to have them in place and to maintain strategies to optimize patient safety.4,5 Nonetheless, CIRS are increasingly falling into disrepute for not being effective in sustainable improving patient safety.6,7
These systems depend on hospital staff to recognize and report incidents using standard report forms. These are then reviewed by a team of expert clinicians chosen for their abilities to analyze and manage risk.6,7 Depending on each reported CI’s severity (e.g., the expert team’s risk assessment rating8), a causal analysis may be conducted and corrective or preventive feedback may be provided. That is, this information will be disseminated as appropriate within the institution.9,10 This way, CIRS are intended to contribute to continuous improvement loops.
However, CIRS are subject to major limitations. These include underreporting,7 which reflects both their voluntary nature and the characteristics of each institution’s safety culture. If CI reports are misused to allocate blame, for example, staff members may hesitate to submit them. In addition, unless CIs lead to patient harm, the reported information is commonly difficult to validate.11 Similarly, gaps in the information regarding an incident’s context, which is rarely fully transmissible using a reporting form, interfere with a causal analysis of that incident.
Furthermore, when Liukka et al12 studied a web-based incident reporting database (HaiPro, used in over 200 social service and health care organizations in Finland) from 16,019 incident reports over a 5-year period, they found that extremely few of the examined CI reports (2.7%) triggered written recommendations to prevent recurrences of the reported incident. This finding illustrates how disruption of the flow of information can limit its effectiveness. In line with prior research,13 Jäger et al’s longitudinal analysis of 5493 CIs demonstrated that the “feedback loop”—the cycle of information, action and improvement made possible by CIRS data—was clearly underused.14
Within a functional feedback loop, reported instances of patient safety hazards become data for causal analyses; the results of those analyses allow elimination or reduction of the identified causes. By increasing patient safety, this process is expected to improve future care. However, the latest World Health Organization report on CIRS notes that as many incident reports remain unaddressed, their current use often leads to few real improvements; that is, CIRS data are largely wasted.2
As CIRS are used in hospitals worldwide, numerous studies discuss aspects of learning from reported incidents. Unfortunately, comparable information on the characteristics of the reported CIs, as well as comparative reviews on corrective actions following reported CIs, is currently lacking. To address this shortfall, we set 2 main objectives for the current review: first, to systematically analyze hospital-based CIRS studies regarding each reported incident’s type, severity, and contributing factors and, if possible, second, to evaluate the actions taken to prevent further such incidents.
METHODSThis systematic review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.15
Search StrategyWe searched the MEDLINE, Embase, CINAHL, and Scopus databases. Our queries used 4 normal-text strings—“Critical Incident Reporting System,” “Incident Reporting System,” “Critical Incident Reporting” and “Patient Safety Learning System”—and the following MeSH terms and Boolean operators (including parentheses): (“Hospitals”[Mesh] OR “Patients” [Mesh] OR “Inpatients”[Mesh] OR hospital*[tiab] OR Patient*[tiab] OR inpatient*[tiab]) AND (“Medical Errors/methods”[Mesh] OR “Medical Errors/statistics and numerical data”[Mesh] OR “Risk Management/methods”[Mesh] OR “Risk Management/statistics and numerical data”[Mesh]) AND (Critical Incident*[tiab] OR Incident Reporting*[tiab] OR Near Miss*[tiab] OR Safety Incident*[tiab]).
Inclusion and Exclusion CriteriaWe included observational studies using data from established hospital-based CIRS that reported CIs’ characteristics and/or improvement actions. To be eligible for inclusion, studies had to be published between 2000 and 2019 in English or German, use compatible definitions of CI reporting (i.e., incidents that affected or could have affected 1 or more patients’ safety),1 and include data from a minimum of 100 reports. We excluded studies from national and statewide reporting systems,16–18 those in nonhospital settings19,20 (e.g., primary care, nursing homes), and those for reporting specific incident types21,22 (e.g., falls, equipment, transfusions).
Data Extraction, Quality Assessment, and AnalysisAll titles and abstracts of the identified articles were independently screened for eligibility by 2 reviewers and arbitrated by a third to reach consensus in cases of disagreement. For data extraction, we used 2 forms: (1) study characteristics, that is, author(s), publication year, country of origin, setting/sample, study design, the used definition of CIs, and study duration in months and (2) incident-related details, that is, characteristics/types, consequences, contributing factors, and organizational actions taken/lessons learned. We classified the incidents’ consequences according to the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) index,23 the contributing factors according to the Yorkshire Contributory Factors Framework and the Human Factors Classification Framework,24,25 and any actions taken according to an action hierarchy model on strengths of interventions to improve patient safety as proposed in the literature.26,27
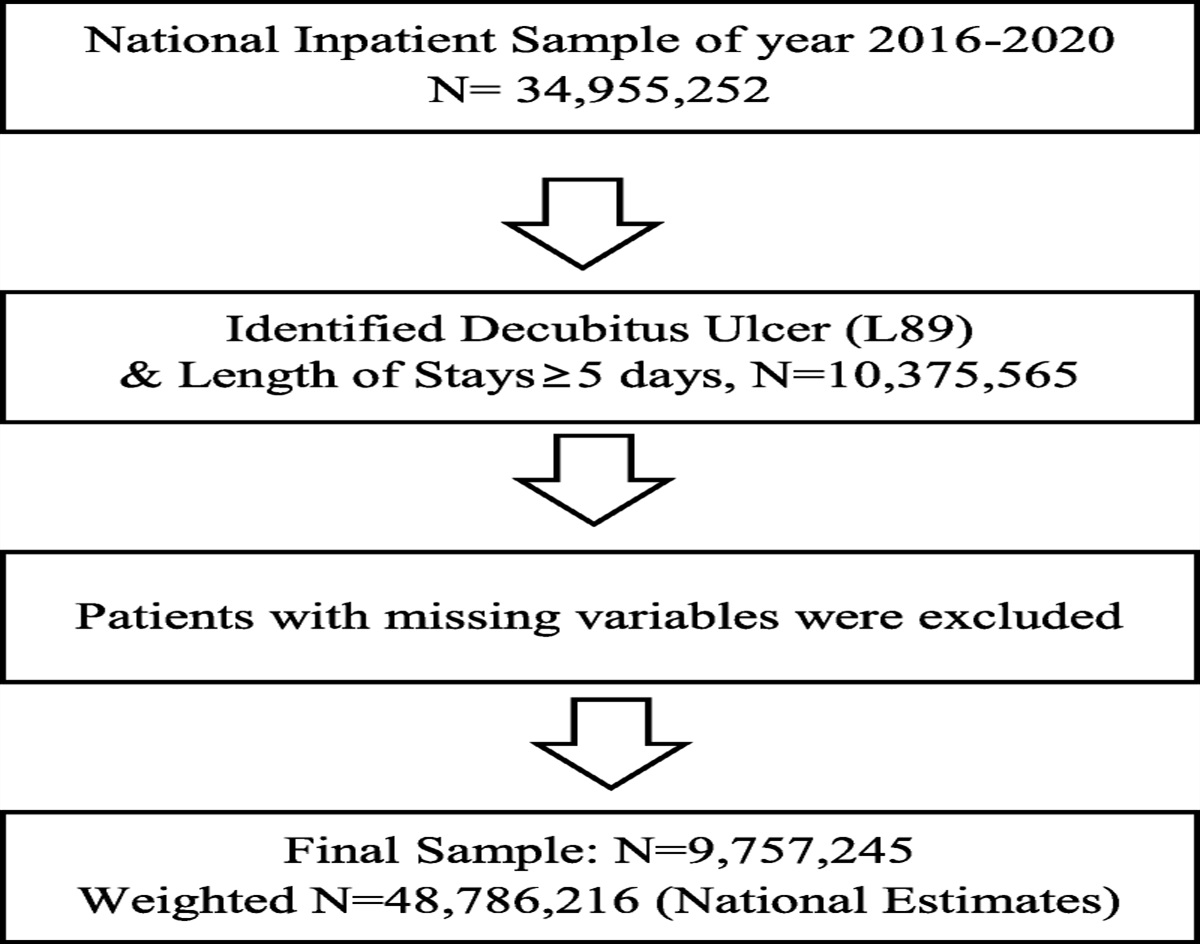
For quality assessment, as no specific critical appraisal tools are available for studies on “critical incident reporting systems.” Two authors (K.G., R.S.) assessed each study’s reporting methodology, that is, they decided whether its included information was adequately structured—first on the basic characteristics of each reported CI (type, consequences/severity, contributing factors) and then on the actions taken to prevent that CI’s recurrence. Disagreements between the 2 study reviewers were discussed until consensus was reached. Based on this process, they narrowed our literature search’s 3621 initial returns to 41 that were eligible for detailed review (Fig. 1).
 FIGURE 1:
FIGURE 1: Flow diagram of article retrieval.
RESULTS Study CharacteristicsThe 41 included studies were conducted between 2004 and 2019 and referred to 479,483 analyzed reports from 212 hospitals. The majority were conducted in Europe (n = 21, 51.2%), followed by North and South America (n = 13, 31.7%), Asian (n = 6, 14.6%), and Middle Eastern (n = 1, 2.4%) regions. Thirty were single-center studies; 11 were multicenter. For the single-center group, incident report sample sizes ranged from 11428 to 8809.29 For the multicenter group, the numbers of included hospitals ranged from 2 to 29, with CI numbers ranging from 58430 to 266,224.31 Across all studies, durations ranged from 12 to 132 months. Settings included “university/academic/teaching hospitals” (n = 29), “acute care hospitals” (n = 23), “suburban hospitals” (n = 13), “urban hospitals” (n = 11), “tertiary hospitals” (n = 7), “quaternary hospitals” (n = 3), “rural hospitals” (n = 2), and “community hospitals” (n = 1); for the remaining 147, no hospital type was specified. Critical incident–reporting clinical departments included surgical disciplines, anesthesia, standard, pediatric and neonatal intensive care units, pediatrics, internal medicine, emergency, ophthalmology, and radiology (see supplementary file, https://links.lww.com/JPS/A508, summarized study characteristics).
Reporter CharacteristicsIn 22 of the 41 studies (53.6%), the incident reporters’ professions were specified. Of these 22 studies’ reporters, 83.7% were nurses (range, 0.8%32–84.7%33), 6.5% pharmacists (range, 1%34–51.9%35), 4.8% physicians (range, 1.1%31–50.3%36), and 5% other professions, including laboratory technicians, paraclinical staff, dieticians, etc (range, 0.1%33–10%37).33,34,37–43 In 2 studies,32,36 most reports were made by physicians. In 1 study,44 apart from “physician,” no professions were specified.
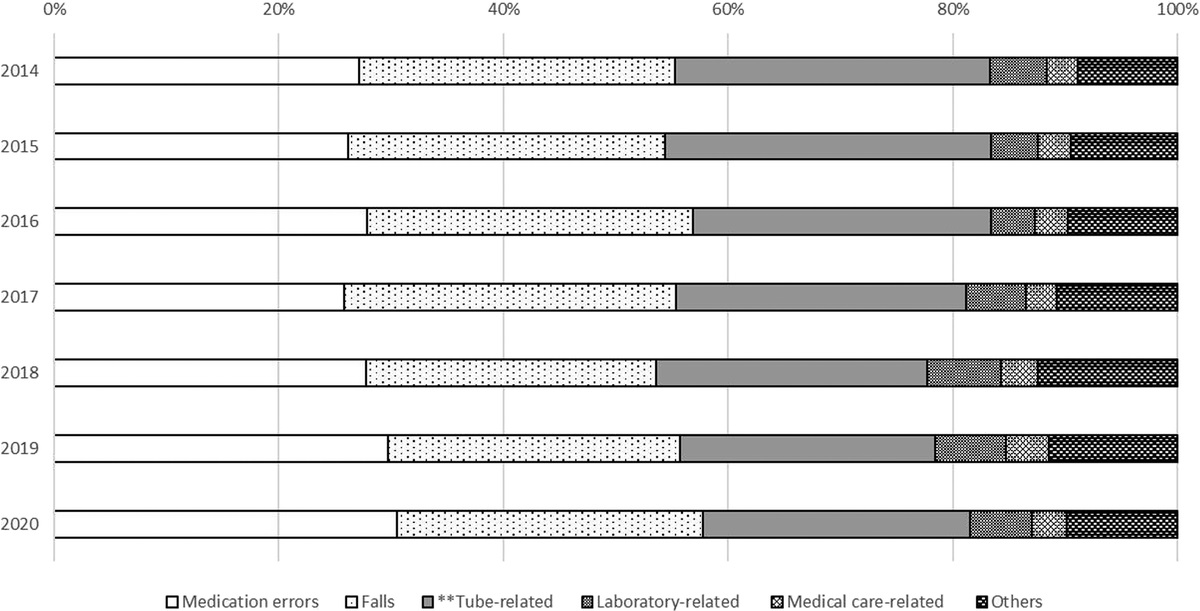
Incident TypesIn 35 of the 41 included studies (85.4%, n = 467,616 CIs), the types of CI were specified (Fig. 2). The 3 most commonly reported CI categories were: medication related (28.8%; range, 3.4%45–63.3%46), administration related (12.9%; range, 2.3%45–18.9%47), and fall related (11.5%; range, 0.2%40–16.6%29). In 1 study,31 adverse clinical events were classified as events related to medical treatment. Across the 24 studies (58.5%) that provided CI incidences, these ranged from 1.648 to 10340 reported CIs per 1000 patient days (overall mean, 28 CI reports per 1000 patient days).
 FIGURE 2:
FIGURE 2: Types of reported critical incidents.
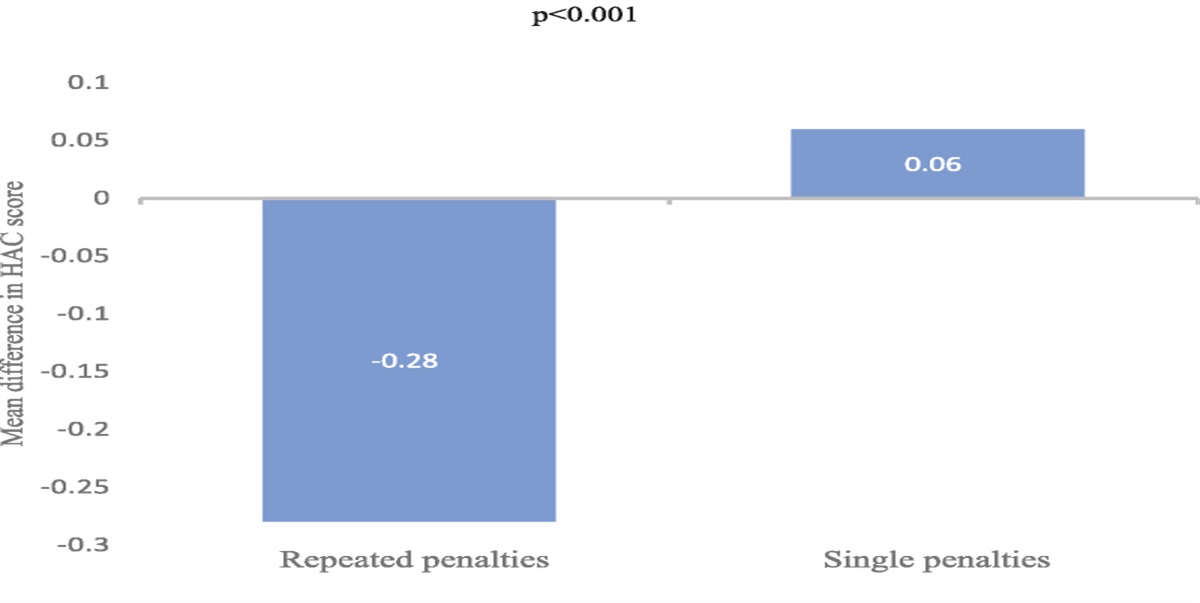
Consequences of IncidentsIn 23 of the 41 studies (56.1%, n = 341,097 CIs), CIs’ consequences were reported. As recommended by the NCC MERP index, we divided these consequences into 5 groups, no error (circumstances or events that have the capacity to cause error), error, no harm (an error has occurred but has not caused any harm to the patient), error, harm (an error has occurred and harmed the patient), error, death (an error has occurred that could have contributed to or could have led to the death of the patient), and not coded (not classified; Fig. 3).23 As detailed in Figure 3, 21.7% (74,086/341,097) of incidents resulted in temporary or permanent patient harm, and 0.4% (1208/341,097) resulted in patient death.
 FIGURE 3:
FIGURE 3: Consequences of critical incidents according the NCC MERP index.
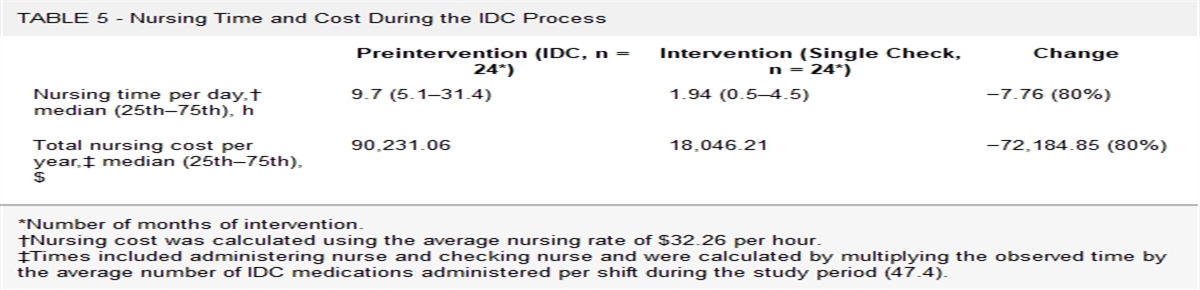
Contributing FactorsIn 20 of our 41 chosen studies (48.8%), the authors indicated factors (n = 51,650) that contributed to the reported CIs (shown in Fig. 4). Overall, the most frequent contributing factor was “active failure” (13,464/51,650, 26.1%), that is, failure regarding healthcare providers’ performance or behavior (e.g., carelessness, treatment errors, failure to meet standards). Additional main contributing factors were “communication” (6548/51,650, 12.7%), “patient factors” (4203/51,650, 8.1%) pointing to patient features (e.g., severity of diseases) that make care more difficult, and “individual factors” (4006/51,650, 7.8%), pointing to healthcare workers’ features that may contribute to active failure, such as inexperience. A secondary contributor was team-related factors (2734/51,650, 5.7%), which consisted of “team factors” (1214/51,650, 2.4%), “staff workload” (879/51,650, 1.7%), and “management of staff and staffing levels” (641/51,650, 1.2%).
 FIGURE 4:
FIGURE 4: Contributing factors according the Yorkshire Contributory Factors Framework.
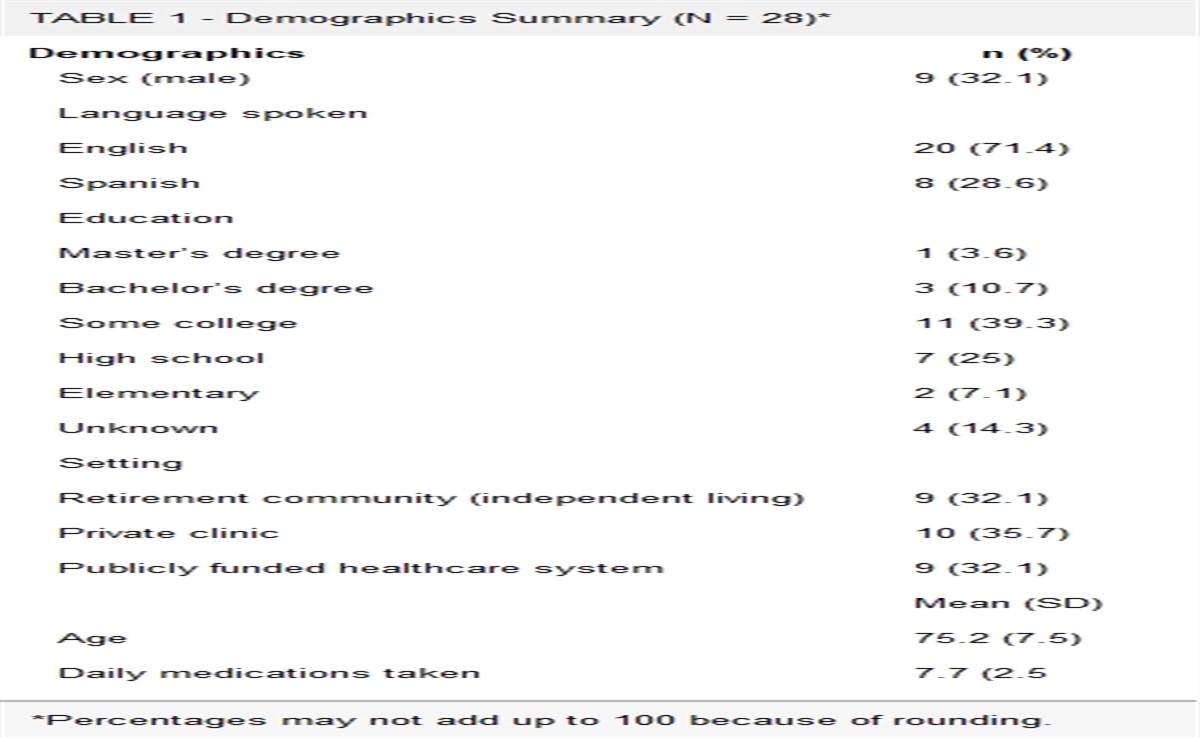
Actions TakenIn 15 of our 41 studies (36.6%), organizational actions taken to prevent future incidents were reported. Of those 15, 13 provided 118 detailed examples of measures taken to improve patient safety (see supplementary file, https://links.lww.com/JPS/A508, summarized study characteristics). Following the Institute for Healthcare Improvement’s action hierarchy (2015),26,27,49 we divided those into three classes. Based on each action’s potential impacts on systems change and improvement, we labeled it as “strong” (n = 32, 27.1%), “intermediate” (n = 49, 41.5%), or “weak” (n = 37, 31.4%; Table 1). Examples include improving the functionality of syringe pumps33 (a “strong action”), the introduction of medication cards for emergency situations and frequently used medications54 (an “intermediate action”), and a nurse-to-nurse check for intravenous pump settings (a “weak action”).44
TABLE 1 - Example Actions Sorted Along the Hierarchy of Impact for Change (N = 118) Magnitude of Actions* No. Reported Actions Examples Stronger actions (these tasks require less reliance on humans’ ability to remember to perform the task correctly) 32 –Expansion of spaces and personnel in emergencies.50In reviewing studies about using CIRS in a variety of acute care hospital types, focusing on corrective measures and learning from incidents to improve patient safety, this study provides an overview of the types of CIs reported, their contributing factors, the extent of patient harm that resulted, and the actions taken.
The first important result is that there is a lack of standards in reporting the results of studies on CIRS: rarely were analytical frameworks mentioned, the characteristics of a “critical incident” were defined inconsistently, and the CI categorizations varied broadly. For example, regarding the reported events’ consequences, the studies analyzed in our systematic review used highly heterogeneous terminology: only one51 explicitly applied the NCC MERP index.23 As this lack of standardization and classification of CIs across healthcare systems impedes interstudy comparisons, it slows progress.
The second important result from the review is the lack of evidence of effective organizational learning and improvement of patient safety so far, which is supported by prior claims to change or improve CIRS processes.25,49 Remarkably, only approximately one third of the analyzed studies provided information on improvement actions that followed the analyses. Their main study focus was on the processes of information feeding into the CIRSs (reports, reporters, and consequences) rather than the actions taken. The vital tasks of translating the findings into strong actions that would increase patient safety were much less discussed. Therefore, as a standard feature, any future report on CIRS research should include details of how the CI reports were used to improve patient care using a framework for describing the corrective actions.
The 41 hospital-based CIRS studies covered by this systematic review identified 479,483 CI reports from 212 hospitals. Investigating which kinds of events were reported and by which professional group allows to shed light on the capability of CIRS as an instrument for identifying patient safety hazards. For example, nurses were responsible to varying degrees for more than 80% of the reported incidents, which also reflects that nursing staff provide a vast majority of frontline hospital care.58 However, hazards within the physicians’ work processes may be underrepresented in the reports.
In line with prior research,59 the most frequently reported CIs were categorized as “medication related” (28.8%). This ranking reflects the high potential for harm from errors in drug administration.60–62 The second most reported class of CI (20.6%) was “unspecified clinical event”. As a catch-it all term, it is similar to “administrative error,” a classification also used in CIRS-related studies to indicate arrays of unspecified CIs. The vagueness of classification points to relevant, unsolved issues in learning from incidents: the causes of an event are subject to analyses and are influenced by the knowledge, perspective, and interests that the analysts bring with them.63 The same event may be attributed different causes by different analyzing teams and at different points in time. For example, the classification of a report before it is analyzed may result in it being assigned to completely different categories than would be the case after analysis. A forgotten insulin administration, for example, may be considered an active failure due to inattention, while—after analysis—one may realize that it is also the result of a complex interplay between organizational factors, such as the usability of the medication chart, and the staffing around the time of administration. The topic “communication” also exemplifies the challenges of classifying CIs and their causes into meaningful categories: communication problems were attributed as causes for 12.7% of all CIs, apparently confirming communication’s “error proneness.”64 In addition, several of our reviewed studies included communication both in “incident type” and “contributing factors” or even in other factor classes (e.g., “human factors,”53,65 “individual (staff) factors”48).
While CIRS can be used to identify hazards, previous research has concluded that the distribution of incident types cannot be used to assess the severity of reported problems or to compare them with one another66: different incident types’ reporting rates may reflect different motivational factors; errors in medication administration may be more readily reported than complex diagnostic errors that become evident only over time. In addition, the culture may be inducive to reporting or not, so that higher reporting rates do not reflect greater problems, but a better reporting culture.67
Classifying contributing factors according to the Yorkshire contributory factors framework25 allowed us to compare them across studies. The most frequently mentioned contributing factor was “active failure,” which encompasses a broad spectrum of factors in healthcare workers’ performance or behavior (e.g., carelessness, any failure regarding treatment processes or standards of medical care).33,43,68,69 This is an important finding, because it illustrates a common limitation of learning from incidents: If the reports are mainly attributed to factors that are “visible” in the situation, rather than trying to find more latent systemic causes, the potential for organizational learning is basically restricted to local improvements. From research about root cause analysis, this tendency to blame the actors involved at the sharp end of an event is well known.70 We therefore recommend based on this review finding that managers responsible for the analysis of incidents should closely track this tendency to assign the responsibility to frontline actors at the sharp end but also keep an eye on “the larger picture” with a more systematic approach. To this end, major changes in the use of CIRS may be necessary. Analyzing critical events, identifying systemic causes, and deriving strong actions demand considerable time and resources. Considering the current limited resources invested in healthcare CIRS, it would not allow to do this for every reported event.2 Thus, groups of incidents reporting similar events can be pulled together and used to do a major analysis, for example. In addition, series of events were proposed to be used to shed light on a patient’s journey.71 In this way, the strength of CIRS lies in providing new qualitative insights into unknown safety issues facing the healthcare organization rather than an unreliable count on an already known issues.72
Furthermore, the details of CI circumstances are essential for their causal analysis; however, these cannot be fully considered in an anonymous written report.73,74 Therefore, recent proposals have suggested to investigate broader time horizons, as well as the patients’ participation in the incident analyses. This would allow exam of the incident within the context of a patient’s journey.71
While none of the reviewed studies applied the Yorkshire framework,25 2 studies48,51 referred to Reason’s59,75 and Vincent’s73 models of accident causation. None of the other studies applied a theoretical framework. As noted in a previous study, this omission suggests a lack of overall consistency.13
Regarding the gravity harm involved, incidents not harming patients but clearly involving an error seem to be the most likely to be reported. This may be explained by the principle that as such errors result in actual occurrences, they are easier to detect than near misses. In addition, if no patients are harmed, many questions of personal responsibility are not raised in the analysis or are associated with less guilt, which might increase the motivation to report. However, poor staffing as system contributor to the occurrence of adverse events relates to excessive nurse workload and lower nurse-to-patient ratios as they are correlated with hospital mortality and morbidity as well as high levels of burnout, work absenteeism, and high job turnover among nurses.76
The error types were reported only in few instances, however, without specifying them for example as error of omission. We did therefore not systematically assess them. However, the fact that the category “error of omission” is not mentioned may also indicate a bias in hazard identification using CIRS, as reporting forgotten or missed actions is less probable than reporting actual behavior.
For CIRS to be effective in improving patient safety, the corrective actions derived need to be defined, implemented, and followed up upon. In addition, deriving strong improvement actions not only also demands considerable resources but often requires actions outside the action repertoires of the participating individuals.77 This means that if systemic causes such as staffing levels or issues in the design of work areas or instruments were identified as important contributors, strategic decisions on the hospital, or sometimes even on the regulatory, national level would need to be taken to generate and sustain strong systemic corrective actions. A good example is the design of healthcare information technology that is often involved in adverse events and that is hard to change from a local level but needs cooperation with industry and sometimes even regulatory demands to be improved.78 Because of these limitations in power to invest resources and bring about systemic change within analysis teams, the causal analyses often derive corrective actions that are the direct cure of an identified issue.79
Attributing incidents to active failures makes the process of identifying a corrective action that can also be implemented fairly simple. Readily available cures include warning signs, updated protocols, or training courses. Although all of these are quite easy to implement, because they target provider behavior, they are also known to offer rather low effectiveness in terms of reducing patient safety hazards.49,80 As Kellogg et al80 sobering illustrated, weak actions derived from event analyses failed to prevent events from recurring during their 8-year study period.
To sum up, the scattered and unsystematically reported evidence in learning from CIRS to improve patient safety paints a rather dire picture of the current situation. Thus, new ways of using CIRS need to be developed. As outlined previously, using reports as qualitative information for uncovering potentially unknown hazards could be a fruitful approach. New tools supporting causal analyses therefore are needed, and best practices in prioritizing action within CIRS management should to be urged14 including schemes to decide which reports to analyze, which to observe, and how to analyze groups of similar incidents. Concerning insights from other instruments to detect patient safety hazards, such as morbidity/mortality conferences and patient complaints, need to be incorporated into the creation of a detailed and comprehensive picture of emerging hazards. Furthermore, we consider it useful to differentiate the target level of potential improvements to not only generate “quick fixes” on the local level, but also develop corrective actions that target systemic levels. Our study proposed framework for classifying incidents, contributory factors, and consequences, systematizing research and practice is an important baseline for improving the current CIRS to not generate waste,14 but actual learning on departmental, hospital, and healthcare system level.
As a final note, we want to highlight that none of the studies systematically reported on the sustainability of the corrective actions or how and when a follow-up happened. This lack of long-term perspective is particularly outstanding, as CIRS aim at systemwide improvements for safety.
LimitationsWhile all of our reviewed studies focused on hospital CIRS, their broad heterogeneity, particularly regarding their methodologies and terminology, impeded the comparability of their data regarding, for example, types of incidents, contributing factors, or actions taken after a CI. Furthermore, as no specific tool was available to assess the quality of our selected CIRS-based studies, we based their eligibility entirely on our study aims. Using a pragmatic approach, our assessment depended heavily on each candidate study’s methodology and primary end points. Nevertheless, to support the comparability of our review findings, we addressed issues of study heterogeneity by applying the NCC MERP index and the Yorkshire contributory factors framework. Finally, for reporting and learning systems such as CIRS, no uniform nationwide legislations does exist across countries and their hospitals, although recommended by the World Health Organization.
CONCLUSIONSThis systematic review of studies of hospital-based CIRS data provides an overview of the characteristics of reported incidents, their contributing factors, their consequences, and their actions taken to prevent future incidents. Two main conclusions are drawn from the review: first, research on CIRS-related studies needs to systematize and align the reporting using frameworks to improve understandability and comparability of their results. Second, the reviews illustrate that there is only scarce evidence showing that systemic change in a hospital is initiated using a CIRS: there was a focus on situational, sharp-end factors in the analyses of the incidents; remarkably, only a third of the reviewed studies described the corrective actions taken; and the sustainability of the derived corrective actions was not addressed systematically. To make a CIRS a useful tool for improving patient safety, there is a need to focus on its strength in providing new qualitative insights into unknown hazards and also on developing tools to facilitate the nomenclature and management of CIRS events, including corrective actions, in a more standardized manner.
ACKNOWLEDGMENTThe authors thank Dr Hannah Ewald, a database researcher, Library of the University of Basel, for her support in developing search strategies and Andrea Wiencierz, PhD, a senior statistician, Department of Clinical Research, University Hospital Basel, for statistics support.
REFERENCES 1. Buckley TA, Short TG, Rowbottom YM, et al. Critical incident reporting in the intensive care unit. Anaesthesia. 1997;52:403–409. 2. World Health Organization. Patient safety incident reporting and learning systems: technical report and guidance. Geneva, Switzerland: World Health Organization; 2020;2020. 3. Institute of Medicine Committee on Quality of Health Care in America, Kohn LT, Corrigan JM, Donaldson MS, eds. To Err Is Human: Building a Safer Health System. In: Washington, DC: National Academies Press (US); 2000. 4. Bundesaerztekammer. Gesetz zur Verbesserung der Rechte von Patientinnen und Patienten 2013. Available froat: https://www.bundesaerztekammer.de/fileadmin/user_upload/downloads/Patientenrechtegesetz_BGBl.pdf. Accessed March 7, 2021. 6. Stiftung Patientensicherheit Schweiz. Critical Incident Reporting & Reacting NETwork. Available at: https://www.patientensicherheit.ch/cirrnet/#c978. Accessed September 12, 2020. 7. World Health Organization. Patient safety—global action on patient safety. Report by the Director-General. Geneva: World Health Organization. 2019. Available at: https://apps.who.int/gb/ebwha/pdf_files/WHA72/A72_26-en.pdf. Accessed September 2, 2020. 8. Scottish Government. The Risk Management of HAI: A Methodology for NHS Scotland; 2008. Available at: https://www.gov.scot/publications/risk-management-hai-methodology-nhsscotland/documents/. Accessed September 14, 2020. 9. Barach P, Small SD. Reporting and preventing medical mishaps: lessons from non-medical near miss reporting systems. BMJ. 2000;320:759–763. 10. Mahajan RP. Critical incident reporting and learning. Br J Anaesth. 2010;105:69–75. 11. Staender S. Incident reporting in anaesthesiology. Best Pract Res Clin Anaesthesiol. 2011;25:207–214. 12. Liukka M, Hupli M, Turunen H. Problems with incident reporting: reports lead rarely to recommendations. J Clin Nurs. 2019;28:1607–1613. 13. Benn J, Koutantji M, Wallace L, et al. Feedback from incident reporting: information and action to improve patient safety. Qual Saf Health Care. 2009;18:11–21. 14. Jäger C, Mohr G, Gökcimen K, et al. Critical incident reporting over time: a retrospective, descriptive analysis of 5493 cases. Swiss Med Wkly. 2021;151:w30098. 15. Moher D, Shamseer L, Clarke M, et al. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1. 16. Runciman WB, Williamson JAH, Deakin A, et al. An integrated framework for safety, quality and risk management: an information and incident management system based on a universal patient safety classification. Qual Saf Health Care. 2006;15(suppl 1):i82–i90. 17. Webb RK, Currie M, Morgan CA, et al. The Australian Incident Monitoring Study: an analysis of 2000 incident reports. Anaesth Intensive Care. 1993;21:520–528. 18. Cassidy CJ, Smith A, Arnot-Smith J. Critical incident reports concerning anaesthetic equipment: analysis of the UK National Reporting and Learning System (NRLS) data from 2006-2008*. Anaesthesia. 2011;66:879–888. 19. Hoffmann B, Beyer M, Rohe J, et al. “Every error counts”: a web-based incident reporting and learning system for general practice. Qual Saf Health Care. 2008;17:307–312. 20. Meyer-Massetti C, Krummenacher E, Hedinger-Grogg B, et al. Medication safety in the home care setting: development and piloting of a critical incident reporting system [in German]. Pflege. 2016;29:247–255. 21. Kobayashi K, Imagama S, Inagaki Y, et al. Incidence and characteristics of accidental falls in hospitalizations. Nagoya J Med Sci. 2017;79:291–298. 22. Lozach P, Vicariot M, Le Niger C, et al. Evaluation of the immediate transfusion reaction incident reporting system at the Brest University Hospital Center [in French]. Transfus Clin Biol. 2001;8:343–349. 23. Hartwig SC, Denger SD, Schneider PJ. Severity-indexed, incident report-based medication error-reporting program. Am J Hosp Pharm. 1991;48:2611–2616. 24. Mitchell RJ, Williamson A, Molesworth B. Application of a human factors classification framework for patient safety to identify precursor and contributing factors to adverse clinical incidents in hospital. Appl Ergon. 2016;52:185–195. 25. Lawton R, McEachan RRC, Giles SJ, et al. Development of an evidence-based framework of factors contributing to patient safety incidents in hospital settings: a systematic review. BMJ Qual Saf. 2012;21:369–380. 26. Bagian JP, King BJ, Mills PD, et al. Improving RCA performance: the Cornerstone Award and the power of positive reinforcement. BMJ Qual Saf. 2011;20:974–982. 27. National Patient Safety Foundation. RCA2: Improving Root Cause Analyses and Actions to Prevent Harm. Boston, MA: National Patient Safety Foundation; 2015. 28. Kupersztych-Hagege E, Duracher-Gout C, Ortego R, et al. Critical incidents in a French department of paediatric anaesthesia. Anaesth Crit Care Pain Med. 2017;36:103–107. 29. Tricarico P, Castriotta L, Battistella C, et al. Professional attitudes toward incident reporting: can we measure and compare improvements in patient safety culture?Int J Qual Health Care. 2017;29:243–249. 30. Rakha EA, Clark D, Chohan BS, et al. Efficacy of an incident-reporting system in cellular pathology: a practical experience. J Clin Pathol. 2012;65:643–648. 31. Rowin EJ, Lucier D, Pauker SG, et al. Does error and adverse event reporting by physicians and nurses differ?Jt Comm J Qual Patient Saf. 2008;34:537–545. 32. Wright JL, Parekh A, Rhieu B-H, et al. Real-time management of incident learning reports in a radiation oncology department. Pract Radiat Oncol. 2018;8:e337–e345. 33. Nakajima K, Kurata Y, Takeda H. A web-based incident reporting system and multidisciplinary collaborative projects for patient safety in a Japanese hospital. Qual Saf Health Care. 2005;14:123–129. 34. Donato Göttems LB, Gomes Dos Santos MdL, Carvalho PA, et al. A study of cases reported as incidents in a public hospital from 2011 to 2014. Rev Esc Enferm USP. 2016;50:861–867. 35. Ashcroft DM, Cooke J. Retrospective analysis of medication incidents reported using an on-line reporting system. Pharm World Sci. 2006;28:359–365. 36. Luebke J, Lang SJ, Reinhard T. Critical incident reporting system in risk management at the Eye Center in Freiburg [in German]. Klin Monbl Augenheilkd. 2017;234:894–899. 37. Milch CE, Salem DN, Pauker SG, et al. Voluntary electronic reporting of medical errors and adverse events. An analysis of 92,547 reports from 26 acute care hospitals. J Gen Intern Med. 2006;21:165–170. 38. Aaronson EL, Brown D, Benzer T, et al. Incident reporting in emergency medicine: a thematic analysis of events. J Patient Saf. 2019;15:e60–e63. 39. Askarian M, Ghoreishi M, Akbari Haghighinejad H, et al. Evaluation of a web-based error reporting surveillance system in a large Iranian hospital. Arch Iran Med. 2017;20:511–517. 40. Grant MJC, Larsen GY. Effect of an anonymous reporting system on near-miss and harmful medical error reporting in a pediatric intensive care unit. J Nurs Care Qual. 2007;22:213–221. 41. Härkänen M, Turunen H, Saano S, et al. Detecting medication errors: analysis based on a hospital’s incident reports. Int J Nurs Pract. 2015;21:141–146. 42. Nyflot MJ, Zeng J, Kusano AS, et al. Metrics of success: measuring impact of a departmental near-miss incident learning system. Pract Radiat Oncol. 2015;5:e409–e416. 43. Sendlhofer G, Schweppe P, Sprincnik U, et al. Deployment of critical incident reporting system (CIRS) in public Styrian hospitals: a five year perspective. BMC Health Serv Res. 2019;19:412. 44. Levtzion-Korach O, Alcalai H, Orav EJ, et al. Evaluation of the contributions of an electronic web-based reporting system: enabling action. J Patient Saf. 2009;5:9–15. 45. Choy YC. Critical incident monitoring in anaesthesia. Med J Malaysia. 2006;61:577–585. 46. Scharein P, Trendelenburg M. Critical incidents in a tertiary care clinic for internal medicine. BMC Res Notes. 2013;6:276. 47. Welters ID, Gibson J, Mogk M, et al. Major sources of critical incidents in intensive care. Crit Care. 2011;15:R232. 48. Zingg U, Zala-Mezoe E, Kuenzle B, et al. Evaluation of critical incidents in general surgery. Br J Surg. 2008;95:1420–1425. 49. Trbovich P, Shojania KG. Root-cause analysis: swatting at mosquitoes versus draining the swamp. BMJ Qual Saf. 2017;26:350–353. 50. Ramírez E, Martín A, Villán Y, et al. Effectiveness and limitations of an incident-reporting system analyzed by local clinical safety leaders in a tertiary hospital: Prospective evaluation through real-time observations of patient safety incidents. Medicine (Baltimore). 2018;97:e12509. 51. Huckels-Baumgart S, Manser T. Identifying medication error chains from critical incident reports: a new analytic approach. J Clin Pharmacol. 2014;54:1188–1197. 52. Hübler M, Möllemann A, Eberlein-Gonska M, et al. Anonymous critical incident reporting system in anaesthesiology. Results after 18 months [in German]. Anaesthesist. 2006;55:133–141. 53. Tuttle D, Holloway R, Baird T, et al. Electronic reporting to imp
留言 (0)