
記住我

The COVID-19 pandemic has created a unique crisis for many aspects of society, perhaps most notably the delivery of healthcare. The high morbidity, mortality, and viral transmission rates yielded disastrous consequence globally. The downstream effects of continuously overloaded hospitals combined with shortages of staff and equipment, disruptions to supply chains, and significantly altered provider workflows contributed to a strain on healthcare workers (HCWs) unprecedented in modern history.
Optimizing patient outcomes requires interprofessional teams to work together using practical and evidence-based team behaviors, especially during times of crisis. The quality and prevalence of these team behaviors have been reliably measured using validated surveys.1–7 A positive teamwork climate also has strong associations to improved patient outcomes.8–10
To date, the toll of the COVID-19 pandemic on teamwork has not been evaluated using large samples, and the extent to which changes in teamwork are associated with other changes in safety culture and workforce well-being is not yet understood. The primary objective of this study is to understand how teamwork climate in healthcare settings evolved during the COVID-19 pandemic. Secondary objectives are to evaluate how changes in teamwork climate were associated with changes in healthcare safety culture and provider well-being.
METHODSTeamwork climate and healthcare safety culture were assessed through 2 routine administrations of the validated and widely used SCORE survey.2,11–13 Culture domains assessed by the SCORE survey include teamwork climate, safety climate, leadership engagement, improvement readiness, and several measures of HCW well-being: emotional exhaustion, emotional exhaustion climate, and work-life balance. The administered version of the SCORE survey also included 2 novel, previously validated metrics of HCW well-being: emotional recovery and emotional thriving.12,14,15
The survey was routinely administered across 93 hospitals in 3 health systems across 10 states within the United States at 2 distinct time points around the COVID-19 pandemic. Initial survey data were collected before pandemic onset during September of 2019 and served as a baseline culture assessment. The second survey administration occurred during the heart of the COVID-19 pandemic (September 2020). All responses were self-reported. Respondents indicated work setting and facility but were not identified at an individual level. Given the anonymity of responses, it was not possible to link individual respondents or respondents at a work setting level across the 2 survey administrations. Results of the 2 survey administrations were retrospectively compared.
This study was approved by the Duke University Health System Institutional Review Board (IRB Pro00083427). All HCWs at the 3 health systems with 50% or greater full-time equivalent commitment to a specific work-setting for at least 4 consecutive weeks were invited to complete SCORE. Survey responses were anonymous and collected minimal demographic data including facility and HCW role (e.g., physician, nurse, pharmacist, technologist, etc). Facilities without survey data for both before and during the pandemic were excluded from secondary analyses.
Most SCORE domains (teamwork climate, safety climate, local leadership, improvement readiness, emotional exhaustion, emotional exhaustion climate, thriving, and recovery) were measured using a series of questions answered with a 5-point Likert scale from strongly disagree (1) to strongly agree (5). Responses included an option of “not applicable,” which were treated as missing data. Work-life balance16–18 was measured as self-reported frequency of specific work-life behaviors (i.e., rarely or none of the time [1] to all of the time [4]). For the purposes of this article, most domains are reported as percentage of staff reporting a positive, or favorable, response based on previously determined and published thresholds for that domain. Emotional exhaustion and emotional exhaustion climate are also presented as percentage of staff reporting a positive score, but for these domains, a positive response is an unfavorable response, also consistent with prior literature.12,13,15,17–19
The teamwork domain included the following items:
Disagreements in this work setting are appropriately resolved (i.e., not who is right but what is best for the patient). In this work setting, it is difficult to speak up if I perceive a problem with patient care. It is easy for personnel here to ask questions when there is something that they do not understand. The people here from different disciplines/backgrounds work together as a well-coordinated team. Dealing with difficult colleagues is consistently a challenging part of my job. Communication breakdowns are common in this work setting. Communication breakdowns are common when this work setting interacts with other work settings.Agreeing or strongly agreeing with items 1, 3, and 4 was considered a favorable response. Items 2, 5, 6, and 7 were reverse scored, such that disagreeing or strongly disagreeing with those items was considered a favorable response.
Descriptive statistics were used to depict survey respondent demographics. Cronbach αs were used to assess psychometric reliability of the scales before and during. αs range from 0 to 1, with a reliability coefficient of at least 0.70 that is acceptable for early-stage research, 0.80 for implementing cutoff scores, and 0.90 if clinically important decisions are being made.20,21 Comparisons between before and during COVID domain values were compared using the t test, with a statistical significance cutoff of a P value less than 0.05. Subgroup analysis was performed to identify changes in teamwork climate by HCW role and facility. Facilities were then grouped into 1 of 3 categories for further analysis: facilities with improved teamwork climate, no change in teamwork climate, or decline in teamwork climate. Facility domain characteristics were evaluated relative to their change in teamwork climate.
RESULTSElectronic surveys were returned by 50,412 (of 66,818) HCWs before and 50,512 (of 67,535) HCWs during the pandemic, for overall response rates of 75.45% and 74.79%, respectively. Respondents by role demonstrate similar proportions of HCW roles from before to during COVID-19 (Table 1), with registered nurses as the most frequent respondent group for each period (37.5%/36.4%). All measured SCORE domains demonstrated strong psychometric properties in both administrations. The Cronbach αs for each domain (before/during pandemic) were as follows: teamwork climate (0.83/0.83), local leadership (0.95/0.95), improvement readiness (0.95/0.95), emotional exhaustion (0.94/0.94), emotional exhaustion climate (0.92/0.92), safety climate (0.88/0.89), thriving (0.89/0.89), recovery (0.89/0.89), and work-life balance (0.85/0.85).
TABLE 1 - Respondent Roles and Percentage Reporting Favorable Teamwork Climate by Role, Before and During Pandemic Before COVID-19 Pandemic During COVID-19 Pandemic Role n % Total Respondents % Who Report Favorable Teamwork n % Total Respondents % Who Report Favorable Teamwork P for % Favorable, Before Versus During Admin support (clerk/secretary/receptionist) 2354 4.7 44.5 2257 4.5 41.3 0.01 Administrator/manager 3226 6.4 58.2 2938 5.8 59.3 0.38 Clinical support (medical assistant/EMT/etc) 1182 2.3 38.1 1047 2.1 37.1 0.45 Nurse 18,927 37.5 45.6 18,409 36.4 43.7 <0.0001 Nurse aide/CNA/PCA/PCT 2437 4.8 41.9 2499 4.9 38.4 0.0003 Other 10,912 21.6 41.8 12,668 25.1 40 0.004 Pharmacist 808 1.6 45.3 888 1.8 44.1 0.61 Physician: attending/staff 1422 2.8 51.6 1457 2.9 57 0.0002 Social worker/counselor 558 1.1 46.5 593 1.2 41.1 0.16 Technician (e.g., surg/lab/EKG/rad) 2086 4.1 40.2 1995 3.9 36.4 0.003 Technologist (e.g., surg/lab/rad) 3786 7.5 48.3 3239 6.4 45.4 0.01 Therapist (RT/PT/OT/speech) 2714 5.4 51.5 2522 5.0 50.8 0.23 Overall 50,412 100 45.6 50,512 100 43.7 <0.0001Data in bold show statistical comparison of the percentage of these respondents reporting favorable teamwork before COVID-19 pandemic versus during COVID-19 pandemic.
CNA, certified nursing assistant; EKG, electrocardiogram; EMT, emergency medical technician; OT, occupational therapist; PCA, personal care attendant; PCT, personal care technician; PT, physical therapist; RT, respiratory therapist.
In general, there was a significant decline in the percentage of respondents reporting favorable teamwork climate during the pandemic compared with the prepandemic survey (Table 1). Half of the role groups (6/12) reported a significant decrease in teamwork climate, representing nursing, nursing aides, administrative support persons, technicians, technologists, and other. Physicians were the only role reporting a significant improvement in teamwork climate in the early stages of the pandemic.
Eighteen of the 93 facilities (19%) were excluded from further analysis because they only reported teamwork climate results during the pandemic. Twenty six of the remaining 75 facilities (35%) demonstrated a significant decrease in teamwork climate during the pandemic, while 46 facilities (61%) saw no significant change in teamwork climate. Only 3 facilities (4%) demonstrated an increase in teamwork climate during the pandemic (Supplemental Table 1 https://links.lww.com/JPS/A498).
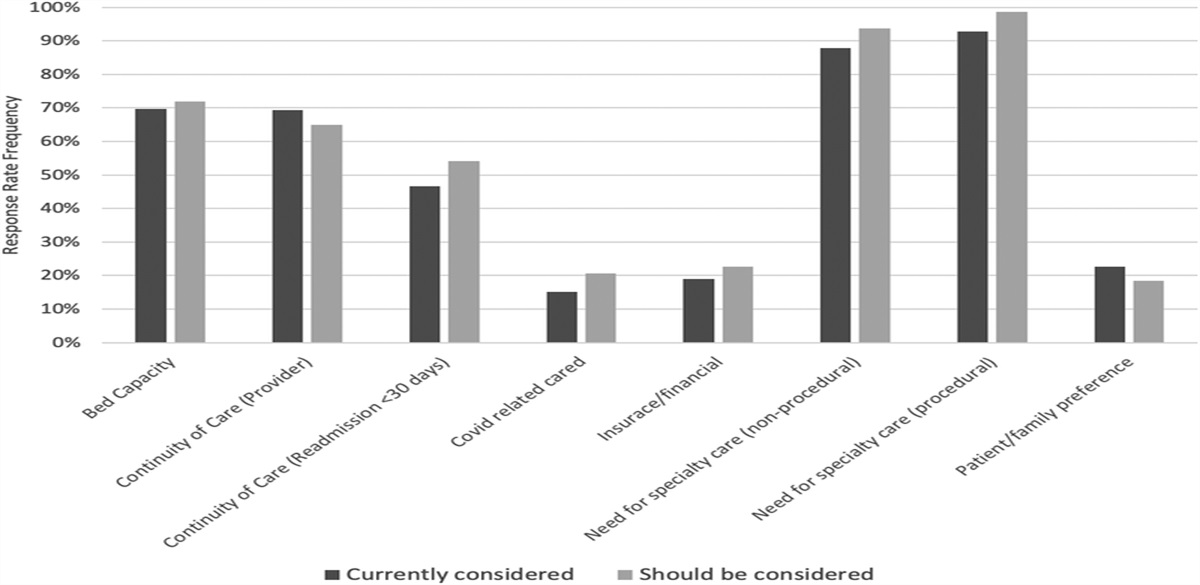
Cumulatively, the 26 facilities with a significant decline in teamwork climate during the pandemic also demonstrated concordant decreases in safety climate, local leadership, improvement readiness, and markers of HCW well-being, as measured by emotional exhaustion and emotional exhaustion climate, emotional thriving, emotional recovery, and work-life balance (Table 2). The 49 facilities with no change in teamwork climate also demonstrated decreases in well-being, but to a much lesser degree than the former group of facilities with a decrease in teamwork climate (Fig. 1). These facilities saw no statistically significant change in any of the safety culture domains of safety climate, local leadership, and improvement readiness.
TABLE 2 - Changes in the Respondents Answering a Positive Result for Each Domain During the COVID-19 Pandemic, by Their Facility’s Teamwork Climate Response Facilities With Improved Teamwork Climate Facilities With No Change in Teamwork Climate Facilities With Decline in Teamwork Climate Facilities 3 46 26 Respondents 7445 42,091 45,992 Domain Before COVID-19 During COVID-19 P Before COVID-19 During COVID-19 P Before COVID-19 During COVID-19 P Local leadership 44.6 51.4 <0.0001 63.5 64.3 0.0.6 69.7 62.5 <0.0001 Improvement readiness 49.5 55.3 <0.0001 64.3 63.7 0.21 69.0 62.1 <0.0001 Emotional exhaustion 49.0 48.3 0.56 39.5 43.6 <0.0001 38.2 47.0 <0.0001 Emotional exhaustion climate 66.0 64.1 0.09 56.4 60.0 <0.0001 54.3 63.1 <0.0001 Safety climate 37.4 44.1 <0.0001 54.3 54.4 0.71 60.0 53.2 <0.0001 Thriving 58.6 61.7 0.09 68.2 64.6 <0.0001 68.5 61.8 <0.0001 Recovery 72.4 72.6 0.88 76.5 74.3 <0.0001 75.6 71.6 <0.0001 Work-life balance 60.1 64.4 0.0002 66.2 69.2 <0.0001 70.9 68.7 <0.0001 FIGURE 1:
FIGURE 1: Change in percentage of respondents reporting a positive result by domain from prepandemic values, by facility teamwork climate response. T and P values represent comparisons between differential in facilities with decline in teamwork versus those with an increase in teamwork.
Among the 3 facilities with an improvement in teamwork climate, there was no statistically significant change in most domains of well-being, including emotional exhaustion, emotional exhaustion climate, thriving, or recovery. These facilities demonstrated statistically significant increases in safety climate, local leadership, and improvement readiness, and work-life balance (Table 2).
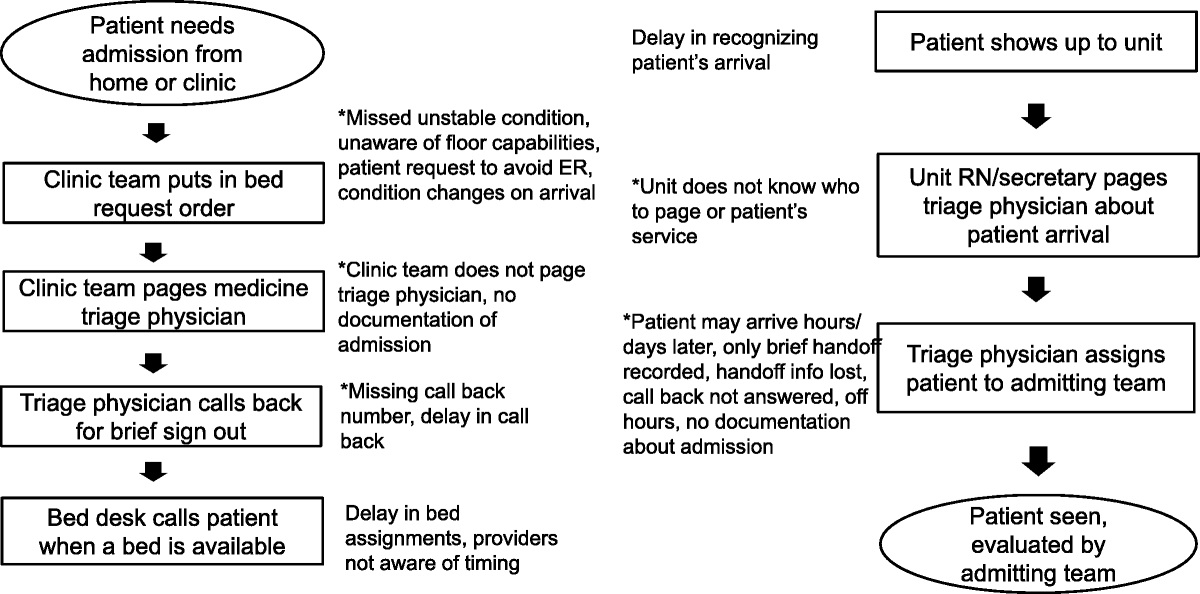
Each of the individual teamwork items demonstrated the same pattern as the global teamwork climate domain in that each item significantly decreased in the 26 facilities with a decrease in teamwork climate during the pandemic, no items demonstrated significant change in the 49 facilities with unchanged teamwork climate during the pandemic, and each item significantly increased in those 3 facilities with improved teamwork climate during the pandemic (Fig. 2). T values for individual items listed previously in facilities with a decline and improvement in teamwork (respectively) were 12.9 and 6.3 (disagreements resolved appropriately), 8.13 and 1.7 (difficult to speak up), 10.8 and 5.5 (easy to ask questions), 10.5 and 5.8 (different disciplines/backgrounds work well together), 6.7 and 3.8 (difficult colleagues a challenge), 9.7 and 4.5 (communication delays common within team), and 9.2 and 4.7 (communication delays common with other teams). All P values were less than 0.001 with the exception except of “difficult to speak up” in facilities with improved teamwork (P = 0.046).
 FIGURE 2:
FIGURE 2: Change in percentage of respondents reporting a positive result by teamwork domain item from prepandemic values, by facility teamwork climate response. T and P values represent comparisons between differential in facilities with decline in teamwork versus those with an increase in teamwork.
DISCUSSIONIn this observational study of 3 large U.S. health systems, the first year of the COVID-19 pandemic had varying effects on teamwork climate among HCWs. Of all HCWs roles, only physicians reported a significant increase in perception of teamwork climate during the first year of the pandemic, while most other roles experienced a decline in their perception of teamwork. Most notably, in healthcare facilities where teamwork climate worsened, there was concordant worsening of every other measured domain of work culture, including safety climate and HCW well-being (Table 2). In a stepwise fashion, safety culture and workforce well-being scores improved within facilities where teamwork climate either stayed constant or improved (Fig. 2).
Perhaps it is noteworthy that only a minority of facilities experienced a decline in norms of teamwork during an unprecedented global health crisis. These results support previous literature demonstrating that maintaining effective teamwork behaviors during crisis situations may be protective of the negative effects of such stressors.22–24 This effect was witnessed in measures of HCW well-being as well as other culture measures linked to patient outcomes, such as safety climate. It follows that proactive focus on team behaviors and skills will not only help team performance over time but also may support team’s well-being and ability to recover from stress. This concept has been repeatedly shown in short-term crisis situations, such as patient resuscitation events and surgeries,8,25–27 but has not been previously demonstrated amid a prolonged, systemic crisis situation like the COVID-19 pandemic.
Also of note, reported teamwork climate worsened during the pandemic for most frontline HCW roles in this sample, with the sole exception of physicians, who reported improved teamwork climate in September of 2020. Other data demonstrate that physicians have also experienced significant stress during the early phases of the COVID pandemic.28–31 The contrasting teamwork climate finding in this study is consistent with a perception gap phenomenon that has been previously described in medical teams with poor work culture.32,33 Those results show that in teams with poor teamwork, leadership engagement, or psychological safety, it is not uncommon for leaders to have an unrealistic and overly positive perception of team culture, widely disparate from the experience of their staff.32,33 In this way, physicians in the current study may represent those team leaders who, as teamwork climate suffered and teams became fractured in other ways, lost touch with the ongoing experience of HCWs in other roles.
Understanding the potential benefits of teamwork during times of crisis is particularly important as team behaviors are correlated with improved patient safety, and actionable strategies are available to improve teamwork climate. The 3 teamwork climate items demonstrating the largest statistical differentiation in both the facilities with a decline in teamwork and those with an increase in teamwork were items 1 (disagreements resolved appropriately), 3 (easy to ask questions), and 4 (different disciplines/backgrounds work well together). These specific items focus on conflict resolution, speaking up, and interdisciplinary cooperation. Interestingly, these items reflect a significant amount of psychological safety norms within the team, suggesting that when HCWs lose their voice, it is a significant harbinger of safety culture and workforce well-being decline. Each of the 3 items provides an area for focus and improvement by leaders to increase teamwork climate. Team training, crew resource management, and simulation are well-documented strategies to not only improve teamwork climate in healthcare teams but also improve team performance and patient outcomes.26,34–39 This knowledge empowers leaders with the ability to develop a strategy to support their teams in anticipation of the next crisis. This is represented through our data by the domain of improvement readiness, which also decreased in the facilities that saw a decline in teamwork. The same empowerment strategies may be applied during a crisis but will be less effective, given HCWs’ limited ability to absorb new concepts and change behaviors during times of increased strain, particularly if more than 40% of staff report burnout.40 As such, proactive team training may provide substantial benefit toward helping teams through stressful times.
Future directions for this work would include deeper investigation into characteristics that allowed some of these facilities to constructively adapt to the stresses of the pandemic, as well as those that may have contributed to declines in teamwork climate during the pandemic. Understanding these team norms and behaviors (e.g., the psychological safety components of teamwork) may identify other opportunities that leaders can use to best support their teams, their cultures, and their workforce well-being.
A primary limitation of this study is that as a large observational study, we can report associations but cannot speak to causality. However, the COVID-19 pandemic provided us a unique opportunity to looks at culture before and during an unprecedented and prolonged stressor. Furthermore, these data were collected before and within the first year of the COVID-19 pandemic and may not be reflective of the longer term effects of the pandemic on work culture. Notably, the results collected during the pandemic were before a vaccine being announced and made available to HCWs and before the emergence of the highly contagious delta and omicron variants resulting in additional waves of infections and hospitalizations. Individual HCW and work setting–specific SCORE responses were not able to be linked; thus, results may not represent before and during results for the same individual HCWs given turnover. We are also relying on self-reported perceptions of culture, but this potential bias is mitigated by using a validated survey with strong psychometric properties, a large sample size, and a representative response rate. While our response rate is quite high for this type of survey, it is possible that the missing responses provide some degree of selection bias. Similarly, 18 facilities did not have prepandemic survey data to report. The imbalance of healthcare role representation in the study may have skewed our findings toward the perceptions of a particular role, such as nursing.
We also did not have access to race, ethnicity, and gender demographic membership, which also likely affect team member experience and would be important to consider in future studies. Finally, given that work culture is local, we would have ideally been able to study the effect of teamwork climate at the work setting level rather than the facility level, but those linked data were unavailable.
CONCLUSIONSMaintaining teamwork norms and behaviors during times of crisis has long been touted as essential to support the safety of our patients and well-being of our workforce. In this unique data set, facilities that suffered a decline in teamwork climate, relative to those that did not, were faced with simultaneous negative impacts to safety culture and workforce well-being. Maintaining specific teamwork norms under pressure, particularly those related to psychological safety, was associated with maintaining safety culture overall as well as HCW well-being. Proactive team training may provide substantial benefit to team performance and team member well-being during stressful times.
REFERENCES 1. Sexton JB, Helmreich RL, Neilands TB, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6:44. 2. Sexton JB, Adair KC, Leonard MW, et al. Providing feedback following Leadership WalkRounds is associated with better patient safety culture, higher employee engagement and lower burnout. BMJ Qual Saf. 2018;27:261–270. 3. Nieva VF, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. Qual Saf Health Care. 2003;12 suppl 2:ii17–ii23. 4. Agency for Healthcare and Research Quality. Quality and Patient Safety Resources. Available at: http://www.ahrq.gov/patient-safety/resources/index.html. Accessed September 27, 2021. 5. Sexton JB, Makary MA, Tersigni AR, et al. Teamwork in the operating room: frontline perspectives among hospitals and operating room personnel. Anesthesiology. 2006;105:877–884. 6. Sexton JB, Holzmueller CG, Pronovost PJ, et al. Variation in caregiver perceptions of teamwork climate in labor and delivery units. J Perinatol. 2006;26:463–470. 7. Blegen MA, Pepper GA, Rosse J. Safety climate on hospital units: a new measure. In: Henriksen K, Battles JB, Marks ES, et al., eds. Advances in Patient Safety: From Research to Implementation (Volume 4: Programs, Tools, and Products). Advances in Patient Safety. Rockville, MD: Agency for Healthcare Research and Quality (US); 2005. Available at: http://www.ncbi.nlm.nih.gov/books/NBK20592/. Accessed September 29, 2021. 8. Sacks GD, Shannon EM, Dawes AJ, et al. Teamwork, communication and safety climate: a systematic review of interventions to improve surgical culture. BMJ Qual Saf. 2015;24:458–467. 9. Schmutz JB, Meier LL, Manser T. How effective is teamwork really? The relationship between teamwork and performance in healthcare teams: a systematic review and meta-analysis. BMJ Open. 2019;9:e028280. 10. Tannenbaum SI, Traylor AM, Thomas EJ, et al. Managing teamwork in the face of pandemic: evidence-based tips. BMJ Qual Saf. 2021;30:59–63. 11. Sexton JB, Adair KC. Forty-five good things: a prospective pilot study of the Three Good Things well-being intervention in the USA for healthcare worker emotional exhaustion, depression, work-life balance and happiness. BMJ Open. 2019;9:e022695. 12. Adair KC, Kennedy LA, Sexton JB. Three Good Tools: positively reflecting backwards and forwards is associated with robust improvements in well-being across three distinct interventions. J Posit Psychol. 2020;1–10. 13. Sexton JB, Adair KC, Profit J, et al. Safety culture and workforce well-being associations with positive Leadership WalkRounds. Jt Comm J Qual Patient Saf. 2021;47:403–411. 14. Pierce RG, Maples WJ, Krippner J, et al. Results from the National Taskforce for Humanity in Healthcare’s integrated, organizational pilot program to improve well-being. Jt Comm J Qual Patient Saf. 2021;47:581–590. 15. Rink LC, Silva SG, Adair KC, et al. The association between well-being behaviors and resilience in health care workers. West J Nurs Res. 2022;44:743–754. 16. Tawfik DS, Shanafelt TD, Dyrbye LN, et al. Personal and professional factors associated with work-life integration among US physicians. JAMA Netw Open. 2021;4:e2111575. 17. Schwartz SP, Adair KC, Bae J, et al. Work-life balance behaviours cluster in work settings and relate to burnout and safety culture: a cross-sectional survey analysis. BMJ Qual Saf. 2019;28:142–150. 18. Sexton JB, Schwartz SP, Chadwick WA, et al. The associations between work-life balance behaviours, teamwork climate and safety climate: cross-sectional survey introducing the work-life climate scale, psychometric properties, benchmarking data and future directions. BMJ Qual Saf. 2017;26:632–640. 19. Rehder KJ, Adair KC, Hadley A, et al. Associations between a new disruptive behaviors scale and teamwork, patient safety, work-life balance, burnout, and depression. Jt Comm J Qual Patient Saf. 2020;46:18–26. 20. Nunnally JC. Psychometric Theory. New York, NY: McGraw Hill; 1967. 21. Nunnally JC, Bernstein IH. Psychometric Theory. New York, NY: McGraw-Hill; 1994. 22. Weaver SJ, Rosen MA, DiazGranados D, et al. Does teamwork improve performance in the operating room? A multilevel evaluation. Jt Comm J Qual Patient Saf. 2010;36:133–142. 23. Baker DP, Day R, Salas E. Teamwork as an essential component of high-reliability organizations. Health Serv Res. 2006;41:1576–1598. 24. Sexton JB, Adair KC, Profit J, et al. Perceptions of institutional support for “second victims” are associated with safety culture and workforce well-being. Jt Comm J Qual Patient Saf. 2021;47:306–312. 25. Ford K, Menchine M, Burner E, et al. Leadership and teamwork in trauma and resuscitation. West J Emerg Med. 2016;17:549–556. 26. Nishisaki A, Nguyen J, Colborn S, et al. Evaluation of multidisciplinary simulation training on clinical performance and team behavior during tracheal intubation procedures in a pediatric intensive care unit. Pediatr Crit Care Med. 2011;12:406–414. 27. Lauridsen KG, Krogh K, Müller SD, et al. Barriers and facilitators for in-hospital resuscitation: a prospective clinical study. Resuscitation. 2021;164:70–78. 28. Kannampallil TG, Goss CW, Evanoff BA, et al. Exposure to COVID-19 patients increases physician trainee stress and burnout. PLoS One. 2020;15:e0237301. 29. Pappa S, Ntella V, Giannakas T, et al. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. 30. Elbay RY, Kurtulmuş A, Arpacioğlu S, et al. Depression, anxiety, stress levels of physicians and associated factors in COVID-19 pandemics. Psychiatry Res. 2020;290:113130. 31. Mosheva M, Hertz-Palmor N, Dorman Ilan S, et al. Anxiety, pandemic-related stress and resilience among physicians during the COVID-19 pandemic. Depress Anxiety. 2020;37:965–971. 32. Thomas EJ, Sexton JB, Neilands TB, et al. The effect of executive walk rounds on nurse safety climate attitudes: a randomized trial of clinical units. BMC Health Serv Res. 2005;5:28. 33. Quan SD, Morra D, Lau FY, et al. Perceptions of urgency: defining the gap between what physicians and nurses perceive to be an urgent issue. Int J Med Inform. 2013;82:378–386. 34. Jones KJ, Skinner AM, High R, et al. A theory-driven, longitudinal evaluation of the impact of team training on safety culture in 24 hospitals. BMJ Qual Saf. 2013;22:394–404. 35. Thomas L, Galla C. Building a culture of safety through team training and engagement. BMJ Qual Saf. 2013;22:425–434. 36. Spiva L, Robertson B, Delk ML, et al. Effectiveness of team training on fall prevention. J Nurs Care Qual. 2014;29:164–173. 37. Jain M, Miller L, Belt D, et al. Decline in ICU adverse events, nosocomial infections and cost through a quality improvement initiative focusing on teamwork and culture change. Qual Saf Health Care. 2006;15:235–239. 38. Armour Forse R, Bramble JD, McQuillan R. Team training can improve operating room performance. Surgery. 2011;150:771–778. 39. Sawyer T, Laubach VA, Hudak J, et al. Improvements in teamwork during neonatal resuscitation after interprofessional TeamSTEPPS training. Neonatal Netw. 2013;32:26–33. 40. Adair KC, Quow K, Frankel A, et al. The Improvement Readiness scale of the SCORE survey: a metric to assess capacity for quality improvement in healthcare. BMC Health Serv Res. 2018;18:975.
留言 (0)