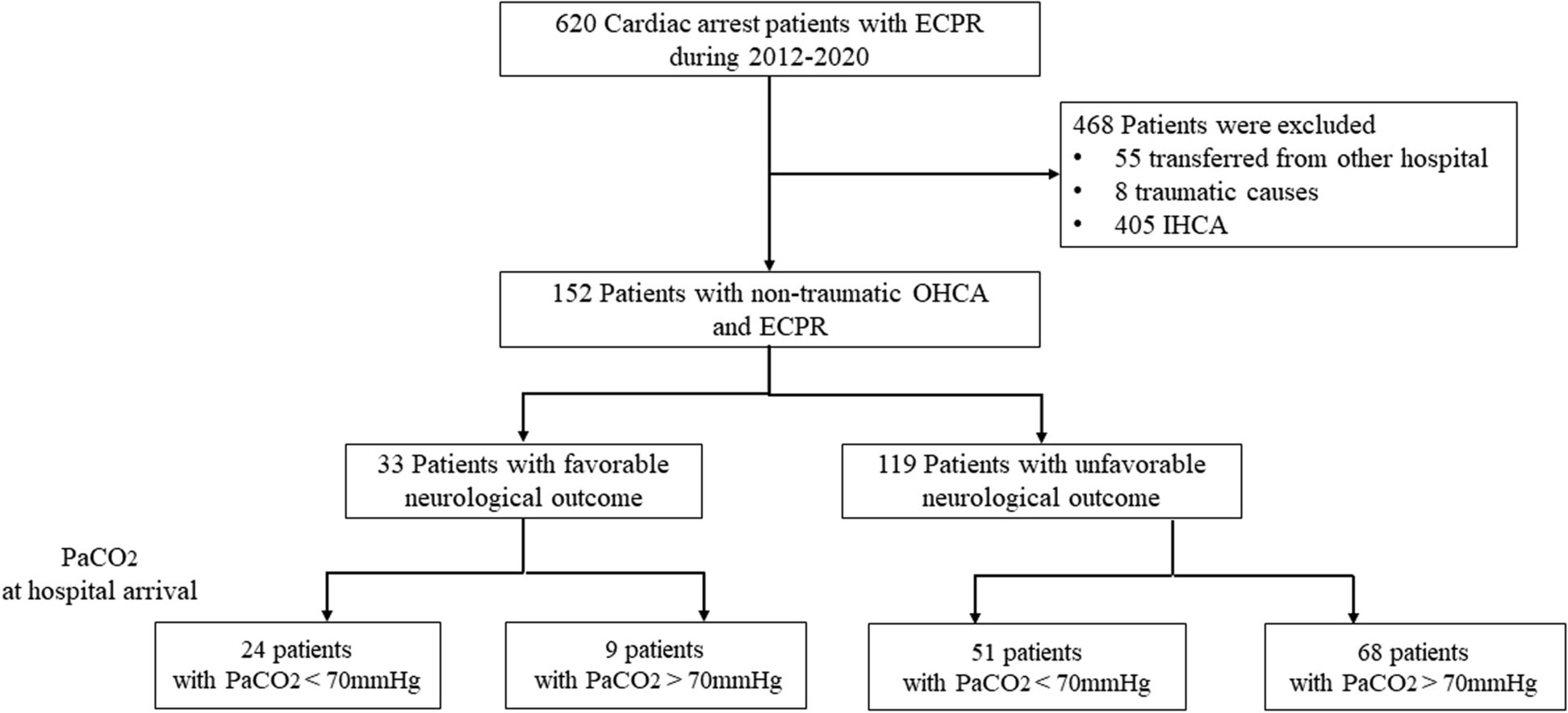
During an observational period of one year, out of 758 patients treated by a PEMT for ACS symptoms at the EMS Bonn (Germany), 9 patients (1.2%, CI 0.5–2.2%) were characterized by simultaneous chest pain and misinterpreted neurological deficits upon initial presentation and ultimately diagnosed with an ACD mimicking an ACS. To our knowledge, this is the first time the incidence of misdiagnosed ACD for suspected ACS has been evaluated in the prehospital setting and our reported incidence is higher compared to previous reports of the “stroke chameleon” in the clinical setting [9]. Considering that neurological disorders account for approximately 7% of all emergency cases in a representative German study [10], 1.2% misdiagnosed patients seem a relevant amount. Within the herein evaluated EMS, this would result in one misdiagnosed patient every six weeks.
ACS and ACD seem different in pathogenesis and clinical presentation. As observed by Cushing, both share common features such as chest pain, elevated troponin and ECG changes [2]. These symptoms and clinical manifestations, subsumed as neurogenic stunned myocardium (NSM) or stroke chameleon, may explain why, sporadically, suspected ACS proves to be an ACD. We present a retrospective analysis evaluating the quantity of ACD within suspected ACS in a prehospital setting, and potentially discriminating features.
Correct out of hospital discrimination between ACS and ACD is important, because prehospital treatment differs relevantly, hospital allocation depends on prehospital diagnosis using current symptoms as well as medical history, and misallocation may delay time sensitive therapy. For suspected ACS, prehospital treatment includes antiaggregant therapy composed of ASA and heparin dosages [7]. For suspected cerebrovascular accidents, prehospital antiaggregant therapy is contraindicated: in case of haemorrhage per definition, in case of ischemia depending on the time of event and risk of secondary bleeding, defined by computed tomography (CT). In the present cohort, 5 patients in the ACD group (55.6%) received ASA and heparin boluses for suspected ACS. Two of these patients were diagnosed with ICH, 3 suffered from cerebrovascular accidents. Thus, the ICH patients were not only treated inadequately, but received contraindicated medication and were exposed to neurological deterioration. Fortunately, both patients did not develop further neurological deficits as compared to the time of hospital admission.
Out of hospital cardiac arrests (OHCA) were excluded from analysis. OHCA due to cerebrovascular accidents or ACS may mimic each other, but prehospital therapy does not differ, since ERC guidelines do not recommend thrombolytic drugs in suspected OHCA due to ACS [11]. Noteworthy, from a retrospective analysis comparing OHCA from SAH to OHCA from ACS, asystole or pulseless electrical activity seems to be a discriminating characteristic for OHCA due to SAH, especially in the absence of ST-segment deviations [12].
Available data on the link between ACS and ACD refer usually to cerebrovascular accidents [5, 13, 14]. It is proposed, that insular involvement leads to autonomic dysregulation resulting in a catecholamine release, thus leading to myocardial dysfunction with wall movement abnormalities, ECG changes and elevated troponin levels [4]. Consistently, final diagnoses in the ACD group were TIA and ischemic stroke in 5 patients and ICH in 2 patients. Interestingly, one patient suffered from neuroborreliosis and one had a suspected combination of anterior spinal artery TIA and panic attack. Spinal ischemia and myelitis, which may involve the sympathetic nervous system, seem conceivable and have been described in two case reports previously [15, 16]. Sole emotional stress may induce NSM, too, with regard to its previous term of “broken heart syndrome” [17]. Neuroborreliosis as trigger for NSM has not been described, yet. Since neuroborreliosis mainly manifests in neuritis and infectious causes for NSM are rare, its causal relation remains unclear, but NSM induced by limbic encephalitis has been described [18].
Discriminating features for ACD in this population are a history of ICH (OR 19, p = 0.01), headaches on presentation (OR 10.1, p = 0.03) or general appearance of neurological symptoms (OR 16.9, p = 0.01). Although seemingly obvious, correct diagnosis was probably confounded by co-existence of chest pain and ECG changes. This is in concordance with statistical analysis, that revealed no difference between groups regarding chest pain and ECG changes. Statistically, GCS was more often reduced in ACD (2 vs. 7 cases with GCS < 15, p = 0.03), advocating its value as indicator for neurological disorders.
A definite and certain distinction between ACS and ACD cannot be accomplished in a prehospital setting, since diagnoses rely on laboratory and imaging results. The use of point of care troponin tests might be helpful in discriminating ACS, but false negative tests must be considered due to delayed increase of serum troponin levels after onset of symptoms. More importantly, elevated troponin levels are well described in ACD patients. [4, 5] Thus, point of care troponin tests will not aid in discriminating ACS from ACD patients prehospitally. Prehospital echocardiography is not established within the EMS Bonn, but is evolving generally, and might be a helpful tool for the experienced emergency physician. Again, ventricular wall motion abnormalities have been described in ACD patients, not allowing a certain differentiation between ACS and ACD in the prehospital setting. [19] Obviously, cerebral imaging to verify or exclude ACD diagnosis is not available. Given these aspects, emergency physicians have to rely and decide on a focused patient history and careful examination. From the presented cohort, appearance of neurological symptoms or reduced GCS might be the “red flags” in discriminating ACD from ACS and should be considered carefully.
From a retrospective analysis, Bulsara et al. proposed criteria to differentiate ACS from NSM in a clinical setting: missing history of heart disease, new onset of cardiac dysfunction defined as ejection fraction (EF) < 40%, wall motion abnormalities discordant to ECG changes and troponin < 2.8 ng/ml in patients with EF < 40% [19]. In the present cohort, only a missing history of arterial hypertension in the ACD group (OR 0.22, p = 0.03) was differentiating. Since arterial hypertension is a common risk factor for heart disease, this is consistent with Bulsara’s NSM criteria. In contrast, from a retrospective multicenter registry study on clinical differences between ACS and stroke, arterial hypertension was more prevalent in stroke patients. Subgroup analysis of female patients revealed no difference in history of arterial hypertension between ACS and stroke patients [20]. It must be considered, that in the presented study, ACD was not compared to the correctly diagnosed ACS patients, but to suspected ACS patients, which might explain these seemingly contradictory results. Also, a subgroup analysis of female patients was not performed, since data, especially regarding ACD group, was underpowered.
Recent investigations on ICH concomitant to ACS reveal its rareness (0.2–0.4%) but also point out the poorer overall outcome [21, 22]. In both studies patients with concomitant ICH received more antiaggregant drugs. It may be speculated, that ICH was a complication due to therapy for ACS as opposed to the presented cases with suspected NSM. Final certainty on what is cause and what is effect may never be reached, though.









留言 (0)