The present study employed novel methods, including NLP and network analysis, to help physicians provide timely palliative care for patients withdrawing from life-sustaining treatments. The study results suggest that broad-spectrum antibiotics, antifungal agents, diuretics, albumin, and opioids are associated with early palliative consultation. Patients and families who withdraw life-sustaining treatments experience physical, emotional, and psychological challenges. Proper and timely palliative care referrals can help establish treatment goals, improve symptom control, and provide psychological support to patients and their families. However, in current clinical practice, most patients receive palliative care extremely late in the end-of-life stage.
Although early palliative care has gradually gained acceptance, the widespread integration of palliative care with standard medical treatment remains insufficient [19]. Therefore, the early recognition of patients’ palliative needs and possible triggers is important for achieving positive healthcare outcomes. Previous studies have reported that palliative triggers, such as advanced or life-limiting diseases, as well as characteristics of hospitalization, are associated with higher resource utilization and negative outcomes [20]. The medication-related palliative triggers identified by the NLP and network analysis in this study can be applied to computer triage systems in the future.
Medications with a high Palliative trigger index included antibiotics (cefepime, vancomycin, and ceftazidime), antifungal agents (fluconazole), opioids (morphine and fentanyl), furosemide, albumin, and amiodarone. The use of broad-spectrum antibiotics and antifungal agents indicated that the patient had a severe infection. Severe sepsis is the leading cause of death in ICUs [21]. Opioids are the primary treatment for pain related to advanced and progressive diseases, especially when withdrawing life-sustaining measures [22]. Furosemide and albumin are used to treat fluid retention [23]. The possible etiologies of fluid retention included fluid infusions during acute resuscitation, chronic cardiac disease, and renal disease, among others [23, 24]. Amiodarone is a potent antiarrhythmic agent used to treat ventricular arrhythmias and atrial fibrillation [25]. Overall, the use of medications with a high Palliative trigger index indicated that the patient was critically ill. Therefore, these data can serve as a reasonable trigger for physicians to recommend timely palliative care.
Network analysis enables the categorization of medications that often occur together in the medical records of the same patient. The co-occurrence of micafungin and voriconazole in the early integration group could be explained by the synergistic effects of severe systemic fungal infections in severely ill patients. Clinicians should adjust antifungal agents according to cultural evidence and clinical presentation, thereby increasing the co-occurrence of various antifungal agents. A possible explanation for the co-occurrence of albumin and furosemide in the early integration group is that both drugs are usually co-administered to correct the reduced oncotic pressure and reinforce their therapeutic effect [26].
In the late referral group, piperacillin and penicillin showed high co-occurrence. Piperacillin-tazobactam is a common choice for both directed and empirical treatment of critically ill patients [27]. Piperacillin is a broad-spectrum penicillin antibiotic, which may explain its co-occurrence. Bevacizumab and capecitabine also showed a high co-occurrence in the late referral group. The combination of bevacizumab and capecitabine is an effective and well-tolerated regimen for elderly patients with metastatic colorectal cancer [28]. This co-occurrence indicates that the patients were undergoing aggressive anticancer treatments.
Network analysis revealed several important patterns of medication use. Interestingly, there was some overlap between the high co-occurrence medications in the early integration group and high Palliative trigger index medications, such as albumin, furosemide, and antifungal agents. This observation reveals that high Palliative trigger index medications are often prescribed together, which indicates that these drugs share some common characteristics.
NLP can be used to automatically extract clinically relevant information, thereby reducing the time required by clinicians to extract salient information manually. In the future, these medical term data can be used to establish a triage system to identify the initial priorities of clinicians for the early integration of specialist palliative care. According to a previous study, a computerized order-entry-based therapeutic control system can remind physicians to perform Hepatitis B virus (HBV) screening before prescribing chemotherapy [29]. We may also apply a similar computerized order-entry-based therapeutic control system to integrate palliative care before the patient withdraws from life-sustaining treatments. When physicians prescribe broad-spectrum antibiotics, antifungal agents, or opioids, the computerized order-entry-based therapeutic control system can prompt them to evaluate whether the palliative team should be consulted. Furthermore, referral triggers can also be integrated into SDM. Palliative consultants and multidisciplinary teams can assist ICU teams in imparting high-quality communication, exploring all possible preferences, and making sound clinical decisions.
Limitations
Although the present study reveals important findings, it has several limitations.
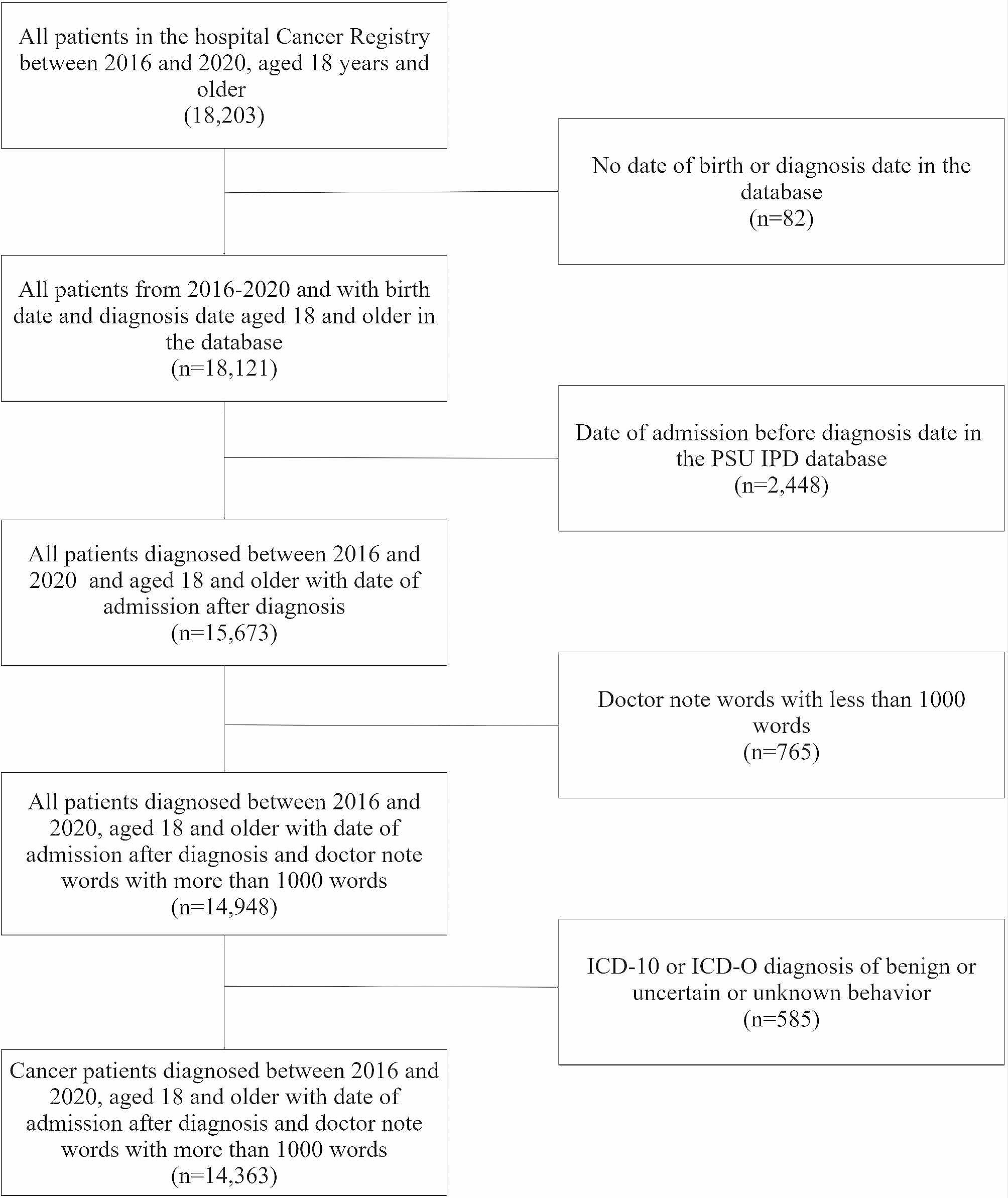
First, it was a single-center study. The sample size was relatively small, and only 119 patients were included in the final analysis. The participants only included Taiwanese citizens; therefore, the results may not reflect populations in other countries.
In addition, owing to the retrospective nature of the study, the causality between medications and palliative referral cannot be fully confirmed. The admission course of the early integration group might have been longer than that of the late referral group, which may have caused a possible bias because the early integration group had more opportunities for different medical terms in their medical notes.
In addition, there are many synonyms in use, including generic names, brand names, and abbreviations, which increases the difficulty of machine identification. Currently, synonyms, such as generic names and brand names, must be manually combined. The present study did not include patient symptoms or psychosocial or cultural factors in our analysis. As many of these factors were recorded in Chinese, they may have increased the difficulty of the analysis. The accuracy of NLP requires further improvement in future studies.
Patients with different diagnoses, in addition to medications, have different treatment courses and may influence end-of-life care. In this study, we did not perform disease-group-based NLP, which could be a potential source of bias. However, we believe that all patients in ICUs receiving life-sustained withdrawal treatments were in the terminal stages and had a similar prognosis and time for palliative care referral, regardless of disease type. In addition, the sample size for each disease was small, making it difficult to determine if a particular result is a true finding. Thus, we focused on all ICU patients who underwent endotracheal tube withdrawal and did not perform a subgroup analysis.
The Palliative trigger index is a novel method for evaluating palliative triggers. But it still needs further reliability and validity analysis in the future. High Palliative Trigger Index words could also be found in ICU patients who are not approaching to the end of life soon. Additional studies should be performed to check the incidence and value of the Palliative trigger index in non-end-of-life ICU patients to confirm our findings. Future studies can also extend the word of interest to NLP, enroll more participants, and focus on the outcomes of patients after the application of a therapeutic control system based on the computerized order entry.









留言 (0)