
記住我



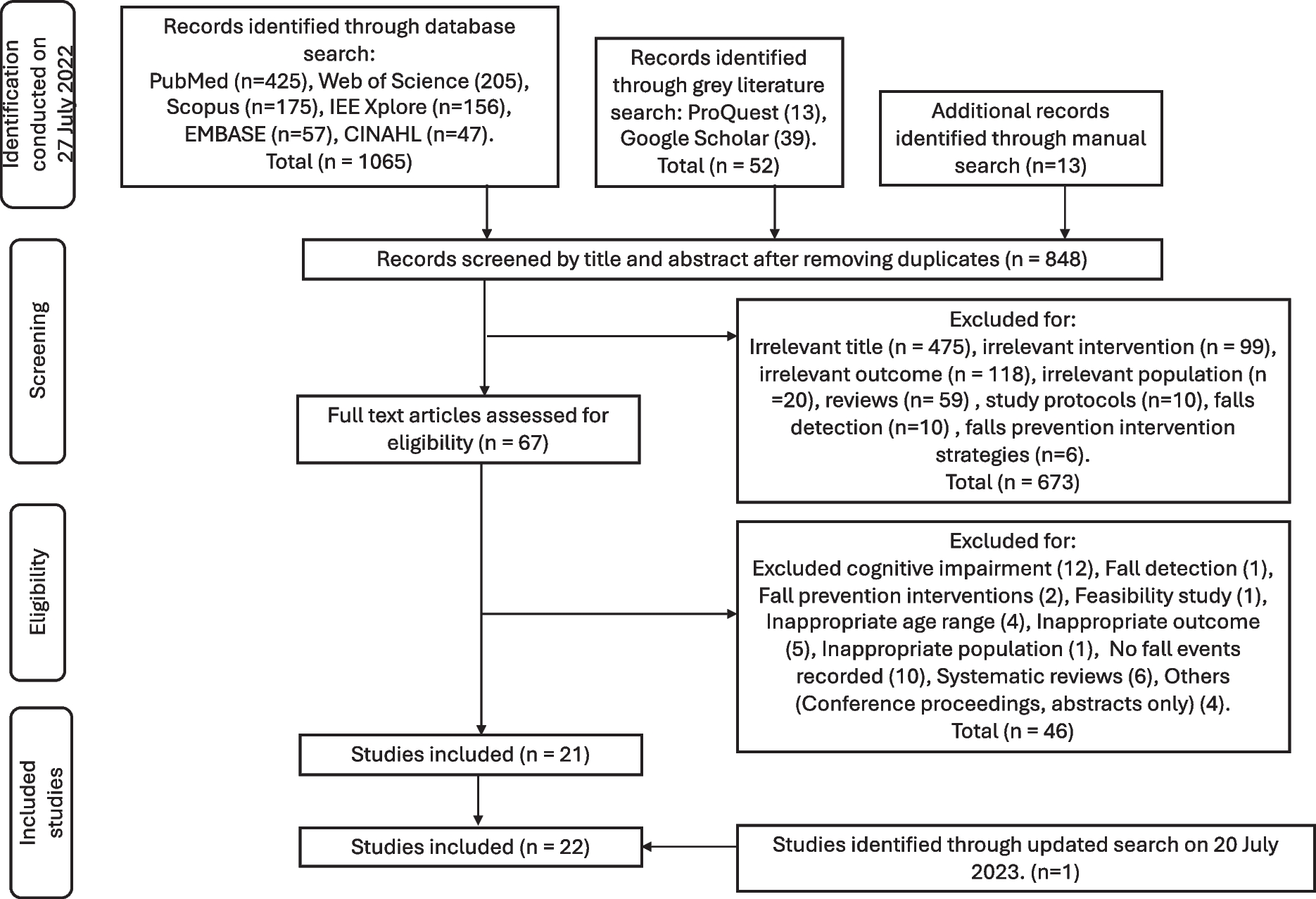




A total of 216 adults were recruited for this study out of 592 screened individuals. Due to attrition and missing data, 191 adults were included in the final analyses (138 females and 53 males). A full accounting of recruitment, sample size, and attrition is presented in Fig. 1. To be included, a participant had to be between the ages of 45 and 75 years, be fluent in English, own a smartphone, be willing to communicate via text message, and have at least two of the following risk factors for ADRD based on the Australian National University–Alzheimer’s dementia risk index (ANU-ADRI): high school education or less; a body mass index (BMI) ≥ 25 kg/m2 but less than 40 kg/m2; or history of diabetes, hypertension, high cholesterol, smoking, or traumatic brain injury. Participant exclusion criteria were visual problems impacting the ability to view a screen at a normal distance; history of a learning disability; recent cardiovascular event; current participation in a cognitive training intervention or lifestyle change program; current diagnosis of any mental health condition, neurologic condition, dementia, mild cognitive impairment, or any other serious health condition; or more than one of the following ADRD protective factors based on the ANU-ADRI: high physical activity level, eating non-fried fish or seafood more than 5 times per week, or a high level of cognitive engagement.
Fig. 1
Study recruitment flowchart
Required sample size was determined a priori by utilizing both a mathematical and practical approach. Mathematically, total sample size requirement was calculated using G*Power 3.1.9.7 [17] based on the primary statistical test planned for this study (2 × 2 mixed factorial ANOVA). Calculations were based on an alpha level of 0.05, a statical power of 0.8, and a small effect size (ηp2 = 0.02 or d = 0.2). The largest required sample size returned from mathematical analyses was a total sample of 100 total participants. Practical analyses for required sample size were conducted by examining related HC literature and the samples recruited to demonstrate efficacy therein. Studies examining the efficacy of HC on improving psychological and cognitive variables were conducted with sample sizes ranging from 40 to 45 total participants and demonstrated significant improvement in outcome measures [14, 15, 18]. Taken together, a sample size of at least 100 participants was pursued for this study.
A convenience sampling procedure was utilized in this study. Participants were recruited through advertising on National Public Radio, advertising on a university newswire service, social media, and word of mouth. Potential participants expressing interest in the study were emailed a link to an inclusion/exclusion survey instrument which was used to determine whether they were a candidate for the study.
Study designThis study followed a parallel arm trial design wherein participants were randomized into one of two groups (HC or HE) with an equal allocation ratio and then scheduled for an initial visit to the laboratory to complete a testing session. Randomization was achieved by pre-assigning all study IDs to an arm using a binary random number generator with an equal allocation randomization rule for the full recruited sample size. As participants entered the study, they were sequentially assigned an ID number and assigned to the corresponding study arm. No form of blinding was utilized in this trial. The randomization sequence was generated by the principal investigator, and study enrollment as well as formal trial arm assignment was carried out by the study coordinator.
MeasuresThree primary outcomes were assessed in this study. First, the participant’s self-reported global cognition was collected as a measure of their own perception of their cognitive state. Self-reported global cognition, although subjective, is a valid and reliable predictor of cognitive state [19] and is sensitive to detection of mild cognitive impairment [20]. Second, neuropsychological cognition was assessed as an overall objective measure of a participant’s cognitive state. Multidimensional neuropsychological cognition assessment batteries are the accepted gold standard for objective cognitive assessment, and these instruments are generally used in both the research and clinical setting to discriminate between individuals with and without cognitive impairment [21, 22]. Third, Alzheimer’s risk was assessed as both a risk measure (positive risk), protection measure (negative risk), as well as a composite risk score taking into account both risk and protection. In long-term follow-up studies, Alzheimer’s risk data obtained from survey instruments has good predictive validity for determining future ADRD diagnoses within 3–6 years following testing [23].
Global cognitionThe Everyday Cognition (ECog-12) survey was used to assess self-reported global cognition. The ECog-12 is a self-reported survey instrument that asks participants to compare their current state of cognition to their cognitive state 10 years in the past [19]. Each of the survey’s 12 items use a 4-point scale, with higher values indicating greater cognitive impairment [19]. The ECog-12 is reliable and valid, and has excellent discriminant ability for separating participants with clinical cognitive impairment from individuals with normal cognitive function [19].
Neuropsychological cognitive abilityThe Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) was used to assess neuropsychological cognition. The RBANS assessment is a digital assessment presented to participants on a tablet and administered by a trained test administrator. Participants are asked to complete several cognitive/memory tests including repeating words and stories, drawing geometric shapes, identifying pictures, and matching symbols with numbers from a given key [24]. The assessment evaluates five neuropsychological construct domains: immediate memory, visuospatial/constructional, language, attention, and delayed memory. Scores from the five domains were adjusted based on age and level of education, and combined to yield a single, continuous index score indicating overall neuropsychological cognitive ability [24]. RBANS is a valid and reliable instrument for measuring neuropsychological cognitive domains and overall ability [25].
Alzheimer’s riskThe ANU-ADRI is a self-report inventory assessing Alzheimer’s risk across several positive and negative risk factors [10]. Protective (negative risk) factors examined are social engagement, cognitive activity, physical activity level, non-fried fish and seafood consumption, and alcohol consumption (if less than 2 drinks per day). Risk (positive risk) factors assessed in this survey are diabetes diagnosis, depression status, obesity, history of traumatic brain injury, history of smoking, high cholesterol, high alcohol consumption (3 or more drinks per day), exposure to pesticides, as well as known demographic risk factors such as sex, age, and level of education [10]. The ANU-ADRI is a valid [23] and reliable [26] measure of Alzheimer’s risk.
Data collectionParticipants who were identified as candidates for inclusion in the study upon completion of the initial inclusion/exclusion survey were asked to complete a digital copy of an informed consent document. The study, all recruiting procedures, and informed consent were approved by the Institutional Review Board at a major, land-grant institution of higher education. Participants returned a digitally signed informed consent. In addition to this first session, participants completed a second session approximately 4 months from the first.
Prior to arriving for each testing visit, participants were asked to complete one additional digital survey remotely to collect demographic and health status data. This demographic and health survey contained the ECog-12 survey and questions designed to collect relevant demographic information such as age, sex, and level of education. Other information was collected by the demographic and health survey which was not utilized in the present analysis including healthcare utilization, diagnosed medical conditions, prescribed medications, self-reported health status, depression status, and sleep quality status. If this survey was not completed remotely before each appointment, completing it was the first task assigned to participants upon arrival at the laboratory.
Arriving at the laboratory (or after completing the demographic and health survey if not completed beforehand), participants were asked to complete the ANU-ADRI assessment on a provided laptop. Although the inventory is self-guided, a researcher was present to answer any questions the participant may have had regarding the ANU-ADRI. Following completion of the ANU-ADRI, basic cardiovascular and anthropometric data were collected from participants. Blood pressure was collected manually by a trained researcher using a standard inflatable sphygmomanometer cuff and stethoscope, and pulse rate was collected with a standard pulse oximeter on the finger. Weight was collected using a beam-balance physician’s scale, and height was collected using a stadiometer.
The RBANS assessment was administered roughly 20 min after the cardiovascular and anthropometric assessments. The RBANS test is produced in multiple versions utilizing the same battery of tests but make slight changes to the presentation of words, figures, and numbers to mitigate learning effects from test to re-test [24]. For this study, the RBANS Form A was administered in the first appointment and Form B in the second. The RBANS tests were graded by a trained and experienced rater in accordance with procedures from the RBANS manual [24]. Data were recorded by researchers and input into a master database for analysis.
As this present analysis was performed as a part of a larger study, other data were collected but not utilized here. Participants completed other measures of body composition and physical function that are not germane to the analysis presented here. The full protocol for the DC MARVel Study is described elsewhere [16].
InterventionHealth coachingParticipants randomized into the HC intervention were assigned to a trained health coach who worked with them throughout the study’s duration. HC is unique in the set of health and lifestyle interventions typically examined in research in that it does not follow a standardized approach. Rather, it works within a set of principles and practices to provide a personalized intervention to participants. After the first visit to the laboratory, participants were scheduled to have an initial video conference or phone call with their health coach wherein they discussed the HC process, were educated about lifestyle domains and their impact on cognitive health, described to the coach which domains they wanted to change, assessed their motivation and willingness to change, and established goals to achieve their desired future vision. The health coach focused on improving cognitive health through targeting the following lifestyle domains: nutrition, physical activity, sleep, stress, social engagement, and cognitive activity. The specific intervention for each participant is formulated within that framework and the decision of which modifiable risk factors to focus on is made based on the participant’s preferences and the coach’s recommendation.
During the intervention, the participant and coach communicated monthly via video conference or phone call, and the coach reached out to participants 1–2 times per week via text messaging app and email. In monthly meetings, the coach checked progress, assessed readiness for progression, discussed obstacles, and strategized about how the intervention would be implemented subsequently. More frequent weekly messages and emails to participants would provide personalized education materials based on the specific participant’s current goals. HC participants were also provided access to a cognitive health app (Citruslabs, Santa Monica, CA), where they can access cognitive training activities, workout routines, and recipes, and were instructed to interact with the app at least 3 times per week. Adherence to the HC protocol was defined as the completion of at least one HC appointment between baseline and the 4-month time point. The health coach recorded all adherence data for each de-identified participant in an online database.
Health educationParticipants randomized into the HE intervention received a biweekly email that included educational material outlining how they could improve cognitive health through lifestyle change. Participants were asked to read each email when they received it, and the emails were designed to be eye-catching and engaging. The same lifestyle domains addressed in HC were utilized as topics in HE to allow for better direct comparison between interventions without adding an additional source of variability. Outside of scheduling and basic communication, HE participants only had access to study staff during their on-site testing appointments.
Data analysisAll data analyses were performed using SPSS 27 (IBM Corp, Armonk, NY). Means, standard deviations, and 95% confidence interval of the mean were calculated for all continuous dependent, demographic, and anthropometric variables. Before completing any inferential statistical tests, all relevant assumptions were checked, and if they were met, statistical analysis was allowed to proceed. Prior to hypothesis testing, an independent samples t-test was utilized to determine if there were differences in baseline cognitive scores (ECog-12 and RBANS) due to sex. Another independent samples t-test determined if cognitive score differences existed between the HC and HE group at baseline. Dependent samples t-tests were utilized to determine if outcomes had changed from baseline to 4 months with each intervention group (HC and HE). A 2 × 2 (intervention × time) mixed factorial ANOVA was utilized to determine if a difference in cognitive scores obtained in the first and second visit was dependent on intervention (HC or HE). That is, to determine if there was a significant intervention × time interaction effect. If baseline sex differences were found in cognitive scores, sex was included as a blocking factor to better isolate the effect of intervention and time. An a priori alpha level of 0.05 was used for all analyses.
留言 (0)