
記住我
Dietary high sodium intake is known to be associated with a range of health outcomes, such as hypertension, cardiovascular disease, and death [1]. A growing body of evidence suggests that night-time blood pressure and a nondipper or riser pattern of night-time blood pressure are independently associated with total cardiovascular event rates, especially in heart failure [2], where the elevation of night-time blood pressure or nondipper patterns are associated with increased circulating volume, which is largely determined by sodium intake [3].
Observational studies [4,5] have also demonstrated the potential role of sodium intake in obesity, that is, sodium intake is positively correlated with urinary sodium and body mass index (BMI). High sodium intake and obesity, both prevalent worldwide, are shared risk factors for many chronic diseases, and they also have adverse health consequences and disease burdens.
The left atrium (LA) is increasingly regarded as a bellwether, with its function providing critical prognostic information as a diagnostic of subclinical disease [6], indicating diastolic dysfunction [7]. The LA is a dynamic structure. LA function has three phases, serving as a reservoir in systole, as a conduit in early diastole, and as a booster in late diastole [8]. Myocardial strain analysis is a relatively new technique for determining the function of the LA.
In addition, the close physiological relationship between LA and left ventricular (LV) suggests a decoupling between the functions of the two cardiac chambers, the left atrium, and left ventricle, which can also lead to heart failure and cardiac dysfunction [9]. A recent mesa study [10] indicates that the left atrioventricular coupling index (LACI), assessed by cardiovascular magnetic resonance imaging (CMR), defined as the ratio between the left atrial and LV end-diastolic volumes, has improved prognostic value in predicting heart failure events compared with traditional heart failure factors.
In recent years, cardiac magnetic resonance feature tracking (CMR-FT) has emerged as a new magnetic resonance technology that enables high spatial resolution and superior contrast. Stability and repeatability are advantageous [11]. More crucially, several CMR-FT investigations [12,13] on LA strain and strain rate (SR) have demonstrated high inter-and intraobserver repeatability.
Urinary sodium is a surrogate indicator for sodium intake [14], with 24-h urinary sodium regarded as the gold standard method [15]. An earlier study reported the effects of sodium intake (represented by 24-h urinary sodium replacement) on LV function [16], but no research has focused on the effects of sodium intake on LA function and left atrioventricular coupling.
Thus, we investigated the relationship between 24-h urinary sodium, a surrogate measure of sodium intake, and cardiac MRI-assessed LA function and left atrioventricular coupling, with the assumption that in individuals without clinical heart failure, higher 24-h urinary sodium is associated with worse LA function (myocardial strain) and left atrioventricular coupling (expressed by the LACI). As previously described, sodium intake is closely related to blood pressure and BMI, so we used mediation analysis to investigate whether blood pressure and BMI are mediators in the relationship between 24-h urinary sodium and LA function and left atrioventricular coupling.
MATERIALS AND METHODS Study populationIn this study, 398 patients of higher economic status volunteered to undergo relevant examinations, including cardiac magnetic resonance imaging, 24-h urine collection, and 24-h ambulatory blood pressure measurement. They were recruited from the ward of the International Medical Department of the Second Affiliated Hospital of Dalian Medical University from December 2020 until December 2021. Obesity was defined according to the standard BMI as defined by the World Health Organization (WHO) (Asian cutoff ≥25 kg/m2) [17], and BMI was calculated as weight in kilograms divided by the square of height in meters. All participants were aged 20–90 years and had eaten regular meals for the past 1 month.
The exclusion criteria were as follows: secondary hypertension; coronary heart disease; HF with reduced ejection fraction (EF); moderate or severe valvular disease; atrial fibrillation; severe arrhythmia; cardiomyopathy; severe hepatic and renal dysfunction; stroke; malignant tumor; use of SGLT2i,Sodium-glucose cotransporter 2 inhibitor; use of glucocorticoids; and, finally, urine samples not able to be collected continuously throughout the day or whose 24-h urine volume is less than 500 ml.
All participants provided informed consent to participate in this study before enrollment. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Dalian Medical University and complied with the principles of the Declaration of Helsinki. A written informed consent form was obtained from each participant.
Biochemical testsAfter the participants had fasted for at least 8 h, venous blood was collected and analyzed. For participants on the regular diet, the participant's bladder was emptied and abandoned at 0700 h on the first day. All the urine discharged within 24 h of this time was stored, up until any last urination at 0700 h the next morning. Urinary sodium was determined by the electrode method and expressed as mmol/d. Renal function was represented by the estimated glomerular filtration rate (eGFR).
Blood pressure measurementAll patients were subjected to 24-h ambulatory BP monitoring using an oscillometric device (Spacelabs90207; Spacelabs, Snoqualmie, Washington, USA). The arm cuff was placed around the nondominant upper limb. Automatic BP recordings were obtained regularly every 30 min during the daytime period and every 1 h during the night-time period. The International Database of Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes criteria were used to define a complete ambulatory blood pressure (ABPM) measurement, defined as at least 10 daytime (1000–2000 h) and at least five night-time (midnight–0600 h) SBP and DBP measurements [18]. Then, ambulatory BP monitoring was removed, and these recordings for 24 h were used to obtain the mean 24-h, daytime, and night-time SBP, DBP, and HR, Heart rate were downloaded onto a computer and processed with the Medicom software International Database on ABPM. Patients were asked to attend to their daily activities, but to remain still while being measured. The patterns of night-time BP dipper were calculated based on the reduction in SBP while night-time vs. daytime: dippers (10–<20%); nondippers (0–<10%); and risers (night-time-to-daytime systolic BP [SBP] ratio >1.0) [19].
Conventional echocardiographyEach patient underwent an echocardiography examination, which was measured with a Vivid E9 ultrasound system (GE Vingmed Ultrasound, Horten, Norway). Transmitral inflow velocities were assessed during diastole by pulsed-wave Doppler and obtained with the sample volume placed between the tips of the mitral leaflets on the apical four-chamber view. The early diastolic (E) and late atrial (A) transmitral flow velocities were measured, and the E/A ratio was calculated. On the apical four-chamber view, pulsed-wave tissue Doppler was used to evaluating mitral plane movement. The early diastolic velocity of the myocardium (e′) was measured by placing the sample volume at the lateral mitral annulus.
MRI protocolAll MR measurements were performed using a 3.0-T whole-body scanner (Trio Tim; Siemens Medical Solutions, Erlangen, Germany) with a dedicated 32-channel body phased-array coil for when patients are in the supine position. Cardiac dimensions and function were assessed with ECG-triggered balanced steady-state free precession (b-SSFP) cine sequences during a brief breath-holding period. Cine images including three long-axis views (two-chamber, three-chamber, four-chamber) and two-chamber short-axis views were acquired (repetition time [TR] 3.4 ms, segments 12, echo time [TE] 1.31 ms, matrix size 208 × 139, the field of view [FOV] 234 mm × 280 mm, slice thickness 8 mm, and flip angle 39°).
Imaging analysis Left atrium feature-tracking analysisLA myocardial feature tracking (FT) analysis was performed using CVI42 software (Circle Cardiovascular Imaging, Inc., Calgary, Canada). The images were analyzed blinded to the individuals’ basic personal information (including age, sex, etc.). The LA endocardial (pulmonary veins and LA appendages were excluded) and epicardial borders were manually traced using a point-and-click technique in the two- and four-chamber images at the minimum LA volume following atrial contraction. In all two- and four-chamber views, the endocardial LA strain, and SR values were averaged across three tracking studies. The LA strain parameters included reservoir strain (LAs-s, which corresponds to atrial reservoir function at LV end-systole), conduit strain (LAs-e, which corresponds to atrial conduit function during early diastole), and booster strain (LAs-a, which corresponds to atrial booster function during late diastole). Thus, their associated SR characteristics, which include peak positive SR (SRs), peak early negative SR (SRe), and peak late negative SR (SRa), were obtained simultaneously.
Left atrium volumetric analysisManual tracings of the LA length and area were performed in the two-chamber and four-chamber long-axis views using CVI software. LA volume parameters were evaluated using the validated biplane area-length method according to a previously described formula [20]. LA appendages and pulmonary veins were excluded from the LA volume. For each of these phases, the maximum volume of LA (LAV) was defined at the left ventricle's end-systole and the minimum volume of LA (LAVmin) at the left ventricle's end-diastole [21].
Left atrioventricular coupling indexLACI was defined for each participant by the ratio between the LA end-diastolic volume and the LV end-diastolic volume assessed by CMR, as previously described. The LV volume was determined from the stack of short-axis cine images, while the LA volume was established from the two-chamber and four-chamber views. Both volumes were measured during the same end-diastolic phase, as determined by the closure of the mitral valve. This index is expressed as a percentage, and a higher LACI indicates a greater disproportion between the LA and LV volumes at the ventricular end-diastole, indicating a greater impairment of left atrioventricular coupling [22].
Left ventricular function and morphology analysisLV end-diastolic volume was calculated using Simpson's rule (the summation of areas on each separate slice multiplied by the sum of slice thickness and image gap). LV mass (LVM) was determined by the sum of the myocardial area (the difference between the endocardial and epicardial contour) times slice thickness plus the image gap in the end-diastolic phase multiplied by the specific gravity of the myocardium (1.05 g/ml) [23]. The LVM was indexed for BSA to determine the LVM index (LVMI). LVEF was calculated as LV stroke volume divided by LV end-diastolic volume multiplied by 100.
The LV feature tracking analyzes the radial, circumferential, and longitudinal strain on the standard CMR b-SSFP sequence using the same software as above. The LV endocardial and epicardial borders were manually drawn in the two-chamber, four-chamber, and short-axis view of the end-diastolic and the end-systole phase. The longitudinal strain and strain rate were obtained by tracking the long horizontal axis cines, whereas the circumferential, radial strain and strain rate were derived from the short-axis cines [24].
Statistical analysisCalculation of clinical features, laboratory data, and routine echocardiographic and CMR feature tracking parameters was carried out for all patients. We employed the designation of low, moderate, and high sodium intake which were based on current recommended intake (low), average intake (moderate), and above average intake (high) [25], the selected patients were divided into three groups according to 24-h urinary sodium, namely the low urinary sodium group: urinary sodium less than or equal 100 mmol/24 h (sodium intake ≤ 6 g/day), moderate urinary sodium group: 100 mmol/24 h < urinary sodium less than or equal 200 mmol/24 h (6 g/day < sodium intake ≤ 12 g/day), high urinary sodium group: urinary sodium at least 200 mmol/24 h (sodium intake >12 g/day).
All data were analyzed using SPSS statistical software (version 26.0; SPSS Inc., Chicago, Illinois, USA). Categorical data are presented as numbers (percentages) and were compared using the chi-square. Normally distributed continuous variables are expressed as the mean ± SD and were compared using a one-way analysis of variance (ANOVA). Pearson's or Spearman's correlation coefficient was used to analyzing the bivariable correlations as appropriate. Two-sided P values of <0.05 were considered to be statistically significant. Because night-time blood pressure and BMI are along the putative causal pathway between 24-h urinary sodium (a surrogate marker of estimated sodium intake) sodium and adverse left atrial function and left atrioventricular coupling, we performed mediation analysis to understand these indirect effects. We calculated the proportion explained by the intermediate factors as follows: 100% × [beta-coefficientmodel − beta-coefficientmodel+intermediatefactor]/[beta-coefficientmod-el] [26]. An application of Process V4.0's plug-in to investigate the mediating effect of BMI and night-time blood pressure on the effect of 24-h urinary sodium on left atrial function and left atrioventricular coupling was carried out.
RESULTS Characteristics of study participantsDescriptive characteristics of the study sample are displayed in Table 1, dichotomized by 24-h urinary sodium. A total of 398 patients were included in the study. The mean age was 55.70 ± 11.30 years, 58% were male, and obesity was common (mean BMI: 25.46 ± 3.78 kg/m2, 51.6% obese [BMI ≥ 25 kg/m2]). The lab results indicate that kidney function remained normal (eGFR: 118.89 ± 38.46 ml/min per 1.73 m2) and that there was a median 24-h urinary sodium 172.01 ± 80.24 mmol/day. No significant differences were observed between the groups in the application of ACEI/ARBs and diuretics (P > 0.05). In general, the study subjects were characterized by higher 24-h urinary sodium and higher rates of hypertension and obesity, as well as a higher BMI (P < 0.01).
TABLE 1 - Clinical and laboratory characteristics by 24-h urinary sodium in the study population All (n = 398) Low urinary sodium group (n = 58) Moderate urinary sodium group (n = 224) High urinary sodium group (n = 116) P Characteristic Age (years) 55.70 ± 11.30 57.29 ± 11.61 55.14 ± 11.35 55.99 ± 11.04 0.411 Height (cm) 169.75 ± 7.86 163.47 ± 6.11 169.39 ± 7.81∗ 173.62 ± 6.42 ∗# <0.001 Weight (kg) 73.81 ± 14.62 60.35 ± 9.30 73.25 ± 12.96∗ 81.70 ± 14.66 ∗# <0.001 Male, n (%) 231 (58) 6 (10.3) 118 (52.7) 107 (92.2) <0.001 BMI (kg/m2) 25.46 ± 3.78 22.57 ± 3.10 25.40 ± 3.24∗ 27.04 ± 4.17 ∗# <0.001 Medical history, n (%) Any alcohol use, n (%) 31 (7.8) 1 (1.7) 14 (6.3) 16 (13.8) 0.009 Smoker, n (%) 105 (26.4) 3 (5.2) 58 (25.9) 44 (37.9) <0.001 Diabetes, n (%) 171 (43.1) 15 (25.9) 99 (44.2) 57 (49.6) 0.011 Hypertension, n (%) 189 (47.5) 17 (29.3) 106 (47.3) 66 (56.9) 0.003 Obesity, n (%) 205 (51.6) 13 (22.4) 118 (52,7)∗ 74 (64.3)∗# <0.001 Antihypertensive medication, n (%) ACEI /ARB 73 (18.3) 9 (15.5) 40 (17.9) 24 (20.7) 0.68 β-Blocker (%) 27 (6.8) 1 (1.7) 12 (5.4) 14 (12.1) 0.017 CCB (%) 90 (22.6) 13 (22.4) 47 (21) 30 (25.9) 0.594 Diuretics (%) 11 (2.8) 0 (0) 9 (4) 2 (1.7) 0.18 Laboratory data Hs-CRP (mg/l) 1.68 ± 3.54 0.90 ± 1.76 1.84 ± 4.19 1.77 ± 2.69 0.204 BNP (pg/ml) 50.69 ± 233.84 38.39 ± 28.18 29.62 ± 27.26 105.46 ± 456.82# 0.106 FBG(mmol/l) 6.01 ± 2.06 5.21 ± 0.74 6.01 ± 1.91∗ 6.41 ± 2.63∗ 0.001 LDL-C (mmol/l) 2.99 ± 0.89 2.98 ± 0.85 3.02 ± 0.86 2.93 ± 0.97 0.687 TC (mmol/l) 5.14 ± 1.08 5.28 ± 1.08 5.17 ± 1.05 5.02 ± 1.14 0.305 TG(mmol/l) 1.80 ± 1.40 1.28 ± 0.58 1.81 ± 1.56∗ 2.04 ± 1.31∗ 0.003 eGFR (ml/min per 1.73 m2) 118.89 ± 38.46 112.87 ± 30.91 119.53 ± 41.56 120.68 ± 35.54 0.422 24-h urinary sodium 172.01 ± 80.24 72.76 ± 20.12 146.81 ± 27.52∗ 270.30 ± 67.90∗# <0.001Values are mean ± SD, or n (%).ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; BMI, body mass index; CCB, calcium antagonists; eGFR, estimated glomerular filtration rate; FPG, fasting plasma glucose; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides.
∗P < 0.05 vs. the low urinary sodium group.
#P < 0.05 vs. the moderate urinary sodium group.∗#P < 0.05 vs. the low and the moderate urinary sodium group.
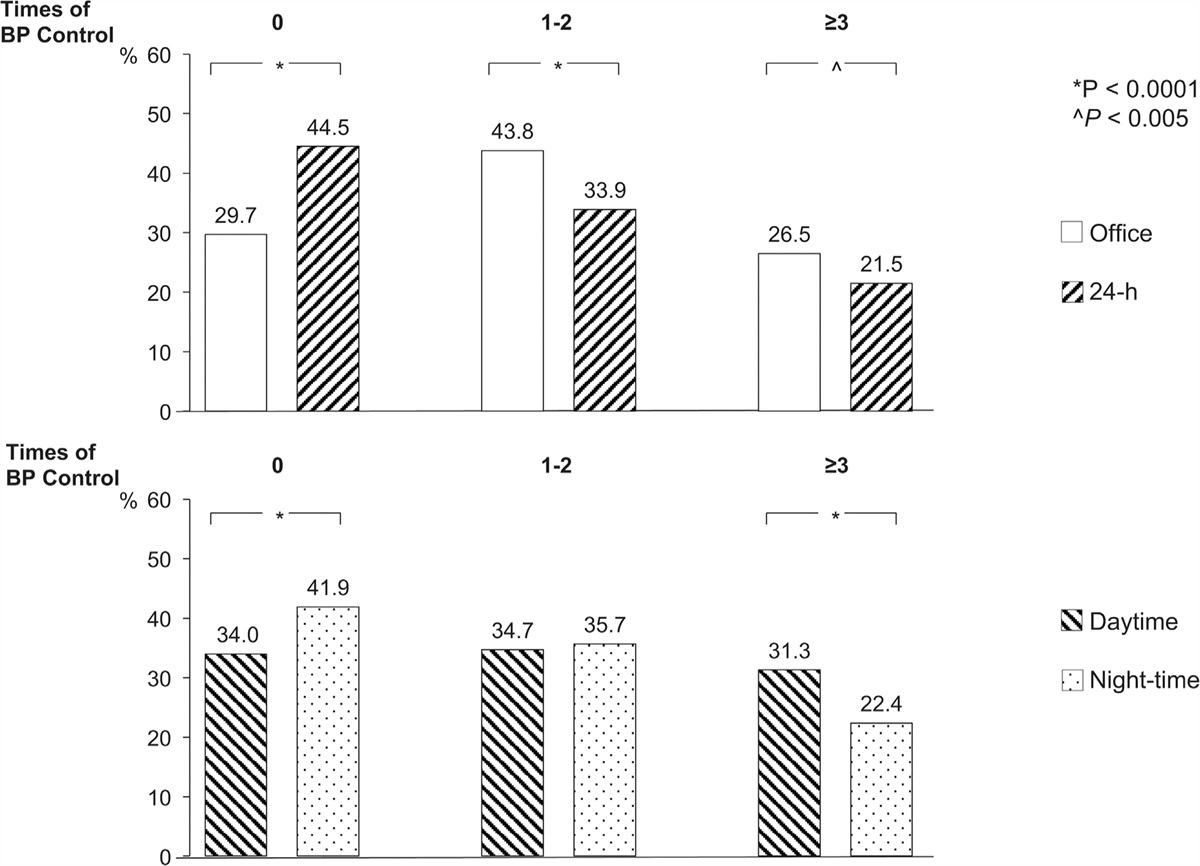
Table 2 lists the ambulatory blood pressure parameters of the study participants. The 24-h urinary sodium was higher in patients who also had higher ambulatory blood pressure (BP) levels (including the 24-h blood pressure, daytime blood pressure, and night-time blood pressure). In terms of circadian rhythm, the night-time systolic blood pressure drop rate was lowest in the high urinary sodium group as compared with the moderate and low urinary sodium groups. The distribution of the dipper, nondipper, and riser groups was different among the different urinary sodium groups, with the riser type share gradually increasing from the low to the medium urinary sodium group to the high urinary sodium group.
TABLE 2 - Indices of ambulatory blood pressure (ABPM) by 24-h urinary sodium in the study population All (n = 398) Low urinary sodium group (n = 58) Moderate urinary sodium group (n = 224) High urinary sodium group (n = 116) P 24-h mean SBP (mmHg) 124.20 ± 15.31 116.39 ± 13.91 123.12 ± 14.76∗ 129.78 ± 15.06 ∗# <0.001 24-h mean DBP (mmHg) 73.35 ± 9.16 66.73 ± 6.87 72.61 ± 8.59∗ 77.78 ± 8.94 ∗# <0.001 Daytime mean SBP (mmHg) 125.46 ± 15.11 119.52 ± 14.31 124.63 ± 14.83∗ 130.09 ± 14.81 ∗# <0.001 Daytime mean DBP (mmHg) 74.64 ± 9.58 68.38 ± 7.54 74.38 ± 9.41∗ 78.42 ± 9.08 ∗# <0.001 Night-time mean SBP (mmHg) 120.10 ± 17.38 112.78 ± 16.03 117.84 ± 16.25 127.64 ± 17.54 ∗# <0.001 Night-time mean DBP (mmHg) 69.83 ± 10.07 62.71 ± 8.77 68.67 ± 9.04∗ 75.24 ± 9.76 ∗# <0.001 24-h SBP load (%) 29.71 ± 28.22 18.24 ± 22.21 27.86 ± 27.86∗ 38.39 ± 29.09 ∗# <0.001 24-h DBP load (%) 22.36 ± 20.66 10.39 ± 10.89 20.42 ± 19.20∗ 31.42 ± 22.95 ∗# <0.001 Daytime SBP load (%) 22.29 ± 26.28 15.12 ± 20.02 21.25 ± 26.46 27.96 ± 27.89 ∗# 0.015 Daytime DBP load (%) 12.40 ± 19.48 3.70 ± 6.77 11.25 ± 18.12∗ 19.08 ± 23.81 ∗# <0.001 Night-time SBP load (%) 47.11 ± 36.82 32.41 ± 35.00 41.41 ± 34.63 64.30 ± 35.69 ∗# <0.001 Night-time DBP load (%) 49.32 ± 34.11 29.22 ± 31.82 44.42 ± 32.67∗ 67.57 ± 29.43 ∗# <0.001 24-h BPV SBP (%) 10.75 ± 2.64 11.01 ± 2.86 10.78 ± 2.53 10.59 ± 2.74 0.685 24-h BPV DBP (%) 13.35 ± 3.78 13.99 ± 4.16 13.69 ± 3.90 12.44 ± 3.22 ∗# 0.022 Daytime BPV SBP (%) 10.15 ± 2.91 10.46 ± 3.13 10.04 ± 2.74 10.18 ± 3.10 0.671 Daytime BPV DBP (%) 13.10 ± 5.88 13.39 ± 4.68 13.37 ± 6.50 12.44 ± 5.22 0.427 Night-time BPV SBP (%) 8.86 ± 3.64 8.92 ± 3.82 9.13 ± 3.71 8.32 ± 3.37 0.241 Night-time BPV DBP (%) 6.72 ± 3.14 7.24 ± 3.78 6.84 ± 3.02 6.26 ± 3.00 0.194 Night-time SBP decline (%) 4.15 ± 7.55 4.22 ± 6.82 5.25 ± 7.16 2.10 ± 8.21# 0.006 Night-time DBP decline (%) 6.30 ± 9.08 7.23 ± 9.93 7.28 ± 9.23 4.07 ± 8.05# 0.021 Dipper patterns 0.027 Dipper pattern (%) 65 (22.3) 6 (14.6) 45 (27.6) 14 (15.9) Nondipper pattern (%) 142 (48.6) 24 (58.6) 79 (48.5) 39 (44.3) Riser pattern (%) 85 (29.1) 11 (26.8) 39 (23.9) 35 (39.8)Values are mean ± SD, or n (%).BPV, blood pressure coefficient of variation; DBP, diastolic blood pressure; SBP, systolic blood pressure.
∗P < 0.05 vs. the low urinary sodium group.
#P < 0.05 vs. the moderate urinary sodium group.∗#P < 0.05 vs. the low and the moderate urinary sodium group.
Table 3 lists the conventional echocardiographic parameters, cardiac magnetic resonance structure, and function parameters of the study participants. No difference was observed between different 24-h urinary sodium groups in terms of E/A and E/e′. In terms of LA structure, it was shown that the maximal left atrial volume (LAV) was significantly increased in the high urinary sodium group when compared to the low and moderate urinary sodium groups(P < 0.001). This study found that concerning LA function, in addition to LA booster function, LA reservoir function and LA conduit function was significantly reduced with an increase in 24-h urinary sodium among participants in various groups (P < 0.01). In addition, the mean LACI was 21 ± 12%, which (LACI) was significantly higher in the high urinary sodium group compared with the low and moderate urinary sodium groups (P < 0.001). As a final point, the EF of all participants was within the normal range, with a mean value of 60.64 ± 7.34%, and the LV function (LV global longitudinal strain, LV global circumferential strain, and LV global radial strain) of participants in the high urinary sodium group was significantly lower than that of participants in the low urinary sodium and moderate urinary sodium groups.
TABLE 3 - Indices of left cardiac structure and function by 24-h urinary sodium in the study population All (n = 398) Low urinary sodium group (n = 58) Moderate urinary sodium group (n = 224) High urinary sodium group (n = 116) P Echocardiographic statistics E/A 0.94 ± 0.32 0.94 ± 0.37 0.95 ± 0.32 0.92 ± 0.28 0.767 E/e’ 8.52 ± 2.58 8.69 ± 2.58 8.25 ± 2.40 8.90 ± 2.86 0.2 CMR statistics LAV (ml) 59.78 ± 25.65 52.82 ± 23.37 55.31 ± 23.47 72.16 ± 26.90 ∗# <0.001 LAs-s (%) 38.76 ± 13.67 45.75 ± 12.15 39.47 ± 13.03∗ 33.61 ± 13.83 ∗# <0.001 LAs-a (%) 17.16 ± 6.25 18.14 ± 4.81 17.63 ± 6.37 15.76 ± 6.56# 0.07 LAs-e (%) 21.44 ± 9.70 27.70 ± 9.39 21.52 ± 9.28∗ 17.89 ± 8.98 ∗# <0.001 LAsr-s (s) 1.75 ± 0.65 2.01 ± 0.68 1.78 ± 0.65∗ 1.56 ± 0.58 ∗# 0.002 LAsr-a (s) 2.22 ± 0.77 2.32 ± 0.60 2.28 ± 0.78 2.04 ± 0.82# 0.074 LAsr-e (s) 2.17 ± 1.03 2.72 ± 1.07 2.24 ± 1.01∗ 1.75 ± 0.89 ∗# <0.001 LV EDV(ml) 134.95 ± 28.33 119.60 ± 21.27 132.10 ± 25.56∗ 148.86 ± 30.95 ∗# <0.001 LVMI (g/m2) 75.83 ± 21.54 71.76 ± 20.26 73.27 ± 17.89 82.98 ± 26.59 ∗# 0.002 EF (%) 60.64 ± 7.34 61.42 ± 7.84 61.45 ± 6.54 58.68 ± 8.17# 0.026 LV GRS (%) 31.65 ± 7.84 34.34 ± 6.92 31.93 ± 7.49 29.60 ± 8.56 ∗# 0.012 LV GCS (%) −18.40 ± 3.16 −19.54 ± 2.50 −18.49 ± 3.12 −17.57 ± 3.38 ∗ 0.009 LV GLS (%) −16.42 ± 3.54 −18.17 ± 1.96 −16.44 ± 3.99∗ −15.39 ± 2.83 ∗# 0.001 LACI (%) 20.86 ± 12.14 18.73 ± 10.10 18.95 ± 9.98 25.92 ± 15.45# <0.001Values are mean ± SD, or n (%).A, the peak late transmitral flow
留言 (0)