
記住我








Multisystem Inflammatory Syndrome in children (MIS-C) is a novel systemic hyperinflammatory, multiorgan disorder temporally associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection described in children and adolescents younger than 21 years of age. The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) have developed criteria for MIS-C.1,2 The CDC criteria for MIS-C include individuals <21 years of age, with laboratory evidence or history of close contact with SARS-CoV-2 infection, fever >24 hours, severe disease requiring hospitalization with at least 2 organ systems involved, laboratory evidence of inflammation, and all other plausible diagnoses to be excluded.1 The exact pathophysiology of MIS-C remains unknown, although it is considered an exaggerated innate and adaptive response of the immune system following SARS-CoV-2 infection in susceptible individuals.3
Since April 2020, reports from Europe, United Kingdom, United States of America and the Western Cape in South Africa reported cases of MIS-C in children with a median age of 9–11 years and mortality rates between 0% and 4%.4–8 However, India, Pakistan, and Colombia have reported MIS-C in younger children (median age 2–7 years) with mortality rates ranging from 9% to 20%.9–12 There are few studies from Africa; these include a study by Butters et al,4 a letter by Webb et al8 from Cape Town, a case series from Sokunbi et al13 from Nigeria and 2 case reports from Moodley P et al14 and Onyeaghala et al.15 In the analysis of 469 children hospitalized in 6 sub-Saharan African countries with SARS-CoV-2 infection, 6.1% were noted to have suspected or confirmed MIS-C.16 While MIS-C was reported in this large multicentre study, the study was limited because of a lack of laboratory and infrastructural capacity to confirm the diagnosis in most countries where the study was performed. Outcomes of children in Sub-Saharan Africa may differ because of the higher burden of childhood diseases like malnutrition, human immunodeficiency virus infection (HIV), tuberculosis (TB) and poorer overall SARS-CoV-2 vaccine coverage.17 MIS-C has also been reported to be more severe in children of Black-African ethnicity living in Europe, the United Kingdom and the Americas and children from a lower socioeconomic background.18,19 Therefore, there is a need to describe the characteristics of MIS-C and the possible associations of severe disease in African children. KwaZulu-Natal is the second-most populous province in South Africa, with the second-highest documented COVID infections, where 86% of the population is Black-African, and 52% of the population live below the poverty line.20,21 Thus, we undertook this study in KwaZulu-Natal.
MATERIALS AND METHODSThis retrospective study was conducted at 5 referral hospitals in KwaZulu-Natal, and records of children hospitalized with MIS-C between June 1, 2020, and April 30, 2021, were analyzed. Cases were identified from the admission register at each hospital by the attending pediatricians, who were co-investigators in this study. Records that met the CDC criteria for MIS-C were included, while records that did not meet the CDC criteria or had an alternative etiologic diagnosis, including those with other microbial causes for the inflammation, were excluded.1 Demographics, clinical data, laboratory tests, imaging, treatment and outcomes were abstracted from the patient’s medical records; this was captured on a case report form and entered into a Microsoft Excel database for Windows [version 16.60 (22041000)]. Medical records which could not be retrieved were excluded. The patient’s race was abstracted from the records as reported by the caregivers. The 5 hospitals enrolled included 2 regional hospitals, 2 tertiary hospitals and 1 central hospital.
These sites were selected as these hospitals have access to laboratory facilities and the capacity to provide critical care to children.
Nutritional disorders were defined using the WHO child growth standards and expressed as z-scores. Weight/length growth charts were used for children under 5 years, and the body mass index (BMI) for children 5 years and older.22 Laboratory tests were analyzed by the National Health Laboratory Service; test results were interpreted according to the National Health Laboratory reference ranges. SARS-CoV-2 RT-PCR was performed on nasopharyngeal swabs of all children. Children who had negative COVID-19 tests but were suspected of having MIS-C were tested for the IgG antibody using the Abbott Architect SARS-CoV-2-IgG (Abbott IL, United States) test for the qualitative detection of SARS-CoV-2 nucleocapsid protein antibodies, to determine exposure to COVID-19. Cardiac involvement was defined as any myocardial, pericardial, endocardial or coronary artery involvement on echocardiography or elevated cardiac biomarkers (troponin-T ≥100 or B-type natriuretic peptide (BNP) ≥1000). Myocardial involvement was defined as fractional shortening ≤28% or ejection fraction less than 50%, or elevated cardiac biomarkers. Coronary artery dilatation was reported if the artery diameter was greater than 2.5 z-scores on echocardiography.23 Shock was identified from the clinical records, supported by evidence of hypotension (systolic arterial pressure less than the fifth percentile for age), capillary refill time >2 seconds or prescription of inotropes. Acute kidney injury (AKI) was defined according to the kidney disease: Initiating Global Outcome (KDIGO) classification.24 Whittaker et al identified 3 patterns of MIS-C in children, a group with severe disease who developed shock and organ involvement, a group with persistent fever and elevated inflammatory markers without features of organ involvement and a third group with features of Kawasaki Disease.5 In this study, children who developed shock, were defined as having “severe disease” and were compared with children who did not develop shock to identify possible associations of severe MIS-C. Morbidity was reported if a child had clinical or biochemical evidence of organ dysfunction on discharge.
Statistical AnalysisBaseline demographic and clinical characteristics were summarized using frequencies, proportions, medians and interquartile ranges. These were applied to categorical and continuous variables. Comparisons were performed using the Pearson Chi-squared test and Fisher exact test for categorical variables, student t-test for normally distributed variables and Mann-Whitney test for data that were not normally distributed. A P value of <0.05 was considered statistically significant. Risk factors associated with death were identified using Chi-square tests or Fisher’s exact test for categorical variables and Mann-Witney tests for numeric variables. Logistic regression was then used to examine the strength of the association and odds ratios (OR) with 95% confidence limits reported. Risk factors potentially associated with shock or mortality were examined. Only the bivariate P values and OR are reported. Because of the small sample size and missing data, a multivariable model was not used to adjust for possible confounders. All analyses were performed using Stata software version 17 (StataCorpLLC). Approval for the study was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (BREC 00002121/2020).
RESULTSThirty-five children were identified with a suspected diagnosis of MIS-C during the 11-month study period, which included the first and second SARS-CoV-2 waves in South Africa. Two children were excluded as a temporal association with SARS-CoV-2 infection could not be established, and 4 had alternative causes for the inflammation. Twenty-nine children were included in the study, 27 (93%) had laboratory evidence of SARS-CoV-2 infection, and 2 had close SARS-CoV-2 contacts. SARS-CoV-2 RT-PCR was positive on 16/29 (55%), and the SARS-CoV-2 antibody was positive on 12/16 (75%). One child tested positive for both the SARS-CoV-2 PCR and the antibody test.
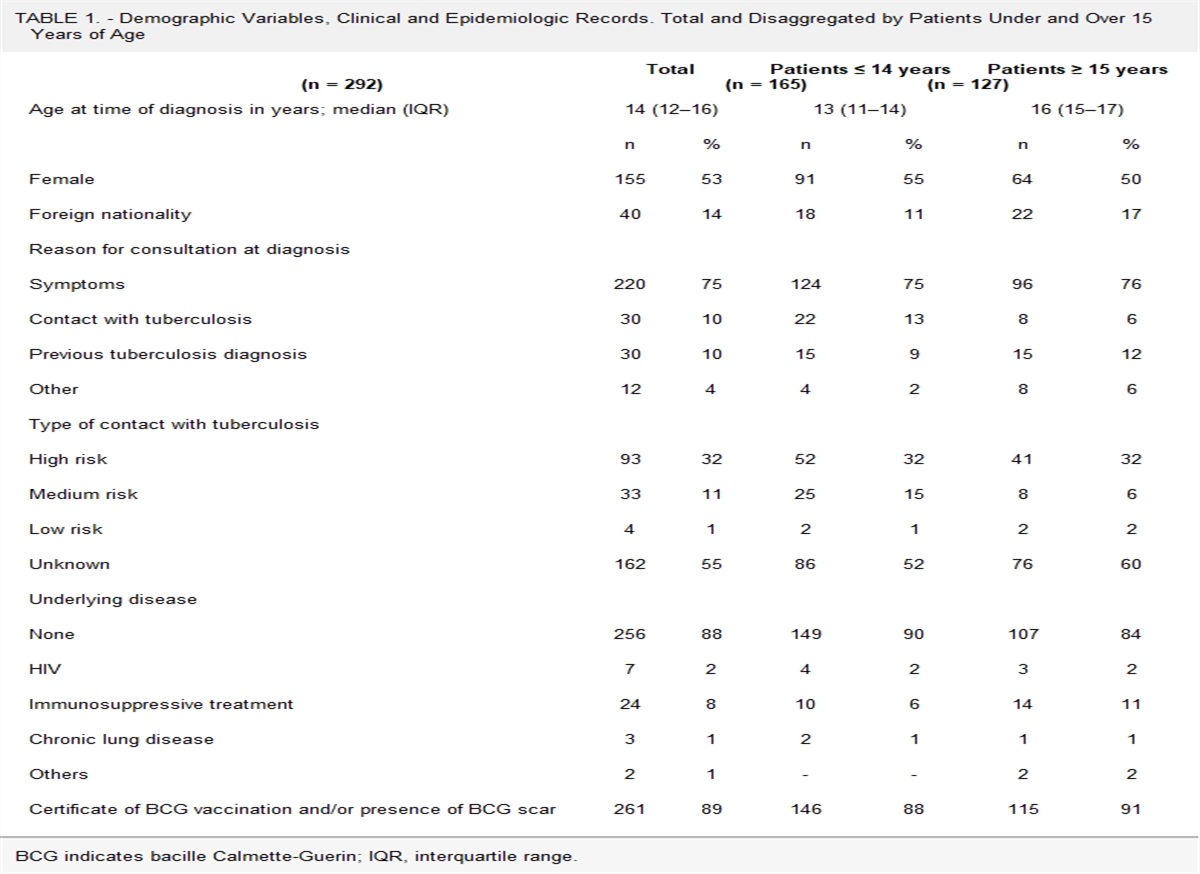
Table 1 describes the demographics and clinical characteristics of the participants. The mean age was 55 (SD ±45) months with 17 (59%) ≤5 years, 13 (45%) males and 25 (86%) Black-African. Pre-existing comorbidities were documented in 8 (28%) children, including congenital heart disease 1 (3%), system onset juvenile idiopathic arthritis 1 (3%), HIV 1 (3%), moderate acute malnutrition 3 (10%) and obesity 2 (7%). The most common presenting symptoms were fever 29 (100%), gastrointestinal symptoms 25 (86%) and rash 19 (65%). The medium duration of fever was 5 IQR (4–7) days. The mucocutaneous lesions included discreet erythematous maculopapular rash over the trunk and limbs, diffuse erythroderma, urticarial lesions with pruritis, peripheral edema of hands and feet, desquamation, perioral erythema, cracking of the lips and bilateral bulbar conjunctival injection. Acute abdominal pain was documented in 17 (59%) children, with 4 (14%) requiring laparotomy.
TABLE 1. - Demographics, Clinical Features and Treatment of Children With Shock Compared With Those Without Shock, With MIS-C in KwaZulu-Natal Total (n = 29) Patients With Shock (n = 17) Patients Without Shock (n = 12) P Odds Ratio (OR) 95% Confidence interval (CI) Age (months), mean (SD) 55 (±45) 66 (±50) 50 (±32) 0.26 1.16 0.96–1.41 Sex Male 13 (45%) 4 (30%) 9 (70%) ref ref ref Female 16 (55%) 13 (81%) 3 (19%) 0.01 9.75 1.74–54.85 Ethnicity African 25 (86%) 15 (60%) 10 (40%) 0.70 1.5 0.18–12.46 Indian 4 (14%) 2 (50%) 2 (50%) ref ref ref Comorbidity 8 (28%) 7 (88%) 1 (12%) 0.05 7.7 0.8–74 Laboratory tests COVID PCR-positive 16 (55%) 10 (63%) 6 (37%) 0.64 1.43 0.32–6.32 SARS-CoV-2 IgG (n = 16) 12 (75%) 8 (67% 4 (33%) 0.15 6.0 0.46–77.7 Clinical features Fever 29 (100%) 17 (59%) 12 (41%) Vomiting 19 (65%) 13 (68%) 6 (32%) 0.15 3.25 0.66–15.98 Abdominal pain 17 (59%) 11 (65%) 6 (35%) 0.43 1.83 0.40–8.27 Diarrhea 15 (52%) 9 (60%) 6 (40%) 0.88 1.13 0.26–4.94 Skin Rash 19 (65%) 12 (63%) 7 (37%) 0.50 1.71 0.36–8.08 Conjunctival Injection 14 (48%) 9 (64%) 5 (36%) 0.55 1.58 0.35–7.00 Mucositis 16 (55%) 9 (56%) 7 (43%) 0.77 0.80 0.18–3.57 Cardiac involvement 15 (52%) 12 (80%) 3 (20%) 0.02 7.20 1.35–38.33 Respiratory distress 12 (41%) 9 (75%) 3 (25%) 0.14 3.38 0.67–17.00 Acute kidney injury 12 (41%) 11 (92%) 1 (8%) 0.01 20.17 2.07–196.4 ALOC 10 (34%) 9 (90%) 1 (10%) 0.03 11.37 1.17–590.4 Treatment Corticosteroids* 21 (72%) 15 (71%) 6 (29%) 0.04 7.5 1.2–48.1 IVIG† 21 (72%) 14 (66%) 7 (33%) 0.22 3.33 0.61–18.1 Inotropic drugs 15 (52%) 15 (100%) 0 (0%) <0.001 76.83 9.41–inf ICU Admission 11 (38%) 10 (91%) 1 (9%) 0.01 14.25 1.47–742.2 Mechanical Ventilation 10 (34%) 9 (90%) 1 (10%) 0.03 11.37 1.17–590.4*Corticosteroids: IV methylprednisone 10 mg/kg/day × 3 days (taper) or IV dexamethasone: 0.5 mg/kg/d × 5–10 days.
†IVIG-IV: immumonoglobulin 2 g/kg over 48 hours.
The laboratory findings are described in Table 2. Children who presented in shock had significantly higher CRP (211 vs. 106 mg/L; P = 0.01), ferritin (1447 vs. 204 ng/mL; P < 0.001), D-dimers (8.5 vs. 1.8 mg/L; P = 0,01), BNP (2500 vs. 163 ng/L; P = 0,01), troponin-T (110 vs. 40 ng/mL; P = 0.02) and lower mean platelet levels (89 vs. 277 × 109/L; P = 0.02) and albumin (23 vs. 33 g/L; P = 0.001) compared with those without shock. Significantly more cardiac involvement (OR 7.2; confidence interval [CI] 1.35–38.33); P = 0.02; acute kidney injury (AKI; OR 20.17; CI 2.07–196.4); P = 0.01 and altered level of consciousness (OR 11:37; CI 1.17–590.4); P = 0.03 was observed in children with shock. Echocardiography was performed after the first week of admission in 20 of 29 (69%) of children by a Pediatric Cardiologist. Myocardial involvement was documented in 13 of 26 (50%), pericardial effusion 2 of 20 (10%) and no coronary artery dilatations or aneurysms were detected. The extent of multisystem involvement is reflected in 24 (83%) children having ≥4 organ-systems involved and 18 (62%) having ≥6 organ-systems involved.
TABLE 2. - Laboratory Features of Children With Shock Compared With Those Without Shock, With MIS-C in KwaZulu-Natal Total (n = 29) Patients With Shock (n = 17) Patients Without Shock (n=12) P NHLS (Normal Range) Leucocyte count (×109/L)*† 12 (9.1–21.3) 14.5 (9.2–2) 11.4 (8.1–17.7) 0.39 3.9–10.2 Lymphocyte (×109/L)*† 1.4 (1.1–2.1) 1.4 (1–1.9) 1.5 (1.3–2.5) 0.28 1.90–4.30 Platelet (×109/L)*† 133 (78–312) 89 (76–159) 277 (151–459) 0.01 150–440 C-reactive protein (mg/L)*† 181 (106–233) 211 (167–246) 106.5 (74–164.5) 0.01 <10 Ferritin (ng/mL)*† (n = 27) 631 (226–1593) 1447 (860–1650 204 (94.5–470 <0.001 7–84 D-dimer (mg/L)*† (n = 28) 3.9 (1.2–12.2) 8.6 (2.4–14.1) 1.8 (0.2–3.5) 0.01 0.00–0.25 BNP (ng/L)*† (n = 26) 935 (152–4579) 2500 (746–4944) 163.5 (78–590) 0.01 <100 Troponin (ng/mL)*† (n = 25) 74 (40–124) 110 (60–435) 40 (20–84) 0.02 ≤50 Albumin (g/L)*† 24 (22–33) 23 (20–24) 33.5 (31–43.5) <0.001 32–47 ALT(U/L)*† 62 (30–109) 64 (48–122) 40 (11.5–103) 0.18 5–30 Creatinine (umol/L)*† 59 (25–123) 87 (59–149) 24.5 (20.5–38.5) <0.001 40–72 Sodium mmol/L*† 135 (131–138) 134 (128–138) 138 (133–138) 0.29 136–145*IQR.
#Median.
ALT indicates alanine transaminase; BNP, B-type natriuretic peptide; IQR, interquartile range; NHLS, National Health Laboratory Service.
The treatment is described in Table 1. Nine children (34%) required invasive ventilation, 1 child did not have access to invasive ventilation and inotropic drugs were prescribed in 15 (52%). Twenty-three children (79%) received specific treatment for MIS-C; 21 (72%) received intravenous immunoglobulin (IVIG) 2 g/kg over 48 hours, 6 (21%) received a second dose of IVIG, 21 (72%) received corticosteroids and 19 (66%) received both IVIG and steroids. Of the children who received corticosteroids, 14 (67%) received intravenous methylprednisolone at 10 mg/kg for 3–5 days with tapering and 7 (33%) received intravenous dexamethasone at 0.5 mg/kg/day × 7–10 days. Aspirin was prescribed in 9 (31%), while 4 (14%) received low molecular weight heparin. All children received antibiotics, none of the admission microbial cultures were positive, and 2 children developed ICU-acquired nosocomial sepsis. Children who developed shock required significantly more corticosteroids (OR 7.5; CI 1.2–48.1; P < 0.04), inotropic drugs (OR 76.83; CI 9.41–inf; P < 0.001), intensive care unit (ICU) admission (OR 14.25; CI 1.47–742.2; P < 0.01) and invasive ventilation (OR 11.37; CI 1.17–590.4; P < 0.03) compared with those without shock. According to the American Heart Association criteria, 7 children were classified as having incomplete Kawasaki disease (KD).25 The mean age was 84 (SD ±40) months, and all had fever and mucocutaneous signs. Shock was documented in 5 (71%), myocardial injury 4 (57%), AKI 4 (57%), thrombocytopenia 5 (71%) and 6 (86%) required corticosteroids. None had evidence of coronary artery aneurysms on late echocardiography.
The median length of hospital stay was 11 (IQR 7–19) days. A full recovery was documented in 14 (48%) of children at discharge, and 4 (14%) recovered within 8 weeks of discharge; these children had discharge diagnoses of intermittent fevers 2 (7%), mild myocardial dysfunction 1 (3.5%), and a small pericardial effusion 1 (3.5%). Residual morbidity was documented in 5 (17%) children; spastic quadriplegia 1 (3.5%), speech and cognitive deficits 1 (3.5%), amputation of the foot 1 (3.5%), cardiomyopathy 1 (3.5%) and relapse of the systemic onset of juvenile idiopathic arthritis 1 (3.5%). The CT angiography of the child with spastic quadriplegia demonstrated multiple areas of stenosis in the anterior cerebral artery and the angiogram of the child with gangrene demonstrated arterial occlusion of the vessels of the foot. The mortality was 20.6%, and the mean age of children who did not survive was 48.3 (SD:65,3). In the mortality analysis, we found that children who did not survive had significantly higher ferritin levels 1593 (IQR 1069–1650) ng/mL versus 540 (IQR 181–1156) ng/mL; P = 0.03) and significantly more of them required mechanical ventilation (P < 0.005; OR = 18; CI:1.7–191.5) compared with those who survived. There were no significant differences between the survivors and the nonsurvivors with regard to age, sex, inflammatory markers, cardiac biomarkers or organ involvement. Four of the 6 (66%) children who did not survive met the 2016 Pediatric Rheumatology International Trials Organization criteria for macrophage activating syndrome,26 compared with 4 of 23 (17%) of those who survived. Because of resource constraints, biologics and extracorporeal membrane oxygenation therapy were not available.
DISCUSSIONThis study reports on 29 children hospitalized with MIS-C in KwaZulu-Natal, South Africa. It is the first study that highlights the significant mortality and morbidity associated with MIS-C in a poorly resourced African setting with high rates of HIV, Tuberculosis and malnutrition. The 5 hospitals selected are referral hospitals; thus, there may be an overrepresentation of children with severe MIS-C. In contrast to studies from high-income countries,5–7 we found that these children tended to be younger, had more aggressive disease and had higher mortality. We found that 59% of children were ≤5 years of age compared with 42% in the group of children under 13 years reported by Dufort et al from the United States.7 A younger age for MIS-C was also reported in other low-middle-income countries, including India, Pakistan and Colombia.10–12 In addition, we found that previously unidentified comorbidities like HIV and malnutrition, although limited by small numbers, may contribute to the higher morbidity and mortality in this setting.27,28 This study adds to the evidence that significantly elevated biomarkers and critical organ involvement may be associated with severe MIS-C, and it suggests that higher ferritin levels and the need for mechanical ventilation confers a higher mortality risk in this context.
The predominant presentation of MIS-C in the current study was that of a febrile illness with gastrointestinal and mucocutaneous symptoms associated with shock and multisystem disease. We found that significantly increased CRP, ferritin, BNP, troponin, creatinine, low platelets and albumin were associated with severe MIS-C. These biomarkers have crucial clinical utility in identifying, managing, and monitoring children with high risk for severe MIS-C, especially in Sub-Saharan Africa, where access to higher levels of care is very limited.
Critical organ involvement was more common in our series, with altered levels of consciousness (34% vs. 9%) and AKI (41% vs. 22%) compared with the United Kingdom.5 A third of the children presented with an altered level of consciousness, highlighting the delay in presentation of MIS-C in our setting. Lipton et al observed significantly elevated inflammatory markers in 26 children with MIS-C who had AKI, suggesting that AKI is also a marker of severe disease.29 Coronary artery dilatations and aneurysms have been described on early echocardiography in children with MIS-C, which resolved on subsequent imaging.5,6,30 The absence of coronary artery dilatations and aneurysms may be explained by the delayed echocardiography performed in our setting because of resource constraints. A quarter of our participants presented with the KD phenotype; however, they were older, had severe circulatory, cardiac, renal and coagulation abnormalities and required more corticosteroids, which differs from the classic KD. This supports the evidence that MIS-C is distinct from KD and may represent a new systemic inflammatory disease.25
Consensus has not been reached regarding the treatment of MIS-C, and the optimal use of IVIG and corticosteroids remains controversial.31,32 The treatment of MIS-C was not standardized however most children received IVIG as the first line of therapy; corticosteroids were added if there was a poor response to IVIG or if the child had shock or organ involvement. Most children received both IVIG and corticosteroids. The cost of IVIG may be prohibitive in resource-limited countries, and the large volumes of fluids required to reconstitute IVIG may exacerbate myocardial dysfunction. Licciardi et al documented a 67.7% response in 31 children treated with IV methylprednisolone alone as the first line of treatment, suggesting that steroids could be used as first-line therapy.33 However, a larger randomized study is required to verify this. When compared with the series by Butters et al from Cape Town, we observed lower platelet count (133 vs. 189 × 109/L), higher troponin levels (74 vs. 38 ng/mL), greater use of inotropes (52% vs. 38%) and more invasive ventilation (34% vs. 11.8%), suggesting a more aggressive inflammatory process in our cohort. This may possibly be because of a delay in accessing healthcare and the limited access to higher levels of care and advanced therapies in our study. The lower rates of ICU admissions (38% vs. 80%) compared with the cohort from the United States reflect the limited availability of ICU facilities. There is a critical shortage of intensive care beds for children in KwaZulu-Natal, with ICUs only available at the central hospital and one of the tertiary hospitals enrolled. A limited number of patients are offered “interim ventilation” at regional hospitals until an ICU bed is available at the central hospital. The central hospital is the only public hospital in the province to provide renal replacement therapy and perform echocardiography by Pediatric Cardiologists to a population of 10 million, reflecting resource constraints in this population.
The 20% mortality in this series is higher than that reported in the literature, which ranges from 0% to 4% in high-income countries to 9% to 20% in LMIC. We found that the higher ferritin levels conferred a higher risk for mortality which is consistent with the report from Colombia. Two-thirds of children who did not survive had evidence of macrophage activating syndrome,26 reflecting the aggressive inflammation associated with MIS-C in our patients. The increased mortality in this study may be attributed to severe inflammation associated with delayed presentation, delay in accessing higher levels of care and poor access to advance therapies because of resource constraints or a more aggressive inflammatory process in the African patient. KwaZulu-Natal is a province with high poverty levels (52.4% vs. 21.3%) compared with the Western Cape. According to a Statistics South Africa 2018 general household survey, 62% of the child population of KwaZulu-Natal is classified as rural, while 94% of the children in the Western Cape were classified as urban dwellers.18 Rural areas in South Africa have limited access to health care facilities, primarily regional and tertiary levels of health care. Javalkar et al also reported that lower socioeconomic status and Black-African ethnicity were independent risk factors for MIS-C.34 About half of the population in KwaZulu-Natal live below the poverty line in poor socioeconomic circumstances.18 In a retrospective surveillance study in the United States, Abrams et al found that non-Hispanic Black children were more likely to require mechanical ventilation and have more severe outcomes than White children.15 Broad et al reported similar findings in the United Kingdom.16 A larger prospective study with genetic and immunopathological investigations is required to explore these factors in our setting.
CONCLUSIONMIS-C, in a resource-constrained setting, is an aggressive disease with substantial mortality. Significantly elevated biomarkers and critical organ involvement are associated with severe MIS-C. This study highlights the need for rapid recognition and treatment of MIS-C. It underscores the premise that social determinants of health possibly contribute to poorer outcomes in more impoverished communities.
Limitations of the StudyA major limitation is that this is a small study and is underpowered to detect statistically significant differences between groups. Children under the age of 13 years were enrolled from referral facilities, therefore, there is a bias toward younger children and severe diseases. The study also reports on children from areas with limited health resources and poor socioeconomic backgrounds, with both these factors impacting clinical presentation and outcomes.
ACKNOWLEDGMENTSWe express gratitude to Ms Cathy Connolly (Biostatistician), School of Public Health, University of KwaZulu-Natal) and Mrs Leora Sewnarain for assistance with formatting and language review.
REFERENCES 1. Centers for Disease Control and Prevention (CDC). Multi-system inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19). 2020. Available at: https://emergency.cdc.gov/han/2020/han00432.asp. Accessed May 10, 2022. 2. World Health Organization (WHO). Multi-system inflammatory syndrome in children and adolescents temporally related to COVID-19. 2020. Available at: https://www.who.int/publications-detail-redirect/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19. Accessed May 10, 2022. 3. Henderson LA, Yeung RSM. MIS-C: early lessons from immune profiling. Nat Rev Rheumatol. 2021;17:75–76. 4. Butters C, Abraham DR, Stander R, et al. The clinical features and estimated incidence of MIS-C in Cape Town, South Africa. BMC Pediatr. 2022;22:241. 5. Whittaker E, Bamford A, Kenny J, et al.; PIMS-TS Study Group and EUCLIDS and PERFORM Consortia. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA. 2020;324:259–269. 6. Feldstein LR, Rose EB, Horwitz SM, et al. Overcoming COVID-19 investigators; CDC COVID-19 response team. multisystem inflammatory syndrome in U.S. children and adolescents. N Engl J Med. 2020;383:334–346. 7. Dufort EM, Koumans EH, Chow EJ, et al. Multisystem inflammatory syndrome in children in New York State. N Engl J Med. 2020;383:347–358. 8. Webb K, Abraham DR, Faleye A, et al.; Cape Town MISC-Team. Multi-system inflammatory syndrome in children in South Africa. Lancet Child Adolesc Health. 2020;4:e38. 9. Nayak S, Panda PC, Biswal B, et al.; EICOMISC Study Group. Eastern India Collaboration on Multisystem Inflammatory Syndrome in Children (EICOMISC): a multicenter observational study of 134 cases. Front Pediatr. 2022;10:834039. 10. Dhanalakshmi K, Venkataraman A, Balasubramanian S, et al. Epidemiological and clinical profile of pediatric inflammatory multisystem syndrome - temporally associated with SARS-CoV-2 (PIMS-TS) in Indian children. Indian Pediatr. 2020;57:1010–1014. 11. Mohsin SS, Abbas Q, Chowdhary D, et al. Multisystem inflammatory syndrome (MIS-C) in Pakistani children: a description of the phenotypes and comparison with historical cohorts of children with Kawasaki disease and myocarditis. PLoS One. 2021;16:e0253625. 12. Acevedo L, Piñeres-Olave BE, Niño-Serna LF, et al. Mortality and clinical characteristics of multi-system inflammatory syndrome in children (MIS-C) associated with covid-19 in critically ill patients: an observational multicenter study (MISCO study). BMC Pediatr. 2021;21:516. 13. Sokunbi O, Akinbolagbe Y, Akintan P, et al. Clinical presentation and short-term outcomes of multisystemic inflammatory syndrome in children in Lagos, Nigeria during the COVID-19 pandemic: a case series. EClinicalMedicine. 2022;49:101475. 14. Moodley P, Tsitsi JML, Reddy DL, et al. A case of multi-system inflammatory syndrome in an African adolescent male: case report. Pan Afr Med J. 2021;38:174. 15. Onyeaghala C, Alasia D, Eyaru O, et al. Multisystem inflammatory syndrome (MIS-C) in an adolescent Nigerian girl with COVID-19: a call for vigilance in Africa. Int J Infect Dis. 2021;105:124–129. 16. Nachega JB, Sam-Agudu NA, Machekano RN, et al.; African Forum for Research and Education in Health (AFREhealth) COVID-19 Research Collaboration on Children and Adolescents. Assessment of clinical outcomes among children and adolescents hospitalised with COVID-19 in 6 sub-Saharan African countries. JAMA Pediatr. 2022;176:e216436.
留言 (0)