
記住我






ANDA data has shown room for improvement in key processes and clinical outcomes over the previous 8 years; hence, there is an urgent need for reformatting the feedback. Our formative work with ANDA centres identified desired changes to data presentation in ANDA feedback. The comparator will hence be ANDA feedback only, but this feedback will be redesigned to meet these identified needs.
Intervention description Interventions Feedback reportBoth the intervention and control groups will receive the redesigned ANDA feedback report. This feedback report will be informed by the formative qualitative study [16] and developed by the lead author in consultation with the investigator group, including clinicians and an audit and feedback expert. The draft design of the report will then be modified based on their advice about clarity and feasibility, in a co-design process. The redesigned feedback will be configured for an automatic generation process by the ANDA data management team and will be delivered electronically to the contact person for each participating diabetes centre as a PDF document at one timepoint (December 2021).
PowerPoint slide deckA partially pre-populated PowerPoint slide deck template to facilitate presentation of data within clinical practice teams will also be provided with the feedback report. The slide deck will be developed by the project lead in consultation with the ANDA-EFFECT investigator group and will allow diabetes centres to enter the data from their ANDA feedback report into the PowerPoint template.
Control armStandard treatment/care: Participating diabetes centres randomised to the control arm will only receive the feedback report and PowerPoint slide deck, as above.
Intervention armIn addition to the feedback report and PowerPoint slide deck, participating diabetes centres randomised to the intervention arm will receive a tailored theory-based intervention designed to address identified, modifiable barriers to utilising and implementing the recommendations from ANDA feedback. The design of the intervention is underpinned by a formal qualitative study to elicit current quality improvement practices and barriers to implementation of feedback [16].
Intervention componentsThe intervention comprises a package of educational resources and community of practice forums, delivered on the NADC website. These resources will include:
A 45-min QI webinar will be developed to guide participants, including short instructional videos to guide participants through understanding their data, along with presentations delivered by external QI experts
Audio-visual stories from clinical change champions from a range of metropolitan and regional services in different states in Australia, identified through prior NADC involvement. These stories will describe how change champions have used ANDA data to facilitate QI activities
Peer-led community of practice forums will be provided on the NADC website to facilitate participants to share knowledge and ideas related to the effective use of ANDA data. These forums will be moderated by the project lead
These resources will be produced by the project lead and the investigator group in collaboration with the NADC to maximise their clinical outreach. To prevent contamination between study groups, the intervention resources will be password-protected to only be available to intervention sites.
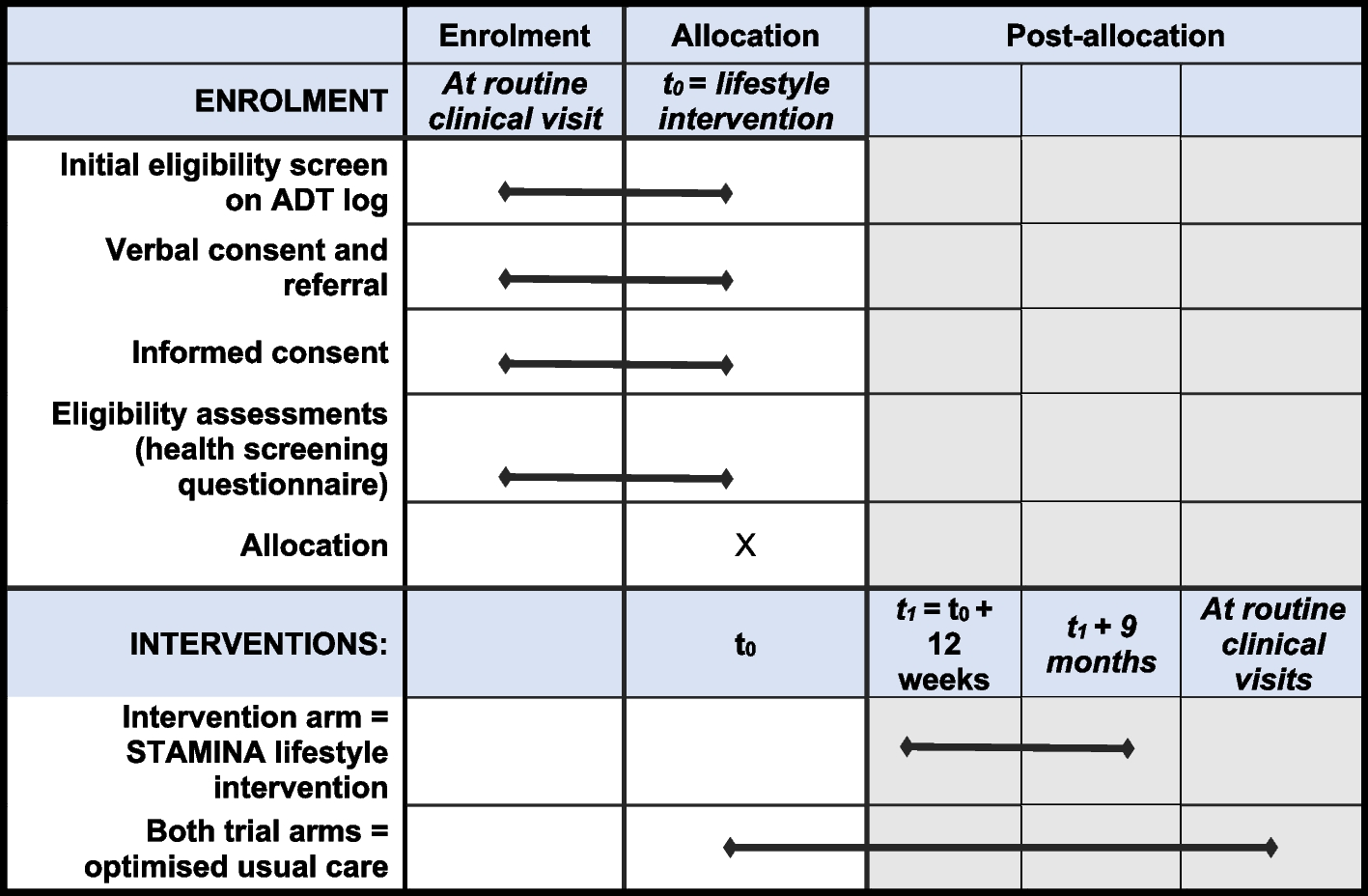
DeliveryThe intervention resources will be made available to participants in the intervention arm by the ANDA research team approximately 3 months before they receive their redesigned ANDA audit feedback, to allow time for familiarisation with the resources. These resources will remain accessible to participants in the intervention arm following the delivery of ANDA audit feedback. There are no a priori plans for centre-specific tailoring or modification of the intervention resources. An overview of the trial arms is shown in Fig. 1.
Fig. 1
Overview of ANDA-EFFECT trial arms
Expectation of engagementThe expectation of participating centres will be made clear in the explanatory recruitment statement. Centres participating in the intervention arm will be expected to complete a minimum of three activities from the intervention resources, including:
Attendance at the QI webinar—this will be hosted initially in the evening, followed by a live question and answer session. The webinar will be replayed with a live question and answer session during a lunch hour, to facilitate maximum uptake
Viewing of at least one ‘clinical change champion’ video
Participation in at least one peer-led forum
We anticipate that these activities will take up to 80 min in total, which could be comprised of multiple 5–10-min viewing blocks.
Criteria for discontinuing or modifying allocated interventionsThere are no criteria for discontinuing or modifying the allocated interventions, as the interventions are delivered to participating diabetes centres, not individual patients.
Strategies to improve adherence to interventionsThe trial will be promoted by the clinical partners (NADC) to their members who have participated in ANDA in 2021. A potential limitation of the recruitment strategy is that this is a pragmatic trial utilising an existing audit and feedback activity, where participation in ANDA 2021 has been impacted by the effects of COVID-19 on clinical practice [18]. As such, there is a lower than usual number of eligible diabetes centres from which to recruit, and the ANDA-EFFECT investigator group acknowledge that it may be difficult to reach optimal sample size; however, all efforts will be made to maximise participation.
Intervention fidelityThe interventions will be delivered in a standard, pre-recorded manner to all participants and as such are not susceptible to fidelity delivery variability in the way that educational interventions delivered as live sessions can be [19]. Our fidelity evaluation will therefore focus on whether participants engage with the interventions, as detailed in the section ‘Methods in analysis to handle protocol non-adherence and any statistical methods to handle missing data ’.
Relevant concomitant care permitted or prohibited during the trialThis is a cluster randomised trial targeting clinical practices, not patients. As such, there are no restrictions on concomitant care.
Provisions for post-trial careNot applicable as this trial is testing interventions aimed at the cluster (practice) level rather than the patient level. As such, patient care is independent of the trial and will be administered as per normal processes by participating diabetes centres.
Outcomes , including plans for assessment and collection of outcomes Primary outcomesTo address the aim of the trial to assess the impact of the interventions on clinical outcomes, we will collect data on HbA1c levels of patients attending participating centres for care. To address the aim of the trial regarding practitioner perceptions, we will collect data related to the acceptability and utility of the interventions.
HbA1c at 6 monthsHbA1c is routinely collected for patients from participating diabetes centres as part of ANDA. Baseline de-identified (coded) mean HbA1c percentage will be extracted for each participating diabetes centre from routine ANDA data collection in 2021. Follow-up data will be collected as part of the ANDA 2022 audit (6 months after delivery of the 2021 ANDA site reports).
Acceptability and utility of the intervention at 3 monthsTo assess how well the interventions address the issues raised in our formative work [16] at a practitioner level, the acceptability and utility of the intervention will be assessed via a 15-min online survey, which we will design specifically for this purpose. This survey will adapt on a survey (ENACT) used by a group of audit and feedback researchers with permission from the authors (personal communication) to assess the acceptability of online audit and feedback interventions [20]. The ENACT survey will be adapted to allow inclusion of parts of an existing ANDA questionnaire. Surveys will be completed 3 months after the delivery of site reports (feedback). Participants will rate a variety of factors about the feedback using Likert scales and open-ended text comments. The developed, combined survey will be validated for test/retest reliability and face validity prior to its use in outcome assessment (see sub-study below). The survey will be delivered to participants as an email link sent to the registered contact persons for the participating sites and will be conducted through REDCap [21], a secure web application for online survey and database management hosted at Monash University. The survey will be delivered 3 months after the delivery of the ANDA feedback reports.
Secondary outcomes Other clinical and process of care outcomesOther de-identified (coded) baseline clinical and process of care outcomes will be extracted from routine ANDA data collection in 2021, using the ANDA data collection form. These will include mean systolic blood pressure (mm Hg) and associated prescribing rates of hypertensives as well as mean total cholesterol, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) (mmol/L) and the associated prescribing rates of lipid-lowering medications. In the same manner as the primary clinical outcome, follow-up data will be collected as part of the ANDA 2022 audit (6 months after the delivery of the 2021 ANDA site reports). All clinical measures included in the standard ANDA data collection form are collected independently of this trial, either by the participating diabetes centres or by the independent pathology services undertaking clinical testing for the participating centres as part of their routine care. As these results are submitted to ANDA in a coded (de-identified) manner, managed by the ANDA data management team and reported in aggregate, the ANDA-EFFECT investigator group do not have access to individual patient data for these variables and will extract mean clinical outcomes from the existing ANDA data set.
Exploratory outcomesHbA1c at 18 months after delivery of intervention may be collected from the ANDA 2023 audit.
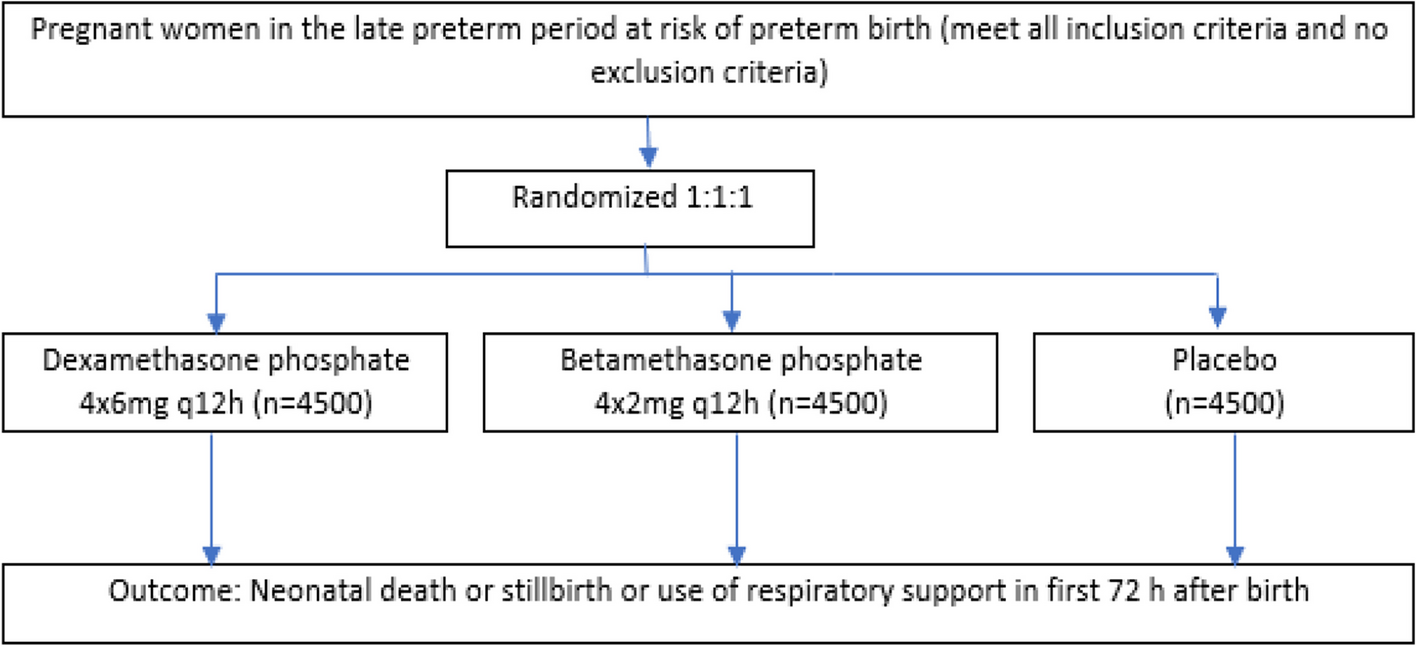
Participant timelineThe participant timeline is presented in Fig. 2.
Fig. 2
ANDA-EFFECT SPIRIT figure [22]
Sample sizeSample size calculation is based on a cluster randomised trial design with the difference in HbA1c as the primary endpoint. Assuming a mean difference in the intervention group of 0.5%, a total sample size of 3500 patients, 35 sites in each arm will provide at least 80% power assuming that the standard deviation of HbA1c is 2.3, the intracluster correlation coefficient is 0.070 and the coefficient of variation of cluster sizes is 0.730. We thus plan to recruit 78 diabetes centres: 39 in each arm to allow for a 10% non-response rate. Sample size calculation was based on the difference in means calculation with the level of significance set at 0.05. PASS V14 software [23] was used for the sample size calculation.
留言 (0)