




記住我
Conceptualization: C.T.C. and M.-A.J.; Participant recruitment and data acquisition: F.B., C.V., L.D.B., N.P., B.L., M.K., M.-J.B., J.C., J.S. (Jason Szabo) J.-P.R., R.T. and E.H.; Methodology, C.T.C., M.-A.J., J.N., J.S. (Joel Singer), T.L., S.M., E.M. and A.V.; Software: J.N., J.S. (Joel Singer) and T.L.; Validation: J.N., J.S. (Joel Singer) and T.L.; Formal Analysis, R.-S.M.B., M.-A.J., C.T.C., J.S. (Joel Singer) and T.L.; Investigation: C.T.C., G.S., M.K., L.D.B., N.P. and M.K.; Resources: C.T.C., M.-A.J., J.N. and D.N.; Data Curation: R.-S.M.B. and C.T.C.; Writing—Original Draft Preparation, R.-S.M.B. and C.T.C.; Writing—Review and Editing, all authors; Supervision, C.T.C., M.-A.J., J.N. and S.S.; Project Administration, C.T.C., J.N., D.N. and M.-A.J.; Funding Acquisition, C.T.C. and M.-A.J.; Manuscript approval: all authors. All authors have read and agreed to the published version of the manuscript.
AcknowledgmentsWe thank the participants for their participation in this study. We also thank the staff at the CTN, including Nisha Shewaramani and Elisa Lau (database managers), and Jayamarx Jayaraman (study monitoring) and all CVIS/MUHC research and clinical staff, including Hansi Peiris, Carolina Berini, Sebastien Landry, Benoit Lemire, Jasmine Mian, Kathleen Normandin, Claude Cyr, Yulia Alexandrova, Erik Pavey and Tara Mabanga. We are grateful to the Tilray staff, including Philippe Lucas, Catherine Jacobson and Gosia Grzyb, as well as to Carolyn Baglole and the Research Centre for Cannabis at McGill University.
Figure 1. Schedule of visits and procedures. Screening: Up to 4 weeks prior to randomization, during the screening visit, study staff explained the study to the participants and obtained written informed consent prior to initiating any study procedures. Study staff assessed the participant’s eligibility by assessing the inclusion and exclusion criteria. Study staff collected the medical history and concomitant medications of the study participants and they underwent a complete physical exam. Blood was collected for hematology, blood chemistry, HIV RNA load and CD4 and CD8 T cells counts. A urine pregnancy test was performed for female participants. Cannabis Use Disorder Identification Test-Revised (CUDIT-R), Drug Use Disorder Identification Test (DUDIT) and Alcohol Use Disorder Identification Test (AUDIT) questionnaires were administrated to the participants and they underwent testing for Hepatitis B and C and syphilis infections. They also underwent urine screen for cannabinoids use. Baseline 1: Up to 3 weeks before the randomization, study staff confirmed eligibility of the candidate and reviewed their medical history. Participants then underwent a second cannabinoids screening test, if his/her initial screen was positive, and answered the CUDIT-R questionnaire in order to identify any problematic cannabis use. The participants underwent a targeted physical exam and blood and semen (from male) were collected to quantify the HIV reservoir size in circulating PBMC from blood and in the semen. Nasal swab and stool specimens were collected from study participants. Antiretroviral Therapy (ART) compliance, alcohol intake and concomitant medication were reviewed by the study staff. Baseline 2 (week 0: Initiation of treatment): Participants confirmed their willingness to participate in the study and eligibility was confirmed, before participants were randomized to either arm 1 or arm 2. Blood was collected from participants. Participants underwent a targeted physical exam. Participants also completed the World Health Organization Quality of Life—HIV Brief Scale (WHOQOLHIV-BREF), Euro-Qol-5Dimension (EQ-5D) questionnaire, and Profile of MoodStates (POMS) questionnaires before receiving a one week supply of the study medication. Follow-up visits (visit 3–8; week 1 to 10): During the follow-up visits, participants underwent a physical examination, and blood was collected to assess the biological study measures. Study drug and ART compliance was assessed. Adverse effects (AEs) were recorded. Pregnancy test was performed on urine of female participants. The participants completed the WHOQOLHIV-BREF, EQ-5D, and POMS questionnaires (Visit 6) and received the study medication until their next visit. End of the treatment (Visit 9; week 12): At Visit 9, participants underwent a physical examination, and blood was collected to assess the biological study measures. Nasal swab and stool specimens were collected from all study participants and semen was collected from male participants. AEs were recorded. A pregnancy test was performed on urine of female participants. Participants then completed the WHOQOLHIV-BREF, EQ-5D, and POMS questionnaires. Final study visit (Visit 10; week 14): At the final visit, participants underwent a physical examination, and blood was collected to assess the biological study measures. AEs were recorded and ART compliance was assessed. A pregnancy test was performed on urine of female participants.
Figure 1. Schedule of visits and procedures. Screening: Up to 4 weeks prior to randomization, during the screening visit, study staff explained the study to the participants and obtained written informed consent prior to initiating any study procedures. Study staff assessed the participant’s eligibility by assessing the inclusion and exclusion criteria. Study staff collected the medical history and concomitant medications of the study participants and they underwent a complete physical exam. Blood was collected for hematology, blood chemistry, HIV RNA load and CD4 and CD8 T cells counts. A urine pregnancy test was performed for female participants. Cannabis Use Disorder Identification Test-Revised (CUDIT-R), Drug Use Disorder Identification Test (DUDIT) and Alcohol Use Disorder Identification Test (AUDIT) questionnaires were administrated to the participants and they underwent testing for Hepatitis B and C and syphilis infections. They also underwent urine screen for cannabinoids use. Baseline 1: Up to 3 weeks before the randomization, study staff confirmed eligibility of the candidate and reviewed their medical history. Participants then underwent a second cannabinoids screening test, if his/her initial screen was positive, and answered the CUDIT-R questionnaire in order to identify any problematic cannabis use. The participants underwent a targeted physical exam and blood and semen (from male) were collected to quantify the HIV reservoir size in circulating PBMC from blood and in the semen. Nasal swab and stool specimens were collected from study participants. Antiretroviral Therapy (ART) compliance, alcohol intake and concomitant medication were reviewed by the study staff. Baseline 2 (week 0: Initiation of treatment): Participants confirmed their willingness to participate in the study and eligibility was confirmed, before participants were randomized to either arm 1 or arm 2. Blood was collected from participants. Participants underwent a targeted physical exam. Participants also completed the World Health Organization Quality of Life—HIV Brief Scale (WHOQOLHIV-BREF), Euro-Qol-5Dimension (EQ-5D) questionnaire, and Profile of MoodStates (POMS) questionnaires before receiving a one week supply of the study medication. Follow-up visits (visit 3–8; week 1 to 10): During the follow-up visits, participants underwent a physical examination, and blood was collected to assess the biological study measures. Study drug and ART compliance was assessed. Adverse effects (AEs) were recorded. Pregnancy test was performed on urine of female participants. The participants completed the WHOQOLHIV-BREF, EQ-5D, and POMS questionnaires (Visit 6) and received the study medication until their next visit. End of the treatment (Visit 9; week 12): At Visit 9, participants underwent a physical examination, and blood was collected to assess the biological study measures. Nasal swab and stool specimens were collected from all study participants and semen was collected from male participants. AEs were recorded. A pregnancy test was performed on urine of female participants. Participants then completed the WHOQOLHIV-BREF, EQ-5D, and POMS questionnaires. Final study visit (Visit 10; week 14): At the final visit, participants underwent a physical examination, and blood was collected to assess the biological study measures. AEs were recorded and ART compliance was assessed. A pregnancy test was performed on urine of female participants.
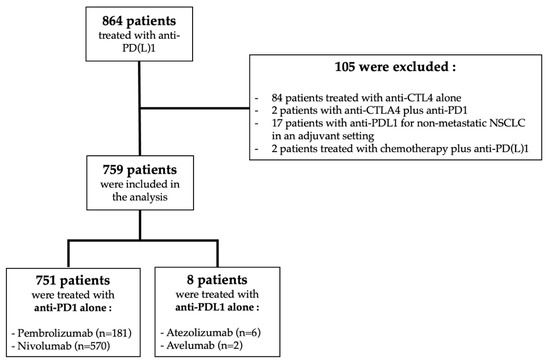
Figure 2. Allocation of participants enrolled in the study (n = 10). Distribution of study participants randomized to arm 1 (TN-TC11M2; THC:CBD) or arm 2 (TN-C200M2; CBD-only), to the study.
Figure 2. Allocation of participants enrolled in the study (n = 10). Distribution of study participants randomized to arm 1 (TN-TC11M2; THC:CBD) or arm 2 (TN-C200M2; CBD-only), to the study.
Figure 3. Daily dosage of CBD-only and THC/CBD combination during the 12 weeks of treatment. (A) THC/CBD arm: In arm 1 (THC/CBD), two participants were able to reach the maximum daily dose of the study drugs (15 mg THC/15 mg CBD), but only one remained at this dose until the end of the treatment, the other participant reduced his dosing to 10 mg THC/10 mg CBD per day because of the occurrence of AEs (somnolence). Two other participants from arm 1 reached the daily dose 10 mg THC/10 mg CBD, but after 3 weeks of treatment, they reduced their dosing because of the occurrence of AEs, one participant experienced cognitive impairment (#102109), while the other had somnolence, fatigue, difficulty concentrating, nightmares and paranoid thoughts (#102101). One remained at 5 mg THC/5 mg CBD per day and the other one who had multiple AEs reduced his daily dose to 2.5 mg THC/2.5 mg CBD after 5 weeks of treatment. A participant (#102110) from arm 1 who first reduced his daily dosing from 5 mg THC/5 mg CBD after 3 weeks of treatment to 2.5 mg THC:2.5 mg CBD, finally increased his dosing from 2.5 mg THC/2.5 mg CBD per day to reach 7.5 mg THC/7.5 mg CBD per day until the end of treatment. (B) CBD arm: 3 participants reached the maximum daily dose of 800 mg CBD after 4 weeks of treatment, but two of them experienced AEs (transient transaminitis for #102107) and SAE (hepatitis with persistent elevated transaminases and worsened diabetes type 2, for #102108) and the treatment was permanently discontinued 1 and 2 weeks after, and they were withdrawn from the study. The other participant who reached the maximum daily dose of 800 mg remained on this daily dose until the end of the study. Finally, two participants from arm 2 gradually increased their daily dosing to reach dose of 400 mg of CBD per day and remained in this range until the end of the study medication.
Figure 3. Daily dosage of CBD-only and THC/CBD combination during the 12 weeks of treatment. (A) THC/CBD arm: In arm 1 (THC/CBD), two participants were able to reach the maximum daily dose of the study drugs (15 mg THC/15 mg CBD), but only one remained at this dose until the end of the treatment, the other participant reduced his dosing to 10 mg THC/10 mg CBD per day because of the occurrence of AEs (somnolence). Two other participants from arm 1 reached the daily dose 10 mg THC/10 mg CBD, but after 3 weeks of treatment, they reduced their dosing because of the occurrence of AEs, one participant experienced cognitive impairment (#102109), while the other had somnolence, fatigue, difficulty concentrating, nightmares and paranoid thoughts (#102101). One remained at 5 mg THC/5 mg CBD per day and the other one who had multiple AEs reduced his daily dose to 2.5 mg THC/2.5 mg CBD after 5 weeks of treatment. A participant (#102110) from arm 1 who first reduced his daily dosing from 5 mg THC/5 mg CBD after 3 weeks of treatment to 2.5 mg THC:2.5 mg CBD, finally increased his dosing from 2.5 mg THC/2.5 mg CBD per day to reach 7.5 mg THC/7.5 mg CBD per day until the end of treatment. (B) CBD arm: 3 participants reached the maximum daily dose of 800 mg CBD after 4 weeks of treatment, but two of them experienced AEs (transient transaminitis for #102107) and SAE (hepatitis with persistent elevated transaminases and worsened diabetes type 2, for #102108) and the treatment was permanently discontinued 1 and 2 weeks after, and they were withdrawn from the study. The other participant who reached the maximum daily dose of 800 mg remained on this daily dose until the end of the study. Finally, two participants from arm 2 gradually increased their daily dosing to reach dose of 400 mg of CBD per day and remained in this range until the end of the study medication.
Figure 4. Dynamics of liver enzymes of participant #102107 and #102108 from arm 2 (TN-C200M2: CBD only), during cannabinoid uptake. Evolution of liver enzyme blood levels in (A). participant #102107 and (B). participant #102108 during the up-titration of CBD dose from the starting of CBD medication to the cessation of the treatment.
Figure 4. Dynamics of liver enzymes of participant #102107 and #102108 from arm 2 (TN-C200M2: CBD only), during cannabinoid uptake. Evolution of liver enzyme blood levels in (A). participant #102107 and (B). participant #102108 during the up-titration of CBD dose from the starting of CBD medication to the cessation of the treatment.
Table 1. Recommended up-titration schedule for TN-TC11M2 and TN-C200M2 regimens.
Table 1. Recommended up-titration schedule for TN-TC11M2 and TN-C200M2 regimens.
Arm 1Table 2. Demographic and biological characteristics of study participants at inclusion (n = 10).
Table 2. Demographic and biological characteristics of study participants at inclusion (n = 10).
TotalTable 3. List of adverse events (AEs) experienced by the participants during the study.
Table 3. List of adverse events (AEs) experienced by the participants during the study.
Adverse EventsTotalTable 4. Liver enzyme and kidney function profiles.
Table 4. Liver enzyme and kidney function profiles.
(Median (IQR))Screening VisitVisit 3Visit 4Visit 5Visit 6Visit 7Visit 8Visit 9p-Value
留言 (0)