
記住我










The eCARE study is the first study implementing a strategy not using a troponin test in patients with chest pain.
The robust stepped-wedge design will ensure applicability of the strategy across numerous centres and provide reliable answers to the objective.
The study highlights safety, with a double safety objective.
By being a diagnostic study, the open-label design was unavoidable, and deviation from the proposed strategy remains possible.
IntroductionChest pain is one of the leading causes of visits to the emergency department (ED) and its diagnosis workup is challenging and time consuming.1 Chest pain may reveal a serious disease, led by acute myocardial infarction (AMI). Ruling out AMI in patients with chest pain is one of the main concerns for emergency physicians. The cornerstones of acute coronary syndrome (ACS) diagnosis are ECG and serial high-sensitivity cardiac troponin measurements.2–4 The diagnostic pathways combining these examinations are very safe to rule out an AMI, and accelerated diagnostic strategies allow prompt discharge from the ED. Until this is proven, all patients presenting with chest pain in the ED are suspected to have an AMI.
To do so, current guidelines recommend performing one or serial troponin measurement(s). However, in current practice, the clinician will, in some patients with chest pain, rule out the hypothesis of an AMI based on their implicit judgement, without any cardiac biomarker measurements. This represents about 20% of patients with chest pain consulting EDs in France.5 This practice was shown to lead to an unacceptable rate of 5% of missed AMIs.6 7 A tool able to identify which patient with chest pain should be investigated for possible AMI or, on the contrary, for whom an AMI could be safely ruled out without further investigations, would be of great help for emergency physicians.
For this purpose, we previously described the HEAR score (History, ECG, Age, Risk factors), a partial history, ECG, age, risk factors, troponin (HEART) score.8 9 In observational studies, the HEAR score exhibited good performances with a very low rate of failure8–10 (figure 1). A patient with a HEAR score below 2 is considered low risk, allowing to rule out an AMI without troponin measurements. Moreover, the HEAR score could be easily combined with the HEART score in a two-step approach: when the HEAR score is ≥2 but the HEART score <4, an AMI can be ruled out with only a single troponin measurement (HEAR-T strategy).11 Observational studies show that more than half of patients presenting to the EDs with chest pain are classified as low risk by the HEAR-T strategy and that these patients have a very low risk of experiencing a major adverse cardiac event (MACE) during the 30-day follow-up (<1%).8 MACE is used because it includes, in addition to AMI, other cardiovascular emergencies that result from atherosclerotic disease and usually present as chest pain.
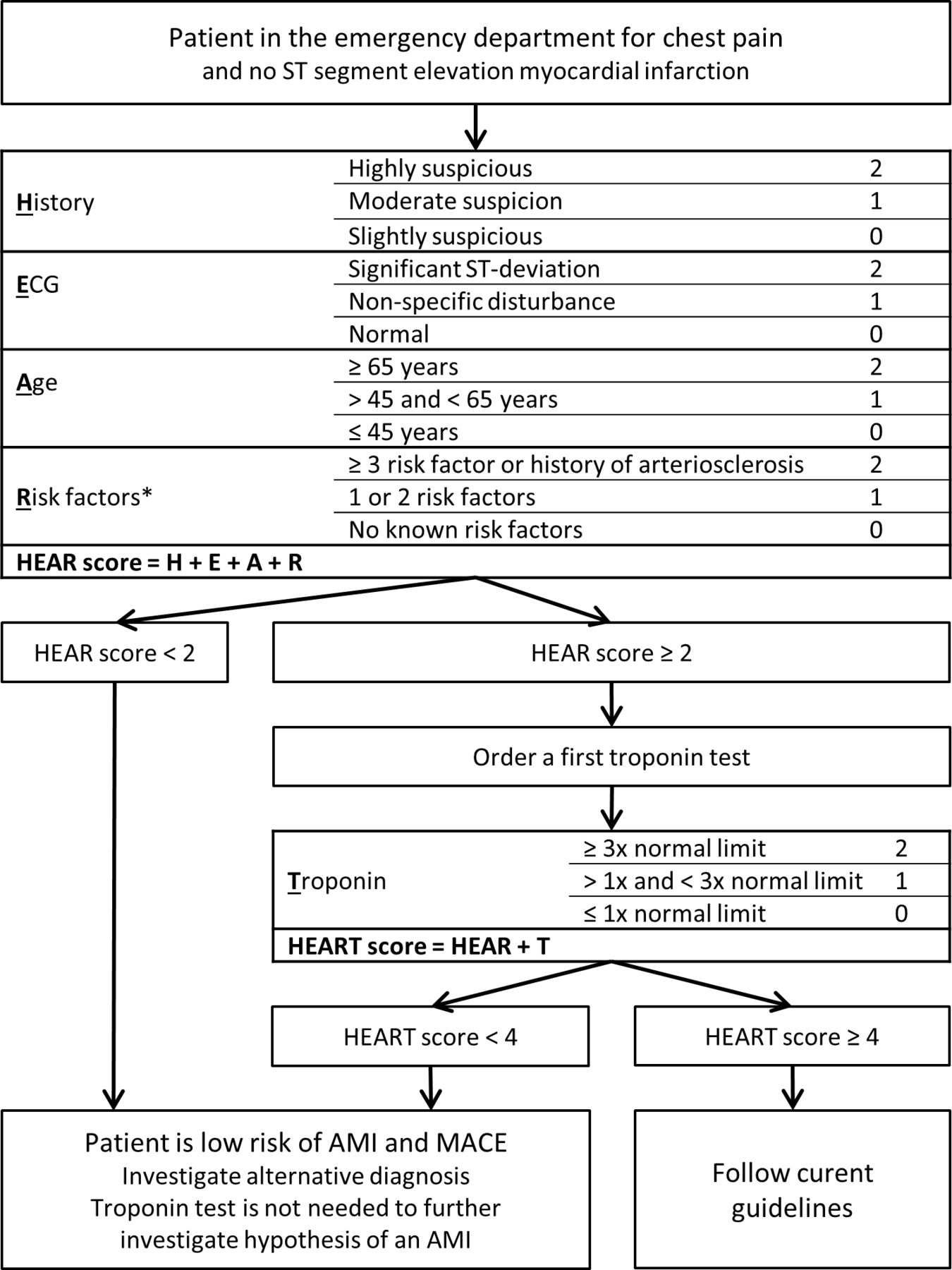 Figure 1
Figure 1 Description of interventional procedure. *Risk factors include: hypercholesterolaemia, hypertension, diabetes mellitus, cigarette smoking, positive family history and obesity. History of atherosclerotic disease includes: coronary vascular disease, stroke, peripheral artery disease and symptomatic carotid artery stenosis. AMI, acute myocardial infarction; HEAR; history, ECG, age, risk factors; HEART, history, ECG, age, risk factors, troponin; MACE, major adverse cardiac event.
Aim and hypothesisWe hypothesise that using the HEAR-T strategy, using a HEAR score in a first step, and a HEART score in a second step, is a safe and effective way of ruling out the hypothesis of an AMI patients with chest pain in the ED.
Our main objective is to prospectively assess the safety of implementing the HEAR-T strategy in ED patients presenting with non-traumatic chest pain to rule out an MACE without a troponin assessment (HEAR score) or a single troponin measurement (HEART score). Our secondary objective is to assess the efficiency of the HEAR-T strategy, in terms of the number of troponin measurements, time spent in the ED and costs.
Methods and analysisStudy designThe eCARE study is an open-label stepped-wedge pragmatic cluster-randomised control trial conducted in 10 EDs in France and Belgium (6 academic and 4 community hospitals). The study’s protocol follows the Standard Protocol Items: Recommendation for Interventional Trials guidance for cluster randomised trials (online supplemental appendix 1). The study started, and the first patient was included on 10 January, 2022. The anticipated inclusion completion date is 9 July 2023, for a study completion date on 9 August 2023.
Trial objectives and outcomesPrimary objective and outcomeThe main objective is to demonstrate the non-inferiority in terms of safety of the HEAR-T strategy in order to rule out an AMI in ED patients presenting with non-traumatic chest pain, as compared with the current recommended strategy. The HEAR-T strategy consists of (1) an assessment of the HEAR score before prescribing a troponin test and, if the HEAR score is≥2, (2) an assessment of the HEART score. An AMI will be ruled out if (1) the HEAR score is <2 (indicating there is no need for a troponin test to further investigate this hypothesis) or (2) if the HEAR score is ≥2 and, on the basis of a troponin test, the HEART score is <4 (indicating there is no need for a second troponin test or other investigation). Other situations are solved using current guidelines (figure 1). The primary outcome is the rate of MACE, combining AMI, percutaneous coronary intervention (PCI), coronary artery bypass graft, survived cardiac arrest, cardiac death or death when a cardiac cause could not be formally dismissed, occurring between hospital discharge and the 30th day following the inclusion. We concentrate on short-term outcomes because the studied strategy aims to identify patients suitable for early ED discharge. Some patients may need further assessments, but the strategy aims to show it could be safely performed as an outpatient, in ambulatory clinics. The need for further assessment remains controversial and is left to the discretion of a consultant or local standard procedures.12
For the same reason, events occurring during the hospital stay of inclusion are considered as appropriately detected by the strategy (right positive in intention-to-diagnose analysis). Therefore, for patients who experience MACEs during the hospital stay of inclusion, any further MACEs occurring during the 30-day follow-up are considered as recurrence rather than a false negative result of the diagnostic strategy and are not taken into account in the main analysis. This definition allows to focus on unexpected events (false negative). The fourth international definition of myocardial infarction is used.13 The two types of AMI, type 1 and type 2, are considered due to challenges in distinguishing them.14 15 PCI is defined as per online supplemental appendix 10-A-5 from Hicks et al.16 Death due to AMI is as defined being a type 3 AMI in the fourth definition of myocardial infarction. Cardiovascular death and undetermined cause of death are defined as per online supplemental appendices 3 and 5 from Hicks et al.13 16 The primary outcome is adjudicated by two independent experts, and a third is requested in case of disagreement.
Secondary objectivesSecondary objectives are hierarchical (see multiple testing section). The first secondary objective is to demonstrate that patients in whom an ACS was ruled out using the HEAR-T strategy are at low risk of MACE to follow-up. This analysis considers any MACE, including those diagnosed during the encounter of the inclusion. The second secondary objective is to demonstrate that the HEAR-T strategy reduces the absolute number of troponin measurements compared with the current recommended strategies. The third secondary objective is to demonstrate that the HEAR-T strategy reduces the length of stay in the ED compared with the current recommended strategies. The fourth and last secondary objective is to demonstrate that the HEAR-T strategy improves resource consumption compared with the current recommended strategies. Global discriminative performances of the HEAR and HEART score will also be compared with reference scores: Thrombosis in myocardial infarction (TIMI) risk score and global registry of acute coronary events (GRACE) score.17 18
Experimental plan for stepped-wedge designIn this stepped-wedge cluster-randomised trial, the 10 participating centres begin the trial in the control phase. Every 1/11th of the total number of patients needed to include in the study, a centre is switched to the interventional phase, so that all centres are in the interventional phase at the end of the trial (figure 2). The order of the switch is randomised by the department of research and innovation of the University Hospital of Angers using a stratified randomisation list on the size of the centre (community or academic). For this purpose, the inclusion rate is monitored, and the dates of the switch are predicted using a linear model regression model. In case of substantial imbalance between the two groups, the date of the next centre switch is postponed without modifying the order of the switch of the centres.
 Figure 2
Figure 2 Stepped-wedge design.
Study settings and populationPatients are included in the study if presenting to a participating ED for non-traumatic chest pain, are over the age of 17 years, have expressed their oral (France) or written (Belgium) consent to participate and have up-to-date health insurance coverage. Criteria for non-inclusion are as follows: (1) 30-day follow-up is not possible; (2) ST-segment elevation myocardial infarction on the ECG at admission; (3) chest pain formally related to another diagnosis other than an ACS before inclusion (ie, pneumothorax, pneumonia, etc); (4) patients having had a troponin test in the last 24 hours; (5) patients referred from other healthcare structure, other than primary care; (6) patients already included in this study and still in their follow-up period; (7) pregnant, breast feeding or parturient patients; (8) patients deprived of liberty by judicial or administrative procedures; (9) patients undergoing forced psychiatric care; (10) patients under legal protection measures and (11) patients unable to give free and informed consent. Patients are excluded from the main analysis if (1) follow-up is impossible or (2) if a component of the HEAR or HEART score is missing, and its potential values may change the risk category of the patient.
Description of the interventionDuring both study periods, patients presenting to the ED for chest pain are assessed for eligibility. Patients meeting all the inclusion criteria and none of the exclusion criteria receive verbal and written information about the study. They are included if they provide consent. The data needed to compute the HEAR, HEART and TIMI risk score for unstable angina are prospectively collected by the consultant, either in a secured electronic case report form (e-CRF) or in a printed version of the CRF.
Control phaseDuring the control phase, no information and a fortiori recommendation about the HEAR-T strategy is provided. The doctors of participating centres are advised to follow current guidelines for managing suspected ACS, including ECG and troponin tests, repeated if needed. The use of 0/3h, 0/2h or 0/1h algorithms is left to the discretion of the consultant.2 3 All centres are enabled with high-sensitivity troponin assays, allowing to measure a troponin level in at least 50% of healthy populations and validated for accelerated diagnostic protocols: Roche Cobas cTnT-hs (n=8), Siemens ADVIA Centaur TNIH (n=1) and Abbott Alinity HS-cTnI (n=1). The doctor in charge is still free to apply the diagnostic strategy they consider the most appropriate for the patient. Similarly, the interpretation of the troponin measurement(s) is left to the discretion of the consultant.
Interventional phaseIn the interventional phase, the HEAR score is calculated and displayed to the doctor via the e-CRF of its printed version (figure 1). If the HEAR scores are 0 or 1, an AMI is ruled out and the consultant is advised not to perform a troponin test and to look for an alternative diagnosis. Nevertheless, the doctor remains free to perform a troponin test for the diagnosis or prognosis assessment of another disease other than an AMI (such as myocarditis or pulmonary embolism). The doctor can also overrule the advised strategy and carry out investigations to rule out an AMI but must report the reason of this strategy deviation. If the HEAR score is 2 or more, the doctor is advised to draw a single troponin test to compute a HEART score. Likewise, patients with a HEART score below 4 are considered a low risk for an AMI and leads to the doctor being advised to do not perform further tests to rule out an AMI. For patients with a HEART score equal to or above 4, the doctor is advised to follow current guidelines, as described in the control phase.
Follow-upThe medical records are checked for possible ED consultation, investigation or hospitalisation during the follow-up period. The number of troponin measurements performed during the first 24 hours of admission is collected, as well as all other investigations performed to diagnose any cardiovascular disease. The patients, their relatives or their general practitioner are interviewed at the end of the 30-day follow-up period to identify possible cardiovascular events. For each possible event during the follow-up, an adjudication file is constituted, including reports of all relevant examinations. All possible events are adjudicated by the independent committee and assessed blind with regard to the times and randomisation arm (control or interventional period).
PragmatismThe purpose of this study is to evaluate an innovative diagnostic strategy that influences decision making to the extent that it will be implemented in routine clinical practice and directly informs clinical decision-making. It is therefore considered as a pragmatic randomised trial and follows the extension of the Consolidated Standards of Reporting Trials statement for pragmatic trials.19–22 The study is rated a score of 36 out of 45 according to the PRECIS-2 guideline, with a score of 0 being a study that is totally explicative, and 45 being a study that is perfectly pragmatic (online supplemental appendix 2). The wide and consistent inclusion criteria, the recruitment procedures, the wide panel of centres represented, the applicability of the procedures and methods used for follow-up matches expectation for a pragmatic study, in terms of eligibility, recruitment, setting organisation, adherence and follow-up. The primary outcome remains rather explicative, but the doctor will remain free to overrule the intervention strategy, as it would have happened in clinical practice. The method to deliver the intervention is still brought by a dedicated material, influencing the flexibility to deliver the intervention.
Patient and public involvementThe study was designed and is conducted without direct public’s or patient’s involvement. The study was reviewed and approved by the ethics committee Ile de France II, whose members include patient representatives.
Statistical analysisDescriptive analysisPopulation characteristics are assessed using the mean and SD for continuous variables with expected Gaussian distribution, or with median and with the IQR. Qualitative variables are reported in proportions and Clopper-Pearson 95% CI for categorical variables. Student’s t-test, the Mann-Whitney U test or Fisher’s exact test are used for the comparison of groups, as appropriate. Diagnostic performances are reported using predictive values, sensitivity, specificity and likelihood ratios with their 95% CI. Statistical analysis is performed using R software, V.4.0.0 (R Core Team, 2018, a language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria). Type-I error rate is set to 5% for all tests. No interim analysis is planned.
Per-protocol and intention-to-diagnose analysesThe analyses are carried out as both per-protocol and intention-to-diagnose. In the per-protocol analysis, the population is classified as if the strategy suggested by the corresponding study phase was strictly applied. This means that all patients having had an appropriately followed 0/3h, 0/2h or 0/1h pathway, as recommended, are considered for the analysis in the control phase.2 3 For the interventional phase, patients with a HEAR score of <2 or patients with a HEAR score of ≥2 and a HEART of <4 are attributed to the low-risk group, and others to the intermediate-high risk group. In the intention-to-diagnose analysis, the population includes all patients in the interventional phase against those included in the control phase, irrespectively of protocol deviations, if any.
Main objectiveIn order to demonstrate the non-inferiority of the study procedure, compared with the control phase, the main analysis is performed as per-protocol analysis, that is, in patients not having had a troponin test to look for an AMI if a HEAR score is <2 and no more than 1 troponin test in patients with a HEART score of <4. Being a safety outcome, this kind of analysis is preferred to challenge the interventional procedure and ensure maximal safety. The difference in MACE rate between discharge and the 30-day follow-up is estimated using a mixed effect logistic regression model with random effect on the cluster and the phase. Polling centres will be considered if the number of inclusions is not sufficient to allow robust estimation of model parameters. No other adjustment variables is added in the model. The covariance matrix is set unstructured. If the model does not fit under this assumption, a compound symmetry structured matrix will be used. The expected failure rate of current diagnostic strategies is low. The non-inferiority margin is set to 1.5%, which appears to be a margin consistent with studies with a similar study design.23–26
Secondary objectivesHierarchical analysis of secondary outcome is conducted to control the risk of multiple testing (see multiple testing section). The first secondary objective is to validate the safety of ruling out an MACE using the HEAR-T strategy. All patients in the interventional phase experiencing an MACE, including those diagnosed during the in-hospital stay following the first ED presentation and inclusion, in whom the HEAR-T strategy suggested to rule out an ACS will be considered false negative of the strategy (per-protocol population). The upper limit of the 95% CI of the false negative rate must be lower than 2.5%, using Clopper-Pearson intervals, with are shown to have good performances for small proportions.27 The next secondary outcomes are efficacy outcomes. An analysis of these objectives is performed in the intention-to-diagnose population and assesses the superiority of the intervention. The second secondary outcome compares the absolute reduction in the number of troponin measurements performed in the first 24 hours of inclusion between the two phases, using a Poisson generalised linear mixed model, with the same strategy for random effect as the principal analysis. The third secondary outcome compares the absolute reduction in ED length of stay, using a Cox proportional hazard model. The proportional hazard assumption is checked graphically and tested on the Schoenfeld residuals. If the proportional hazard is not verified, a landmark approach will be considered. The fourth secondary objective consists of a cost-effectiveness analysis, using MACE, occurring between discharge and 30 days as a health efficacy outcome. The costs considered are all the resources required to carry out the diagnostic strategies, as well as all the consequences directly related to these strategies. Due to differences in costs across countries, it is only performed on the population included in France. The result of the analysis is presented as a differential ratio of cost-effectiveness (differences in cost divided by the differences in effectiveness).28 Performances of the different risk scores will be compared using area under the receiver operating curve and tested with the Delong-Delong test.29
Sensitivity analysesIn a first sensitivity analysis, the definition of MACE is extended with ACS. It increases the sensitivity for adverse outcomes, even if it lacks reproducibility and remains of limited impact if patients do not experience a MACE. An intention-to-diagnose analysis is performed for primary and first secondary objectives. A ‘worst-case scenario’ analysis is also conducted for both of these objectives, considering all patients lost to follow-up as if they had experienced an MACE. Per-protocol analysis is performed for other secondary analyses.
Missing dataNo imputation of missing data is planned. Monitoring and CRF are designed to minimise missing data. A patient is not excluded from analysis if a component of the HEAR or HEART score is missing, and its potential values do not change his or her risk category (ie, a patient with a HEAR score of 4 is already not in a low-risk category even if no troponin result is available to compute the HEART score). However, missing data are analysed to determine whether it is informative and whether it is likely to lead to potential selection or information bias. The potential impact of these biases will be discussed in the final paper.
Multiple testingA hierarchical analysis of secondary outcome is conducted, so that no correction for multiple testing is required. This means than secondary outcomes are interpreted only if the main criterion and the preceding secondary objectives (if any) reached statistical significance.
Sample size calculationThe sample size is estimated to provide an accurate estimation of our primary outcome. We assume a maximal event rate of MACE at 1.5% of modern diagnostic strategies. In an individually randomised study, 812 patients per randomisation arm would be required, considering equivalent missed rates of MACE and a non-inferiority margin of 1.5% and a power of 80%. An increase by a factor of 1.11 is required due to the clustered design, considering the 10 centres and a 0.0014 intracentre correlation coefficient, based on previous studies.30 Considering a 10% incidence rate of MACE diagnoses during first ED admission and a 5% rate of lost to follow-up, a total of 2080 patients (1040 per arm) is required for the study across the 10 centres.31
Ethics and disseminationInformed consent is obtained for all patients and an information letter is provided to all participants. As per regulations, signed consent is obtained for patients included in Belgium, and verbal consent for patients included in France. Participation to the study protocol is recorded in a medical chart. An institutional review board has approved the study (Comité de Protection des Personnes Ile de France II, no 2019-A02265-52) for all participating centres and authorisation was granted by the ethics committee of the participating hospital in Belgium (Comité d’éthique hôpital-facultaire Saint Luc, no 2020/16JUL/372). The results of the study will be published in peer-reviewed journals and will be presented in conferences.
DiscussionTo the best of our knowledge, this study is the first to implement a diagnostic strategy allowing to forgo blood tests in patients with chest pain. This study will fill the gap between recommendations and clinical practice. Guidelines recommends to timely perform a troponin test in all patients. Whereas in clinical practices, we noticed that one-fifth of patients do not have a single troponin measured. The question of very low-risk chest pain in patients is rarely studied. Indeed, most diagnostic studies use suspected ACS as main inclusion criteria, so that low-risk patients are omitted from those studies. It was however shown that low-risk patients, even when considered being ‘definitely not an ACS’ based on clinical judgement and ECG, have a substantial risk of experiencing adverse outcomes.
This study will provide answers to a daily problem encountered by emergency physicians. In case of conclusive results, it will enable emergency physicians to perform timely triage of patients with chest pain, where some are suspected to have an AMI and follow dedicated pathways to diagnose this life-threatening situation, and others where the hypothesis of an AMI is very unlikely and should be preferably investigated for an alternative diagnosis. The HEAR score is a very useful tool for emergency physician. It is easy to learn and does not require a calculator to be computed.
The study provides a robust design, enabling to directly change current clinical practices. The clustered study design is chosen in order to diminish the risk of contamination of the procedures as compared with individual randomisation or a cross-over design. The use of the HEAR-T strategy will popularise the validated HEART score, which is not used across participating centres and is likely to change current practices. The use of a comparison group is important to measure the impact of the strategy in clinical practice. The potential impact of the strategy was already assessed, but it was only estimated from retrospective or observational studies. The acceptability from doctors working in the ED and patients remains to be demonstrated. The stepped-wedge design, as opposed to a classic cluster-randomised trial, allows to (1) assess the effect and acceptability of the intervention across all centres; (2) reduce the period and centre effect; and (3) works well for crowded EDs. The stepped-wedge design is a robust and widely accepted design for implementation of diagnostic strategies.32 33 It does not allow blinding, but as a matter of fact, blinding is not even possible for this kind of diagnostic study. Using MACE as a primary endpoint is a tried and tested outcome to benchmark ACS. The per-protocol analysis of the safety outcomes challenges the strategy beyond what would have happened in clinical practice. The stepped-wedge design provides confidence in the acceptability of the strategy from emergency physicians, and the randomised design enables direct comparison to current clinical practices.
Ethics statementsPatient consent for publicationAcknowledgmentsWe would like to thank the Groupement Interrégional pour la recherche Clinique du Grand Ouest (GIRCI-GO) and the HUGO network for funding the study. We also wish to thank Ms. Béatrice Gable, Ms. Cindy Augereau, Ms. Chloé Ragueneau, Ms. Barbara Maquin, Ms. Nadia Ben Rabah and Ms. Sandra Merzeau for coordinating the project. We thank the department of Innovation and research of the University Hospital of Angers for its contribution. We thank Mr. Jean-Marie Chrétien for coordinating the development of the eCRF and the data management. We finally wish to thank the participating centres for their involvement in the study: department of emergency medicine of the University Hospital of Angers, department of emergency medicine of the university clinics of Saint-Luc, department of emergency medicine of the University Hospital of Tours, department of emergency medicine of the University Hospital of Toulouse, emergency medicine of Le Mans Hospital, emergency medicine of Cholet Hospital, department of emergency medicine of the University Hospital of Liege, emergency medicine of Saint-Brieuc Hospital, emergency medicine of Saint Malo Hospital and emergency medicine of Vendée Hospital.
留言 (0)